Download as pdf or txt
You might also like
- State of Content Marketing 2023Document126 pagesState of Content Marketing 2023pavan teja100% (1)
- Airway ManagementDocument13 pagesAirway ManagementAlaa DaoudNo ratings yet
- Chapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction SyndromeDocument8 pagesChapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction SyndromejefrocNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Fluids and ElectrolytesDocument69 pagesFluids and ElectrolytesHarold DiasanaNo ratings yet
- Oxygen Therapy: By: Melanie S. Cambel, MAN RNDocument21 pagesOxygen Therapy: By: Melanie S. Cambel, MAN RNGeraldine MaeNo ratings yet
- Suctioning TracheaDocument24 pagesSuctioning Trachealuis_chubee100% (1)
- Med Surg MidtermDocument17 pagesMed Surg Midtermjhan grabierNo ratings yet
- Barangay Health Governance Body 2018Document44 pagesBarangay Health Governance Body 2018Donna Lei G. RosarioNo ratings yet
- Pneumonia and BronchiolitisDocument48 pagesPneumonia and Bronchiolitisshashank panwarNo ratings yet
- Respiration 16 Respiratory FailureDocument31 pagesRespiration 16 Respiratory Failureapi-19641337No ratings yet
- Drugs in ObstetricsDocument95 pagesDrugs in ObstetricsPriya jNo ratings yet
- Bleeding DisordersDocument24 pagesBleeding Disorderskholoud220No ratings yet
- Congenital Heart Disease: Thoracic Conference Frank Nami, M.DDocument49 pagesCongenital Heart Disease: Thoracic Conference Frank Nami, M.DMarie CrystallineNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia Gravisdmnd_cdNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- Cardiovascular Disorders 1Document44 pagesCardiovascular Disorders 1Nader Smadi100% (1)
- Basic Respiratory Mechanics (DR Arif)Document36 pagesBasic Respiratory Mechanics (DR Arif)Rizqi Luqmanul HakimNo ratings yet
- Hypovolemic ShockDocument25 pagesHypovolemic ShockManushi HenadeeraNo ratings yet
- Fluids and ElectrolytesDocument192 pagesFluids and ElectrolytesTeodora JoghiuNo ratings yet
- Congenital Heart DiseaseDocument38 pagesCongenital Heart DiseaseSnIP StandredNo ratings yet
- IntubationDocument41 pagesIntubationNice YouNo ratings yet
- Pneumonia: DefinitionDocument5 pagesPneumonia: DefinitionhemaanandhyNo ratings yet
- BCLSDocument25 pagesBCLSikram ullah khanNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Cardiac FailureDocument63 pagesCardiac FailureNina OaipNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- Dka Vs Hhs Edit 1Document25 pagesDka Vs Hhs Edit 1Razeen RiyasatNo ratings yet
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 pagesMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanNo ratings yet
- Asthma and CopdDocument44 pagesAsthma and CopdBeer Dilacshe100% (1)
- Types of InhalersDocument23 pagesTypes of Inhalersshamie1110No ratings yet
- Noninvasive VentilationDocument6 pagesNoninvasive VentilationEma MagfirahNo ratings yet
- Cerebrovascular Accident/Stroke: Rodney R. Reyes, RNDocument51 pagesCerebrovascular Accident/Stroke: Rodney R. Reyes, RNRodney ReyesNo ratings yet
- Respiratory System Diagnostic ProcedureDocument26 pagesRespiratory System Diagnostic Procedurejefroc75% (4)
- Pulmonary PathoPhysiologyDocument45 pagesPulmonary PathoPhysiologySuliman Garalleh100% (1)
- Asthma (Reactive Airway Disease)Document33 pagesAsthma (Reactive Airway Disease)anwar jabariNo ratings yet
- Bronchitis 170709131740Document28 pagesBronchitis 170709131740Viji MNo ratings yet
- General Anesthetic.: Presented by Jayesh Doke (S.Y B Pharm) S.G.D.C.P, JalgaonDocument54 pagesGeneral Anesthetic.: Presented by Jayesh Doke (S.Y B Pharm) S.G.D.C.P, JalgaonJayesh DokeNo ratings yet
- ShockDocument63 pagesShockAhmedNo ratings yet
- Hepatic Encephalopathy and ComaDocument19 pagesHepatic Encephalopathy and ComaJas Castro JoveroNo ratings yet
- Status EpilepticusDocument28 pagesStatus EpilepticusDaniel AlfredNo ratings yet
- Management of ArrhythmiasDocument4 pagesManagement of ArrhythmiasAray Al-AfiqahNo ratings yet
- Mechanical Ventilation 8.2.17Document41 pagesMechanical Ventilation 8.2.17SyafiqAziziNo ratings yet
- PericarditisDocument19 pagesPericarditisxmitchxNo ratings yet
- Neonatal Transition: Training of The Trainers Neonatal ResuscitationDocument36 pagesNeonatal Transition: Training of The Trainers Neonatal ResuscitationmitaNo ratings yet
- Umbilical Artery CatheterizationDocument11 pagesUmbilical Artery CatheterizationRhaq Sheldon-CoelhoNo ratings yet
- Antiretroviral Therapy: Awlachew Firde (S.Pharmacist)Document40 pagesAntiretroviral Therapy: Awlachew Firde (S.Pharmacist)wedajoyonas50No ratings yet
- Lung Abscess - Lecture 2015Document19 pagesLung Abscess - Lecture 2015Okta Dwi Kusuma AyuNo ratings yet
- Anemia Anemia Describes The Condition in Which The Number of Red Blood Cells in The Blood Is Low. Probability & StatisticsDocument7 pagesAnemia Anemia Describes The Condition in Which The Number of Red Blood Cells in The Blood Is Low. Probability & StatisticsSahara GalayNo ratings yet
- High Risk Newborn2Document15 pagesHigh Risk Newborn2Catherine Villanueva Sta Monica100% (1)
- Procedural Sedation in EDDocument41 pagesProcedural Sedation in EDadam NoheNo ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- Diagnosis of ShockDocument9 pagesDiagnosis of ShockRejina RavindranNo ratings yet
- By: Jacqueline I. Esmundo, R.N.MNDocument32 pagesBy: Jacqueline I. Esmundo, R.N.MNdomlhynNo ratings yet
- Vital Signs-Temp, PRDocument54 pagesVital Signs-Temp, PRmags_abad09No ratings yet
- The Cardiovascular SystemDocument5 pagesThe Cardiovascular Systemjuly3ciaNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- Lung AuscultationDocument62 pagesLung AuscultationOlea CroitorNo ratings yet
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 pagesLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANo ratings yet
- Nursing Management of Mechanically Ventilated PatientsDocument179 pagesNursing Management of Mechanically Ventilated PatientsSourabh AlawaNo ratings yet
- Acid Base ImbalanceDocument28 pagesAcid Base ImbalanceJean Gwyneth GatchalianNo ratings yet
- Nov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Document79 pagesNov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Jean Gwyneth GatchalianNo ratings yet
- Nov 19 SEXUALLY-TRANSMITTED-DISEASE-part-1Document48 pagesNov 19 SEXUALLY-TRANSMITTED-DISEASE-part-1Jean Gwyneth Gatchalian100% (1)
- Nov 19 SEXUALLY-TRANSMITTED-DISEASE-part-2Document53 pagesNov 19 SEXUALLY-TRANSMITTED-DISEASE-part-2Jean Gwyneth GatchalianNo ratings yet
- Industrial Security ConceptDocument85 pagesIndustrial Security ConceptJonathanKelly Bitonga BargasoNo ratings yet
- Tugas Tutorial 2 - English Morpho-SyntaxDocument2 pagesTugas Tutorial 2 - English Morpho-Syntaxlotus373No ratings yet
- ANC 103rd Birthday Transport PlanDocument6 pagesANC 103rd Birthday Transport PlanCityPressNo ratings yet
- Sur MBL - Kmtcpusg482545Document2 pagesSur MBL - Kmtcpusg482545nanaNo ratings yet
- 662-Article Text-4087-1-10-20210104Document23 pages662-Article Text-4087-1-10-20210104Pambudi EzNo ratings yet
- Economics PaperDocument4 pagesEconomics PaperAyesha KhanNo ratings yet
- Certificate of Registration Buisness-Paula LawekDocument2 pagesCertificate of Registration Buisness-Paula LawekAmanda HernandezNo ratings yet
- Accounting 1 Module 3Document20 pagesAccounting 1 Module 3Rose Marie Recorte100% (1)
- Parental Involvement and Their Impact On Reading English of Students Among The Rural School in MalaysiaDocument8 pagesParental Involvement and Their Impact On Reading English of Students Among The Rural School in MalaysiaM-Hazmir HamzahNo ratings yet
- The Forgotten Legion Raetia PDFDocument32 pagesThe Forgotten Legion Raetia PDFFrida HorvathNo ratings yet
- UntitledDocument18 pagesUntitledjeralyn juditNo ratings yet
- Bpme1013 Group B Introduction To Entrepreneurship (Full)Document27 pagesBpme1013 Group B Introduction To Entrepreneurship (Full)Randa RamadhanNo ratings yet
- Financial Analysis of Pakistan State Oil For The Period July 2017-June 2020Document25 pagesFinancial Analysis of Pakistan State Oil For The Period July 2017-June 2020Adil IqbalNo ratings yet
- Law of Succession CATDocument11 pagesLaw of Succession CATSancho SanchezNo ratings yet
- De Thi Giua Ki 2 Tieng Anh 8 Global Success de So 2Document21 pagesDe Thi Giua Ki 2 Tieng Anh 8 Global Success de So 2mit maiNo ratings yet
- Education USADocument35 pagesEducation USAPierrecassanNo ratings yet
- MTC Routes: Route StartDocument188 pagesMTC Routes: Route StartNikhil NandeeshNo ratings yet
- Winning The Easy GameDocument18 pagesWinning The Easy GameLeonardo PiovesanNo ratings yet
- PETROJET General Corporate ProfileDocument19 pagesPETROJET General Corporate ProfileOsama KashkoushaNo ratings yet
- NV jss1Document4 pagesNV jss1Samson Oluwafemi oNo ratings yet
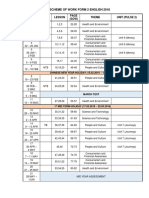
- Scheme of Work Form 2 English 2018: Week Types Lesson (SOW) Theme Unit (Pulse 2)Document2 pagesScheme of Work Form 2 English 2018: Week Types Lesson (SOW) Theme Unit (Pulse 2)Subramaniam Periannan100% (2)
- To Canadian Horse Defence Coalition Releases DraftDocument52 pagesTo Canadian Horse Defence Coalition Releases DraftHeather Clemenceau100% (1)
- Tom Swiss Weekly Mayoral PollDocument5 pagesTom Swiss Weekly Mayoral PollThe Daily LineNo ratings yet
- Designation - Supply OfficerDocument3 pagesDesignation - Supply OfficerShirley P. SumugatNo ratings yet
- SV - ComplaintDocument72 pagesSV - ComplaintĐỗ Trà MyNo ratings yet
- Atlantic Coastwatch: An Era Ending?Document8 pagesAtlantic Coastwatch: An Era Ending?Friends of the Atlantic Coast Watch NewsletNo ratings yet
- HXM ECP L2 Partner Deep Dive Sales Presentation June 2021Document103 pagesHXM ECP L2 Partner Deep Dive Sales Presentation June 2021tegara2487No ratings yet
- Mary Mock Demurrer To 2nd Amended ComplaintDocument19 pagesMary Mock Demurrer To 2nd Amended ComplaintrongottschalkNo ratings yet
- Holy Spirit in Christianity - WikipediaDocument21 pagesHoly Spirit in Christianity - WikipediaSunny BautistaNo ratings yet