
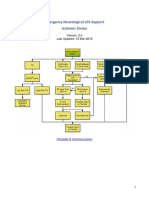
ENLS Acute Ischemic Stroke Protokol
ENLS Acute Ischemic Stroke Protokol
You might also like
- Vascular Access Principles and Practice by Samuel Eric WilsonDocument328 pagesVascular Access Principles and Practice by Samuel Eric WilsonBruno ZanuttiniNo ratings yet
- Challenging Concepts Book Series OUPDocument11 pagesChallenging Concepts Book Series OUPmakmgmNo ratings yet
- Activating A Stroke Alert - A Neurological Emergency - CE591Document7 pagesActivating A Stroke Alert - A Neurological Emergency - CE591Czar Julius Malasaga100% (1)
- Case StudyDocument6 pagesCase StudyMarie-Suzanne Tanyi100% (1)
- 2018 Article CIRSE2018 PDFDocument463 pages2018 Article CIRSE2018 PDFIulia LupascuNo ratings yet
- Emergency Neurological Life Support, Protocols.2019.4th EdDocument229 pagesEmergency Neurological Life Support, Protocols.2019.4th EdMohamad Mostafa100% (1)
- Enls V 3.0 Protocol Ais Final 0418Document25 pagesEnls V 3.0 Protocol Ais Final 0418Caleb LinNo ratings yet
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Day 4 - 10 PSBIM Review 2017 - Lecture - NeurologyDocument159 pagesDay 4 - 10 PSBIM Review 2017 - Lecture - NeurologyRye CalderonNo ratings yet
- Mechanical ThrombectomyDocument58 pagesMechanical Thrombectomyres.uditacharyaNo ratings yet
- Extra Acute Ischemic StrokeDocument52 pagesExtra Acute Ischemic Strokefyqmk4q8pkNo ratings yet
- Module #6 - Cerebral Vascular Accident: ObjectivesDocument7 pagesModule #6 - Cerebral Vascular Accident: ObjectivesWest AfricaNo ratings yet
- Enls v4 0 Ais Slides FinalDocument38 pagesEnls v4 0 Ais Slides FinalAndrio GultomNo ratings yet
- Neurologic EmergenciesDocument11 pagesNeurologic EmergenciesRoberto López MataNo ratings yet
- TPA Protocol: Stroke in Carefully Selected PersonsDocument4 pagesTPA Protocol: Stroke in Carefully Selected PersonsJavier Gonzalez, M.D. DABEMNo ratings yet
- Evidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?Document32 pagesEvidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?maluku barat dayaNo ratings yet
- Conversion GateDocument25 pagesConversion GateThomas HenrryNo ratings yet
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocument10 pagesGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidNo ratings yet
- ATLS Power Point PDFDocument54 pagesATLS Power Point PDFRizky LumalessilNo ratings yet
- DCV PDFDocument25 pagesDCV PDFLeyDi CamposanoNo ratings yet
- National Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Document15 pagesNational Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Muhammad FauziNo ratings yet
- Nursing NotesDocument7 pagesNursing NotesJayNo ratings yet
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- Acute Ischemic Stroke TD - StudentDocument8 pagesAcute Ischemic Stroke TD - Studentapi-594366475No ratings yet
- 2015 Update AHA-ASA Early Acute Stroke Guidelines PDFDocument28 pages2015 Update AHA-ASA Early Acute Stroke Guidelines PDFIvan Yoseph SaputraNo ratings yet
- ACLS Suspected Stroke AlgorithmDocument8 pagesACLS Suspected Stroke AlgorithmBirhane GebreegziabiherNo ratings yet
- AtlsDocument32 pagesAtlsMahesh RajwalNo ratings yet
- Stroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Document14 pagesStroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Natalia OrtizNo ratings yet
- ACLS Simulation ScenariosDocument14 pagesACLS Simulation ScenariosVanessa HermioneNo ratings yet
- Emergency Neurological Life Support Subarachnoid Hemorrhage: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Subarachnoid Hemorrhage: Last Updated: 19-Mar-2016michaelNo ratings yet
- Tiers IcpDocument12 pagesTiers IcpjheyfteeNo ratings yet
- Considerations For Post-Thrombolysis Monitoring in A Ward BedDocument4 pagesConsiderations For Post-Thrombolysis Monitoring in A Ward BedEllaNo ratings yet
- AclsDocument73 pagesAclsKamel Hady50% (2)
- HicksCodeStrokeHospitalists PDFDocument57 pagesHicksCodeStrokeHospitalists PDFRizky DimasaputraNo ratings yet
- Management of Acute Ischemic Stroke (AIS) DR GaneshDocument69 pagesManagement of Acute Ischemic Stroke (AIS) DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Ccu Handbook 2Document44 pagesCcu Handbook 2Nikunj GariaNo ratings yet
- Aha/Asa 2018 Guidelines For The Early Management of Patients With Acute Ischemic StrokeDocument4 pagesAha/Asa 2018 Guidelines For The Early Management of Patients With Acute Ischemic StrokeFrancisco PuenteNo ratings yet
- Pulmonary Edema, Hypotension, or Shock AlgorithmDocument34 pagesPulmonary Edema, Hypotension, or Shock AlgorithmMuhammad SafaatNo ratings yet
- Acute Stroke Management by Carlos L ChuaDocument61 pagesAcute Stroke Management by Carlos L ChuaRemaica Hernadez100% (1)
- Stroke:: What Should Nurses Need To Know About Stroke?Document68 pagesStroke:: What Should Nurses Need To Know About Stroke?Suci Aning TNo ratings yet
- Esc Acs GuidelinesDocument62 pagesEsc Acs GuidelineszakiyaNo ratings yet
- Stroke EssentialsDocument44 pagesStroke Essentialsapi-452244667No ratings yet
- Acute Management of StrokeDocument19 pagesAcute Management of StrokeBKGUBIONo ratings yet
- Acute Ischemic Stroke: Section Cerebrovascular DiseaseDocument4 pagesAcute Ischemic Stroke: Section Cerebrovascular DiseasenashihunamienNo ratings yet
- Ramilo, Sheena Patricia M. Ncenh06Document4 pagesRamilo, Sheena Patricia M. Ncenh06JaysellePuguonTabijeNo ratings yet
- Procedural SkillsDocument26 pagesProcedural Skillsmrcsexam.iranNo ratings yet
- Neuro Questionnaire 1Document1 pageNeuro Questionnaire 1Michael Baylon DueñasNo ratings yet
- Endovascular Therapy Neuro Intervention (MT) in AIS DR GaneshDocument34 pagesEndovascular Therapy Neuro Intervention (MT) in AIS DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Acute Stroke Lecture (Fall 2021) 2Document47 pagesAcute Stroke Lecture (Fall 2021) 2shahad alghamdiNo ratings yet
- The Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesDocument21 pagesThe Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesRubelyn Joy LazarteNo ratings yet
- Clinical Stroke Neurology (1) .1Document71 pagesClinical Stroke Neurology (1) .1Abhinav GuptaNo ratings yet
- Ghid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Document24 pagesGhid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Raluca L100% (1)
- Politrauma - Rolul AtiDocument18 pagesPolitrauma - Rolul AtiChirita ElenaNo ratings yet
- Acute Stroke Guideline January 2017Document9 pagesAcute Stroke Guideline January 2017Nanthini NarsanNo ratings yet
- Avinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006Document29 pagesAvinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006sgod34No ratings yet
- CVADocument4 pagesCVACloyd Marvin Pajas SegundoNo ratings yet
- Emergency Neurological Life Support Ischemic StrokeDocument22 pagesEmergency Neurological Life Support Ischemic Strokezero thirteen eighty oneNo ratings yet
- Complications of Percutaneous Coronary Intervention: The Survival HandbookFrom EverandComplications of Percutaneous Coronary Intervention: The Survival HandbookAlistair LindsayNo ratings yet
- Antiarrhythmic DrugsFrom EverandAntiarrhythmic DrugsAntoni Martínez-RubioNo ratings yet
- Diagnostic Services:-2D Echo, Audiometry, Bronchoscopy, CTDocument196 pagesDiagnostic Services:-2D Echo, Audiometry, Bronchoscopy, CTLalita NaiduNo ratings yet
- ابحاث انجليزيDocument11 pagesابحاث انجليزيصالح مقالحNo ratings yet
- Interpretation of Arterial Duplex Testing of LowerextremityDocument10 pagesInterpretation of Arterial Duplex Testing of LowerextremityLuciano AlvesNo ratings yet
- Guias JVS 2 Isquemia MMIIs Junio 2019Document163 pagesGuias JVS 2 Isquemia MMIIs Junio 2019LEOPOLDO MARTINEZNo ratings yet
- Chronic Limb Threatening IschemiaDocument35 pagesChronic Limb Threatening Ischemiasifatullah khanNo ratings yet
- Group 1,2,4 QuizDocument221 pagesGroup 1,2,4 QuizPaulNo ratings yet
- Artis ZeeDocument32 pagesArtis ZeeMarckus BrodyNo ratings yet
- RadiodiagnosisDocument42 pagesRadiodiagnosisMasroof GanieNo ratings yet
- Lesson Plan ON AneurysmDocument8 pagesLesson Plan ON AneurysmAnusikta PandaNo ratings yet
- Interventional Infection PreventionDocument43 pagesInterventional Infection PreventionDewi Ratna SariNo ratings yet
- 9th Mena Stroke Agenda FDocument8 pages9th Mena Stroke Agenda FMaya MathewNo ratings yet
- Chronic Aortic DissectionDocument22 pagesChronic Aortic DissectionElena CamposNo ratings yet
- Aneurysm: From Wikipedia, The Free EncyclopediaDocument8 pagesAneurysm: From Wikipedia, The Free EncyclopediajazmiaNo ratings yet
- Angiography PreparationsDocument14 pagesAngiography PreparationsAndrei BulgariuNo ratings yet
- Aortic Coarctation Cardiology Clinics 2020Document15 pagesAortic Coarctation Cardiology Clinics 2020Angela OrozcoNo ratings yet
- My CV in PDF File LDocument115 pagesMy CV in PDF File LMohamed Omar ElfarokNo ratings yet
- Paket BHP Cath-Lab Pt. Giri Sakti UtamaDocument2 pagesPaket BHP Cath-Lab Pt. Giri Sakti UtamaDyazAufarNo ratings yet
- Agenda Dialysis Access and Interventions v3 FinalDocument4 pagesAgenda Dialysis Access and Interventions v3 Finalfouad tabetNo ratings yet
- Ebook Dont Downloadcontains TXT Software Rutherfords Vascular Surgery and Endovascular Therapy PDF Full Chapter PDFDocument67 pagesEbook Dont Downloadcontains TXT Software Rutherfords Vascular Surgery and Endovascular Therapy PDF Full Chapter PDFkathleen.ratcliff442100% (49)
- Imaging Predictors of Procedural and Clinical OutcDocument13 pagesImaging Predictors of Procedural and Clinical OutcYusuf BrilliantNo ratings yet
- Overview of Lower Extremity Peripheral Artery DiseaseDocument24 pagesOverview of Lower Extremity Peripheral Artery DiseasePetru GlavanNo ratings yet
- Complications in Endovascular Surgery Peri Procedural Prevention and Treatment Feb 2 2021 - 0323554482 - Elsevier 1st Edition Dryjski MD PHD FacsDocument54 pagesComplications in Endovascular Surgery Peri Procedural Prevention and Treatment Feb 2 2021 - 0323554482 - Elsevier 1st Edition Dryjski MD PHD Facssteven.owens745100% (14)
- Iec 60601-2-43-2010Document112 pagesIec 60601-2-43-2010latifNo ratings yet
- Guide Catheters Guidewire Overview and Case Illustra5onsDocument45 pagesGuide Catheters Guidewire Overview and Case Illustra5onsNeet Aipg newstips100% (1)
- English FinalsDocument28 pagesEnglish FinalsMark M. Alipio100% (1)
- Recent Innovations in Renal Vascular ImagingDocument16 pagesRecent Innovations in Renal Vascular ImagingHector Hernandez-SoriaNo ratings yet
- Dr. Tondi Maspian Tjili, SPBS (K), M.Kes (Advanced Techniques For Minimallu Invasive in Hemorhagic Stroke)Document22 pagesDr. Tondi Maspian Tjili, SPBS (K), M.Kes (Advanced Techniques For Minimallu Invasive in Hemorhagic Stroke)dewiswahyuNo ratings yet
























































































Download as pdf or txt
You might also like
- Vascular Access Principles and Practice by Samuel Eric WilsonDocument328 pagesVascular Access Principles and Practice by Samuel Eric WilsonBruno ZanuttiniNo ratings yet
- Challenging Concepts Book Series OUPDocument11 pagesChallenging Concepts Book Series OUPmakmgmNo ratings yet
- Activating A Stroke Alert - A Neurological Emergency - CE591Document7 pagesActivating A Stroke Alert - A Neurological Emergency - CE591Czar Julius Malasaga100% (1)
- Case StudyDocument6 pagesCase StudyMarie-Suzanne Tanyi100% (1)
- 2018 Article CIRSE2018 PDFDocument463 pages2018 Article CIRSE2018 PDFIulia LupascuNo ratings yet
- Emergency Neurological Life Support, Protocols.2019.4th EdDocument229 pagesEmergency Neurological Life Support, Protocols.2019.4th EdMohamad Mostafa100% (1)
- Enls V 3.0 Protocol Ais Final 0418Document25 pagesEnls V 3.0 Protocol Ais Final 0418Caleb LinNo ratings yet
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Day 4 - 10 PSBIM Review 2017 - Lecture - NeurologyDocument159 pagesDay 4 - 10 PSBIM Review 2017 - Lecture - NeurologyRye CalderonNo ratings yet
- Mechanical ThrombectomyDocument58 pagesMechanical Thrombectomyres.uditacharyaNo ratings yet
- Extra Acute Ischemic StrokeDocument52 pagesExtra Acute Ischemic Strokefyqmk4q8pkNo ratings yet
- Module #6 - Cerebral Vascular Accident: ObjectivesDocument7 pagesModule #6 - Cerebral Vascular Accident: ObjectivesWest AfricaNo ratings yet
- Enls v4 0 Ais Slides FinalDocument38 pagesEnls v4 0 Ais Slides FinalAndrio GultomNo ratings yet
- Neurologic EmergenciesDocument11 pagesNeurologic EmergenciesRoberto López MataNo ratings yet
- TPA Protocol: Stroke in Carefully Selected PersonsDocument4 pagesTPA Protocol: Stroke in Carefully Selected PersonsJavier Gonzalez, M.D. DABEMNo ratings yet
- Evidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?Document32 pagesEvidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?maluku barat dayaNo ratings yet
- Conversion GateDocument25 pagesConversion GateThomas HenrryNo ratings yet
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocument10 pagesGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidNo ratings yet
- ATLS Power Point PDFDocument54 pagesATLS Power Point PDFRizky LumalessilNo ratings yet
- DCV PDFDocument25 pagesDCV PDFLeyDi CamposanoNo ratings yet
- National Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Document15 pagesNational Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Muhammad FauziNo ratings yet
- Nursing NotesDocument7 pagesNursing NotesJayNo ratings yet
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- Acute Ischemic Stroke TD - StudentDocument8 pagesAcute Ischemic Stroke TD - Studentapi-594366475No ratings yet
- 2015 Update AHA-ASA Early Acute Stroke Guidelines PDFDocument28 pages2015 Update AHA-ASA Early Acute Stroke Guidelines PDFIvan Yoseph SaputraNo ratings yet
- ACLS Suspected Stroke AlgorithmDocument8 pagesACLS Suspected Stroke AlgorithmBirhane GebreegziabiherNo ratings yet
- AtlsDocument32 pagesAtlsMahesh RajwalNo ratings yet
- Stroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Document14 pagesStroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Natalia OrtizNo ratings yet
- ACLS Simulation ScenariosDocument14 pagesACLS Simulation ScenariosVanessa HermioneNo ratings yet
- Emergency Neurological Life Support Subarachnoid Hemorrhage: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Subarachnoid Hemorrhage: Last Updated: 19-Mar-2016michaelNo ratings yet
- Tiers IcpDocument12 pagesTiers IcpjheyfteeNo ratings yet
- Considerations For Post-Thrombolysis Monitoring in A Ward BedDocument4 pagesConsiderations For Post-Thrombolysis Monitoring in A Ward BedEllaNo ratings yet
- AclsDocument73 pagesAclsKamel Hady50% (2)
- HicksCodeStrokeHospitalists PDFDocument57 pagesHicksCodeStrokeHospitalists PDFRizky DimasaputraNo ratings yet
- Management of Acute Ischemic Stroke (AIS) DR GaneshDocument69 pagesManagement of Acute Ischemic Stroke (AIS) DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Ccu Handbook 2Document44 pagesCcu Handbook 2Nikunj GariaNo ratings yet
- Aha/Asa 2018 Guidelines For The Early Management of Patients With Acute Ischemic StrokeDocument4 pagesAha/Asa 2018 Guidelines For The Early Management of Patients With Acute Ischemic StrokeFrancisco PuenteNo ratings yet
- Pulmonary Edema, Hypotension, or Shock AlgorithmDocument34 pagesPulmonary Edema, Hypotension, or Shock AlgorithmMuhammad SafaatNo ratings yet
- Acute Stroke Management by Carlos L ChuaDocument61 pagesAcute Stroke Management by Carlos L ChuaRemaica Hernadez100% (1)
- Stroke:: What Should Nurses Need To Know About Stroke?Document68 pagesStroke:: What Should Nurses Need To Know About Stroke?Suci Aning TNo ratings yet
- Esc Acs GuidelinesDocument62 pagesEsc Acs GuidelineszakiyaNo ratings yet
- Stroke EssentialsDocument44 pagesStroke Essentialsapi-452244667No ratings yet
- Acute Management of StrokeDocument19 pagesAcute Management of StrokeBKGUBIONo ratings yet
- Acute Ischemic Stroke: Section Cerebrovascular DiseaseDocument4 pagesAcute Ischemic Stroke: Section Cerebrovascular DiseasenashihunamienNo ratings yet
- Ramilo, Sheena Patricia M. Ncenh06Document4 pagesRamilo, Sheena Patricia M. Ncenh06JaysellePuguonTabijeNo ratings yet
- Procedural SkillsDocument26 pagesProcedural Skillsmrcsexam.iranNo ratings yet
- Neuro Questionnaire 1Document1 pageNeuro Questionnaire 1Michael Baylon DueñasNo ratings yet
- Endovascular Therapy Neuro Intervention (MT) in AIS DR GaneshDocument34 pagesEndovascular Therapy Neuro Intervention (MT) in AIS DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Acute Stroke Lecture (Fall 2021) 2Document47 pagesAcute Stroke Lecture (Fall 2021) 2shahad alghamdiNo ratings yet
- The Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesDocument21 pagesThe Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesRubelyn Joy LazarteNo ratings yet
- Clinical Stroke Neurology (1) .1Document71 pagesClinical Stroke Neurology (1) .1Abhinav GuptaNo ratings yet
- Ghid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Document24 pagesGhid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Raluca L100% (1)
- Politrauma - Rolul AtiDocument18 pagesPolitrauma - Rolul AtiChirita ElenaNo ratings yet
- Acute Stroke Guideline January 2017Document9 pagesAcute Stroke Guideline January 2017Nanthini NarsanNo ratings yet
- Avinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006Document29 pagesAvinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006sgod34No ratings yet
- CVADocument4 pagesCVACloyd Marvin Pajas SegundoNo ratings yet
- Emergency Neurological Life Support Ischemic StrokeDocument22 pagesEmergency Neurological Life Support Ischemic Strokezero thirteen eighty oneNo ratings yet
- Complications of Percutaneous Coronary Intervention: The Survival HandbookFrom EverandComplications of Percutaneous Coronary Intervention: The Survival HandbookAlistair LindsayNo ratings yet
- Antiarrhythmic DrugsFrom EverandAntiarrhythmic DrugsAntoni Martínez-RubioNo ratings yet
- Diagnostic Services:-2D Echo, Audiometry, Bronchoscopy, CTDocument196 pagesDiagnostic Services:-2D Echo, Audiometry, Bronchoscopy, CTLalita NaiduNo ratings yet
- ابحاث انجليزيDocument11 pagesابحاث انجليزيصالح مقالحNo ratings yet
- Interpretation of Arterial Duplex Testing of LowerextremityDocument10 pagesInterpretation of Arterial Duplex Testing of LowerextremityLuciano AlvesNo ratings yet
- Guias JVS 2 Isquemia MMIIs Junio 2019Document163 pagesGuias JVS 2 Isquemia MMIIs Junio 2019LEOPOLDO MARTINEZNo ratings yet
- Chronic Limb Threatening IschemiaDocument35 pagesChronic Limb Threatening Ischemiasifatullah khanNo ratings yet
- Group 1,2,4 QuizDocument221 pagesGroup 1,2,4 QuizPaulNo ratings yet
- Artis ZeeDocument32 pagesArtis ZeeMarckus BrodyNo ratings yet
- RadiodiagnosisDocument42 pagesRadiodiagnosisMasroof GanieNo ratings yet
- Lesson Plan ON AneurysmDocument8 pagesLesson Plan ON AneurysmAnusikta PandaNo ratings yet
- Interventional Infection PreventionDocument43 pagesInterventional Infection PreventionDewi Ratna SariNo ratings yet
- 9th Mena Stroke Agenda FDocument8 pages9th Mena Stroke Agenda FMaya MathewNo ratings yet
- Chronic Aortic DissectionDocument22 pagesChronic Aortic DissectionElena CamposNo ratings yet
- Aneurysm: From Wikipedia, The Free EncyclopediaDocument8 pagesAneurysm: From Wikipedia, The Free EncyclopediajazmiaNo ratings yet
- Angiography PreparationsDocument14 pagesAngiography PreparationsAndrei BulgariuNo ratings yet
- Aortic Coarctation Cardiology Clinics 2020Document15 pagesAortic Coarctation Cardiology Clinics 2020Angela OrozcoNo ratings yet
- My CV in PDF File LDocument115 pagesMy CV in PDF File LMohamed Omar ElfarokNo ratings yet
- Paket BHP Cath-Lab Pt. Giri Sakti UtamaDocument2 pagesPaket BHP Cath-Lab Pt. Giri Sakti UtamaDyazAufarNo ratings yet
- Agenda Dialysis Access and Interventions v3 FinalDocument4 pagesAgenda Dialysis Access and Interventions v3 Finalfouad tabetNo ratings yet
- Ebook Dont Downloadcontains TXT Software Rutherfords Vascular Surgery and Endovascular Therapy PDF Full Chapter PDFDocument67 pagesEbook Dont Downloadcontains TXT Software Rutherfords Vascular Surgery and Endovascular Therapy PDF Full Chapter PDFkathleen.ratcliff442100% (49)
- Imaging Predictors of Procedural and Clinical OutcDocument13 pagesImaging Predictors of Procedural and Clinical OutcYusuf BrilliantNo ratings yet
- Overview of Lower Extremity Peripheral Artery DiseaseDocument24 pagesOverview of Lower Extremity Peripheral Artery DiseasePetru GlavanNo ratings yet
- Complications in Endovascular Surgery Peri Procedural Prevention and Treatment Feb 2 2021 - 0323554482 - Elsevier 1st Edition Dryjski MD PHD FacsDocument54 pagesComplications in Endovascular Surgery Peri Procedural Prevention and Treatment Feb 2 2021 - 0323554482 - Elsevier 1st Edition Dryjski MD PHD Facssteven.owens745100% (14)
- Iec 60601-2-43-2010Document112 pagesIec 60601-2-43-2010latifNo ratings yet
- Guide Catheters Guidewire Overview and Case Illustra5onsDocument45 pagesGuide Catheters Guidewire Overview and Case Illustra5onsNeet Aipg newstips100% (1)
- English FinalsDocument28 pagesEnglish FinalsMark M. Alipio100% (1)
- Recent Innovations in Renal Vascular ImagingDocument16 pagesRecent Innovations in Renal Vascular ImagingHector Hernandez-SoriaNo ratings yet
- Dr. Tondi Maspian Tjili, SPBS (K), M.Kes (Advanced Techniques For Minimallu Invasive in Hemorhagic Stroke)Document22 pagesDr. Tondi Maspian Tjili, SPBS (K), M.Kes (Advanced Techniques For Minimallu Invasive in Hemorhagic Stroke)dewiswahyuNo ratings yet