Download as pdf or txt
You might also like
- Inclusion-Exclusion Criteria - SynAct-CS002 BaselineDocument4 pagesInclusion-Exclusion Criteria - SynAct-CS002 Baselineadriana gutanuNo ratings yet
- Form Vaksin BVMDDocument2 pagesForm Vaksin BVMDairusmayantiNo ratings yet
- MFAGDocument170 pagesMFAGpcatruongNo ratings yet
- Food Poisoning Investigation Form Version 3 - 0 - 0Document10 pagesFood Poisoning Investigation Form Version 3 - 0 - 0shahanaa AR100% (1)
- Form 4. TX Ipt Card v061416Document2 pagesForm 4. TX Ipt Card v061416Emmanuel GorresNo ratings yet
- Physical Exam Form Nurse AssistantDocument2 pagesPhysical Exam Form Nurse AssistantHawaiiHealthCareNo ratings yet
- Encyclopedia of Metagenomics 2015 PDFDocument766 pagesEncyclopedia of Metagenomics 2015 PDFJordan RuizNo ratings yet
- CDC Covid-19 Report FormDocument2 pagesCDC Covid-19 Report FormiggybauNo ratings yet
- Cif Zika - 2016 PDFDocument3 pagesCif Zika - 2016 PDFNicholai CabadduNo ratings yet
- Student Health Record PDFDocument2 pagesStudent Health Record PDFailen joy villoNo ratings yet
- Cif NTDocument2 pagesCif NTIvy marie BonNo ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- Impact of Bacterial Infections On Chemotherapy-Induced Neutropenia in Cancer PatientsDocument3 pagesImpact of Bacterial Infections On Chemotherapy-Induced Neutropenia in Cancer Patientsshamsi saad shamsiNo ratings yet
- Prenatal Nutrition and Immunization: Demographics OB HistoryDocument19 pagesPrenatal Nutrition and Immunization: Demographics OB HistorynivraeNo ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Lindo Gondales Jr.No ratings yet
- Part I - Statement by The Candidate: Edical Ertificate FOR PpointmentDocument2 pagesPart I - Statement by The Candidate: Edical Ertificate FOR Ppointmentravi ranaNo ratings yet
- MedicalDocument2 pagesMedicalChris HutchinsonNo ratings yet
- Statistical Report 4th Quarter 2007Document5 pagesStatistical Report 4th Quarter 2007api-3836762No ratings yet
- Pediatric History OutlineDocument12 pagesPediatric History OutlineDawn MarcoNo ratings yet
- Case Study IcuDocument31 pagesCase Study Icujanna mae patriarcaNo ratings yet
- Barangay Assisted Booking Form: CODE: D1ADocument4 pagesBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNo ratings yet
- 8.) Health-and-Medical-Profile Template Ver.2Document4 pages8.) Health-and-Medical-Profile Template Ver.2SocialWelfare SilangNo ratings yet
- Animal Bite Treatment RecordDocument2 pagesAnimal Bite Treatment RecordDariel Baculbas AlvarezNo ratings yet
- TB or NOT TB - Data Collection - DraftDocument2 pagesTB or NOT TB - Data Collection - DraftPeter Glenn ChuaNo ratings yet
- Survey QuestionnairesDocument1 pageSurvey QuestionnairesDarianne B. BasaNo ratings yet
- N.202-Introduction To Nursing Practice Health Assessment ToolDocument9 pagesN.202-Introduction To Nursing Practice Health Assessment ToolmNo ratings yet
- JOVIE ANN DOBLON - Copy of NCAR OB NCM 109Document16 pagesJOVIE ANN DOBLON - Copy of NCAR OB NCM 109Jannarie EstebanNo ratings yet
- FP Form1 V3.0 2016Document3 pagesFP Form1 V3.0 2016Lorenz Joey Ricarte100% (2)
- CIF-MR 2022 Ver1Document2 pagesCIF-MR 2022 Ver1Ivy marie BonNo ratings yet
- Medical Status Form - Mt. Sinai PDFDocument1 pageMedical Status Form - Mt. Sinai PDFJennifer LeeNo ratings yet
- Teacher's Health cardSHD-AnnualPE-TeachingNonTeachingDocument4 pagesTeacher's Health cardSHD-AnnualPE-TeachingNonTeachingJudy Ann CruzNo ratings yet
- Statform3: Republic of The Philippines Department of Health ManilaDocument10 pagesStatform3: Republic of The Philippines Department of Health ManilaErica WareNo ratings yet
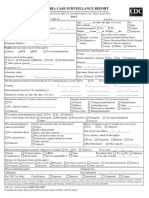
- Malaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)Document2 pagesMalaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)Pramod gameNo ratings yet
- Human Immunodeficiency Virus: Transmission of HIVDocument15 pagesHuman Immunodeficiency Virus: Transmission of HIVdlneisha61No ratings yet
- Anadjah Ebrahim MCDocument1 pageAnadjah Ebrahim MCMusaiden EbrahimNo ratings yet
- Suspected Side EffectsDocument2 pagesSuspected Side EffectsImmah PinedaNo ratings yet
- Patient History and Consent Form For Maternal Serum Testing (Mandatory)Document1 pagePatient History and Consent Form For Maternal Serum Testing (Mandatory)Akhil ChawlaNo ratings yet
- FDA Phils-Suspected-Side-Effects-Reporting-Form-v6.0Document3 pagesFDA Phils-Suspected-Side-Effects-Reporting-Form-v6.0Marizel PormilosNo ratings yet
- Nursing Care Analysis RecordDocument16 pagesNursing Care Analysis RecordJannarie EstebanNo ratings yet
- Covid-19 Visitors DeclarationDocument1 pageCovid-19 Visitors Declarationvp_s4460No ratings yet
- Aily Equirements: Case: Patient With Tuberculosis General Objectives (5pts)Document31 pagesAily Equirements: Case: Patient With Tuberculosis General Objectives (5pts)janna mae patriarcaNo ratings yet
- Cuidados Posoperatorio CirugiaDocument1 pageCuidados Posoperatorio CirugiaAna CristernaNo ratings yet
- Admission LetterDocument17 pagesAdmission LettermarkochikongoyeNo ratings yet
- COVID-19 (Coronavirus) Exposure Questionnaire For Health Care WorkersDocument3 pagesCOVID-19 (Coronavirus) Exposure Questionnaire For Health Care WorkersDixit SushmithaNo ratings yet
- Oil and Natural Gas Corporation LTD Self Declaration On Medical StatusDocument4 pagesOil and Natural Gas Corporation LTD Self Declaration On Medical StatusDodiya NikunjNo ratings yet
- Case 4 - MCNP - Miguel, Mark Darren, T.Document3 pagesCase 4 - MCNP - Miguel, Mark Darren, T.markNo ratings yet
- Application FormDocument5 pagesApplication Formapi-603319031No ratings yet
- PEDO Forms To PrintDocument4 pagesPEDO Forms To PrintMONIQUE QUIMZONNo ratings yet
- GordonsDocument2 pagesGordonsAngelica OctotNo ratings yet
- Health FormsDocument9 pagesHealth Formserika luna romanNo ratings yet
- Center For Diabetes CareDocument8 pagesCenter For Diabetes CareKareen AdvinculaNo ratings yet
- ReportForm TyphoidDocument2 pagesReportForm TyphoidSundarajan ManiNo ratings yet
- Questionnaire To Find Demographic and Clinical Characteristics of Patients With Cerebral Palsy at Shaikh Zayed HospitalDocument2 pagesQuestionnaire To Find Demographic and Clinical Characteristics of Patients With Cerebral Palsy at Shaikh Zayed HospitalZenabNaazNo ratings yet
- Ryans Care Plan AssignmentDocument12 pagesRyans Care Plan Assignmenttaylor.alveyNo ratings yet
- ISARIC COVID-19 CRF V1.3 24feb2020Document12 pagesISARIC COVID-19 CRF V1.3 24feb2020ARINTA DWI KOMALANo ratings yet
- Annual Medical Report Form Annapolis - Ho 2020Document10 pagesAnnual Medical Report Form Annapolis - Ho 2020Melissa DavidNo ratings yet
- Family Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingDocument4 pagesFamily Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- MORTALITY AUDIT FORM FOR HIV - TB - HEI CLIENTS Final VersionDocument12 pagesMORTALITY AUDIT FORM FOR HIV - TB - HEI CLIENTS Final VersionMigori ArtNo ratings yet
- Health Card TeachersDocument3 pagesHealth Card TeachersRuselle N. NavarroNo ratings yet
- HRN: Julia Salazar Hospital: - Clinical Instructor: MRS. JUNELYN TAGARDA Date: 2/12/22 - Shift: AM Area: Ob WardDocument15 pagesHRN: Julia Salazar Hospital: - Clinical Instructor: MRS. JUNELYN TAGARDA Date: 2/12/22 - Shift: AM Area: Ob WardShirley L. CarumbaNo ratings yet
- World Health Organization STRATEGY (2022-2026) : For The National Action Plan For Health SecurityDocument17 pagesWorld Health Organization STRATEGY (2022-2026) : For The National Action Plan For Health SecuritynavenNo ratings yet
- Improving The Collection and Use of Administrative Data On Violence Against WomenDocument77 pagesImproving The Collection and Use of Administrative Data On Violence Against WomennavenNo ratings yet
- Building An NCD-ready Workforce: Technical Meeting ReportDocument48 pagesBuilding An NCD-ready Workforce: Technical Meeting ReportnavenNo ratings yet
- Strengthening The Collection, Analysis and Use of Health Workforce Data and InformationDocument348 pagesStrengthening The Collection, Analysis and Use of Health Workforce Data and InformationnavenNo ratings yet
- PHYS295 Response 5Document5 pagesPHYS295 Response 5navenNo ratings yet
- Seventeenth Meeting of The WHO Vector Control Advisory GroupDocument38 pagesSeventeenth Meeting of The WHO Vector Control Advisory GroupnavenNo ratings yet
- PHYS295 Lab 6Document6 pagesPHYS295 Lab 6navenNo ratings yet
- Preventing Injuries and Violence: An Overview: Key FactsDocument14 pagesPreventing Injuries and Violence: An Overview: Key FactsnavenNo ratings yet
- PHYS295 Worksheet 3Document4 pagesPHYS295 Worksheet 3navenNo ratings yet
- Abortion Care Guideline ExecutiveDocument20 pagesAbortion Care Guideline ExecutivenavenNo ratings yet
- National Workforce Capacity To Implement The Essential Public Health Functions Including A Focus On Emergency Preparedness and ResponseDocument26 pagesNational Workforce Capacity To Implement The Essential Public Health Functions Including A Focus On Emergency Preparedness and ResponsenavenNo ratings yet
- PHYS295 Review 2Document5 pagesPHYS295 Review 2navenNo ratings yet
- PHYS295 Demonstration 10Document5 pagesPHYS295 Demonstration 10navenNo ratings yet
- 2 JKA 319E What Is A Research ProposalDocument13 pages2 JKA 319E What Is A Research ProposalnavenNo ratings yet
- WHO SRH 21.17 EngDocument6 pagesWHO SRH 21.17 EngnavenNo ratings yet
- Towards A Supportive Law and Policy Environment For Quality Abortion Care: Evidence BriefDocument16 pagesTowards A Supportive Law and Policy Environment For Quality Abortion Care: Evidence BriefnavenNo ratings yet
- PHYS295 Demonstration 1Document5 pagesPHYS295 Demonstration 1navenNo ratings yet
- Global Atlas of Medical Devices: A1B2 C3D4Document608 pagesGlobal Atlas of Medical Devices: A1B2 C3D4navenNo ratings yet
- 1 JKA 319E Course IntroductionDocument11 pages1 JKA 319E Course IntroductionnavenNo ratings yet
- EngDocument17 pagesEngnavenNo ratings yet
- The Use of Stems in The Selection of International Nonproprietary Names (INN) For Pharmaceutical SubstancesDocument7 pagesThe Use of Stems in The Selection of International Nonproprietary Names (INN) For Pharmaceutical SubstancesnavenNo ratings yet
- Drug OverdoseDocument12 pagesDrug OverdosenavenNo ratings yet
- WHO Consolidated On Tuberculosis: GuidelinesDocument128 pagesWHO Consolidated On Tuberculosis: GuidelinesnavenNo ratings yet
- Ophthalmology Emergencies - 2Document32 pagesOphthalmology Emergencies - 2navenNo ratings yet
- Approach To Child With Fever: Liew Qian YiDocument33 pagesApproach To Child With Fever: Liew Qian YinavenNo ratings yet
- Mock Drill Disaster Exercise Hospital Evaluation Form: Name of Evaluator: DesignationDocument1 pageMock Drill Disaster Exercise Hospital Evaluation Form: Name of Evaluator: DesignationnavenNo ratings yet
- Emergency Wound Management - BebDocument26 pagesEmergency Wound Management - BebnavenNo ratings yet
- ECG Changes in ACSDocument39 pagesECG Changes in ACSnavenNo ratings yet
- Disaster Preparedness EvaluationDocument2 pagesDisaster Preparedness EvaluationnavenNo ratings yet
- Tetanus and Rabies FinalDocument23 pagesTetanus and Rabies FinalnavenNo ratings yet
- Causes and Prevention of DiseasesDocument4 pagesCauses and Prevention of DiseasesSusan Hepzi100% (1)
- Computer Vision-Based Plant Disease Identification System A Review PDFDocument20 pagesComputer Vision-Based Plant Disease Identification System A Review PDFarjun105flashNo ratings yet
- Biology Notes by Vasumitra GajbhiyeDocument59 pagesBiology Notes by Vasumitra GajbhiyeketamineNo ratings yet
- Uk Plummer VinsonSyndrome2005Document5 pagesUk Plummer VinsonSyndrome2005darsunaddictedNo ratings yet
- Effect of Temperature On Crop ProductionDocument14 pagesEffect of Temperature On Crop ProductionKashif Akram100% (1)
- Case Study Analysis On Beximco Private Limited and Its Product Napa Paracetamol-Caffeine TabletDocument23 pagesCase Study Analysis On Beximco Private Limited and Its Product Napa Paracetamol-Caffeine Tabletamrin jannat0% (1)
- Waterways Summer 2013Document76 pagesWaterways Summer 2013Waterways MagazineNo ratings yet
- Neruo JournalDocument2 pagesNeruo JournalShewit AbrahamNo ratings yet
- Artificial Intelligence For Mental Health and Mental Illnesses: An OverviewDocument18 pagesArtificial Intelligence For Mental Health and Mental Illnesses: An OverviewnamaNo ratings yet
- Central Depressive Effect (Pentobarbital and Carbromal) : CarbritalDocument3 pagesCentral Depressive Effect (Pentobarbital and Carbromal) : Carbritalnisarg bipinchandraNo ratings yet
- Gamma World GM ScreenDocument14 pagesGamma World GM ScreenThe Lyon100% (7)
- First Level Assessment (SAMPLE)Document2 pagesFirst Level Assessment (SAMPLE)Cooby Gempesaw100% (1)
- Calorimetría Indirecta EsencialDocument12 pagesCalorimetría Indirecta EsencialPaulina ToledoNo ratings yet
- Acupressure Study Guidev2Document25 pagesAcupressure Study Guidev2mrruupeeNo ratings yet
- Inspiring With Cystic FibrosisDocument2 pagesInspiring With Cystic FibrosisBeverlyHillsWeeklyNo ratings yet
- What Is Radioactive PollutionDocument4 pagesWhat Is Radioactive PollutionJoy MitraNo ratings yet
- Effect of Chronic Low Back Pain On Lumbar Spine Lordosis During Sit-to-Stand and Stand-to-SitDocument14 pagesEffect of Chronic Low Back Pain On Lumbar Spine Lordosis During Sit-to-Stand and Stand-to-SitVictor CristianNo ratings yet
- Case Based DiscussionDocument35 pagesCase Based DiscussionDenaya Tika ReskiaNo ratings yet
- Np3 Recalls 4Document9 pagesNp3 Recalls 4AhrisJeannine EscuadroNo ratings yet
- A Case Study On Hypertensive Urgency - Group 2 Section 3BDocument48 pagesA Case Study On Hypertensive Urgency - Group 2 Section 3BhernandezmarianneroseNo ratings yet
- Breath Biopsy Complete GuideDocument110 pagesBreath Biopsy Complete Guidemadimadi11No ratings yet
- Prof BSP - Neurologic Paraneoplastic SyndromesDocument122 pagesProf BSP - Neurologic Paraneoplastic SyndromesSavitha BasriNo ratings yet
- 12 Marker-Assisted Selection LecDocument34 pages12 Marker-Assisted Selection Lecvijjumandula0% (1)
- Test 5Document12 pagesTest 5Minh Anh NguyễnNo ratings yet
- NCP ConstipationDocument3 pagesNCP ConstipationNika LoNo ratings yet
- 20-02-2023 Hand Written NotesDocument21 pages20-02-2023 Hand Written NotesKratos KingNo ratings yet
- Probiotic Efficiency of Spirulina Platensis - Stimulating Growth of Lactic Acid BacteriaDocument4 pagesProbiotic Efficiency of Spirulina Platensis - Stimulating Growth of Lactic Acid BacteriastanleystNo ratings yet
- 3 Apply OSH Practices in A CBT &ADocument78 pages3 Apply OSH Practices in A CBT &ARabiul AwalNo ratings yet