Download as pdf or txt
You might also like
- Bleeding Disorders FinalDocument35 pagesBleeding Disorders FinalsanthiyasandyNo ratings yet
- Recombiplastin 2G - 0020002950 (8 ML) : Al For Identification and Resolution of Out-Of-Control SituationsDocument5 pagesRecombiplastin 2G - 0020002950 (8 ML) : Al For Identification and Resolution of Out-Of-Control SituationsSteffyPérezPioNo ratings yet
- Bleeding DisordersDocument137 pagesBleeding DisordersJosiah BimabamNo ratings yet
- Bleeding Disorder (Paediatrics)Document95 pagesBleeding Disorder (Paediatrics)Nurul Afiqah Mohd YusoffNo ratings yet
- 7.hematology Oncology RDocument48 pages7.hematology Oncology Ranas barakahNo ratings yet
- ThrombocytopeniaDocument4 pagesThrombocytopeniaValerrie NgenoNo ratings yet
- ThrombophiliaDocument17 pagesThrombophiliaAbikunda FabriceNo ratings yet
- Inherited Disorders of Platelet Function,ITP and TTPDocument22 pagesInherited Disorders of Platelet Function,ITP and TTPYazanNo ratings yet
- Quantitative Platelet DisorderDocument75 pagesQuantitative Platelet Disorderirishgopez24No ratings yet
- 7 Bleeding Disorders DR - AlaaDocument35 pages7 Bleeding Disorders DR - Alaaaj1998ajNo ratings yet
- Lecture 16 - Bleeding Tendency DiseasesDocument64 pagesLecture 16 - Bleeding Tendency Diseasesapi-3703352100% (1)
- Platelet: Muhammad Nazarudin, S.STDocument15 pagesPlatelet: Muhammad Nazarudin, S.STFafha FafhaNo ratings yet
- Diseases of PlateletsDocument86 pagesDiseases of Plateletsdesktop dolakhaNo ratings yet
- PATH - Bleeding Disorders (7p)Document7 pagesPATH - Bleeding Disorders (7p)Omar HamwiNo ratings yet
- Platelet Disorders:: Marshell Tendean, MD Department of Internal Medicine UKRIDA Jakarta 2016Document27 pagesPlatelet Disorders:: Marshell Tendean, MD Department of Internal Medicine UKRIDA Jakarta 2016charlesy TNo ratings yet
- Define: Gaucher's Disease: AnemiaDocument7 pagesDefine: Gaucher's Disease: AnemiacyrelleNo ratings yet
- Bleeding DisordersDocument35 pagesBleeding DisordersSarahNo ratings yet
- Platelets DisordersDocument29 pagesPlatelets DisordersReza Muhamad NugrahaNo ratings yet
- HemII-chapter 24Document48 pagesHemII-chapter 24m76gmmNo ratings yet
- PlateletDocument15 pagesPlateletFafha FafhaNo ratings yet
- Disturbances of CirculationDocument10 pagesDisturbances of CirculationSuhan HasanNo ratings yet
- Thrombocytopenia Thrombotic Thrombocytopenic Purpura: DR Ahmad Abu Al-Samen MDDocument17 pagesThrombocytopenia Thrombotic Thrombocytopenic Purpura: DR Ahmad Abu Al-Samen MDmohNo ratings yet
- Lecture 5 White Cell DisordersDocument17 pagesLecture 5 White Cell DisordersOsama MalikNo ratings yet
- Disorders of Platelet Prepared By: Abdelgadir H. ElagibDocument5 pagesDisorders of Platelet Prepared By: Abdelgadir H. ElagibthabitbinNo ratings yet
- Hemostasis Coaching NotesDocument45 pagesHemostasis Coaching NotesBen SabladaNo ratings yet
- Bleeding Disorders NPMCDocument58 pagesBleeding Disorders NPMCAbosedeNo ratings yet
- Disorders of PlateletsfDocument51 pagesDisorders of PlateletsfSyarifah Tridani FitriaNo ratings yet
- Coagulation Disorders:: Primary HemostasisDocument58 pagesCoagulation Disorders:: Primary HemostasisFerji Rhenald Arditya100% (1)
- Hemostasis - Hematology BlockDocument40 pagesHemostasis - Hematology BlockamandaNo ratings yet
- QPD Reporting Hema 2Document27 pagesQPD Reporting Hema 2Edmarie GuzmanNo ratings yet
- Bleeding DisorderDocument90 pagesBleeding DisorderAnooda MazenNo ratings yet
- Thrombosis and Antithrombotic TherapyDocument3 pagesThrombosis and Antithrombotic TherapyAdham TarekNo ratings yet
- Trombositopenia Dan TrombositosisDocument33 pagesTrombositopenia Dan TrombositosisAim AimmaNo ratings yet
- ThrombocytopeniaDocument49 pagesThrombocytopeniaMaria EnjelinaNo ratings yet
- Diseases Involving Blood Vessels of The KidneysDocument34 pagesDiseases Involving Blood Vessels of The KidneysAma SatharasingheNo ratings yet
- Secondary HemostasisDocument9 pagesSecondary HemostasisMedicah Simon PeligrinoNo ratings yet
- MTY1215 Hematology 2 (Lec) HandoutsDocument7 pagesMTY1215 Hematology 2 (Lec) HandoutsDarren Gabriel NicolasNo ratings yet
- Natural Remedies To Increase Platelet Count: Swati BurungaleDocument5 pagesNatural Remedies To Increase Platelet Count: Swati BurungaleraamNo ratings yet
- Disorder of PlateletsDocument27 pagesDisorder of PlateletsRoby KieranNo ratings yet
- Hematology 2 Lecture Notes Platelet Quantitative DisordersDocument10 pagesHematology 2 Lecture Notes Platelet Quantitative DisorderscccomayogNo ratings yet
- Bleeding and Coagulation Disorders: DR Nidhi Chaurasia JR-1 MDS PedodonticsDocument66 pagesBleeding and Coagulation Disorders: DR Nidhi Chaurasia JR-1 MDS PedodonticsDrNidhi KrishnaNo ratings yet
- Thrombosis Embolism InfarctionDocument64 pagesThrombosis Embolism InfarctionDontoNo ratings yet
- DVT DR Moses KazeevuDocument24 pagesDVT DR Moses KazeevuMoses Jr KazevuNo ratings yet
- CoagulopathyDocument121 pagesCoagulopathyMegat Mohd Azman AdzmiNo ratings yet
- Hemostasis Disorders in LeukemiaDocument14 pagesHemostasis Disorders in LeukemiaNurul HidayahNo ratings yet
- Hematology 2 SummaryDocument8 pagesHematology 2 Summarymonzon.mika1801No ratings yet
- Bleeding DisordersDocument35 pagesBleeding Disorderskholoud220100% (3)
- ThrombocytopeniaDocument9 pagesThrombocytopenia8pvz96ktd9No ratings yet
- Bleeding Disorders - DR RashaDocument95 pagesBleeding Disorders - DR RashaRasha TelebNo ratings yet
- 5 Hemodynamic Disorders, Thromboembolism and ShockDocument162 pages5 Hemodynamic Disorders, Thromboembolism and Shocksinte beyuNo ratings yet
- Thrombosis AND Disorders OF HemostasisDocument73 pagesThrombosis AND Disorders OF HemostasisAdel mohammadNo ratings yet
- Lecture 4 Bleeding DisorderDocument10 pagesLecture 4 Bleeding Disordernatheer ayedNo ratings yet
- Inherited Platelet AbnormalitiesDocument1 pageInherited Platelet AbnormalitiesNeoMedicaNo ratings yet
- Secondary Clotting DisordersDocument34 pagesSecondary Clotting DisordersLyra Dennise LlidoNo ratings yet
- Pathology Bleeding DisordersDocument67 pagesPathology Bleeding DisordersMarcelliaNo ratings yet
- Gangguan TrombositDocument47 pagesGangguan TrombositLayli Nur ArniatiNo ratings yet
- Lecture 3. Bleeding Disorders Part 1Document31 pagesLecture 3. Bleeding Disorders Part 1Kekelwa Mutumwenu Snr100% (1)
- Platelet DisordersDocument6 pagesPlatelet DisordersMehr AliNo ratings yet
- Bleeding DisordersDocument56 pagesBleeding DisordersDina GamalNo ratings yet
- A Simple Guide to Thrombocytopenia (Abnormally Low Platelets), Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Thrombocytopenia (Abnormally Low Platelets), Diagnosis, Treatment and Related ConditionsNo ratings yet
- 5 PathogensisDocument34 pages5 Pathogensisمصطفي خندقاويNo ratings yet
- 04 Lec - Giardiasis & TrichmoniasisDocument25 pages04 Lec - Giardiasis & Trichmoniasisمصطفي خندقاويNo ratings yet
- 2 & 3 Protozoa and MalariaDocument22 pages2 & 3 Protozoa and Malariaمصطفي خندقاويNo ratings yet
- CestodesDocument34 pagesCestodesمصطفي خندقاويNo ratings yet
- AscarisDocument42 pagesAscarisمصطفي خندقاوي100% (1)
- The LeukemiasDocument52 pagesThe Leukemiasمصطفي خندقاوي100% (1)
- 1 - IntrdxnDocument18 pages1 - Intrdxnمصطفي خندقاويNo ratings yet
- Ic Doc Form Routes 2and4 2Document1 pageIc Doc Form Routes 2and4 2مصطفي خندقاويNo ratings yet
- Dr. Agtuca - PBS, Differential Count, and Reticulocyte CountDocument58 pagesDr. Agtuca - PBS, Differential Count, and Reticulocyte Countمصطفي خندقاويNo ratings yet
- 1-CBC InterpretationDocument10 pages1-CBC Interpretationمصطفي خندقاويNo ratings yet
- Medical Laboratory Sciences Past, Present and FutureDocument5 pagesMedical Laboratory Sciences Past, Present and Futureمصطفي خندقاويNo ratings yet
- Normal HemostasisDocument34 pagesNormal Hemostasisمصطفي خندقاويNo ratings yet
- B L A S T: Asic Ocal Lignment Earch OolDocument22 pagesB L A S T: Asic Ocal Lignment Earch Oolمصطفي خندقاويNo ratings yet
- السعادةDocument21 pagesالسعادةمصطفي خندقاويNo ratings yet
- Lesson-Plan-TemplateDocument2 pagesLesson-Plan-Templateمصطفي خندقاويNo ratings yet
- CURS 12 - Coagularea Intravasculara Diseminata (DR - Manuela Crisan-16.10)Document71 pagesCURS 12 - Coagularea Intravasculara Diseminata (DR - Manuela Crisan-16.10)veronicaNo ratings yet
- Platelet Disorders: N.VigneshDocument48 pagesPlatelet Disorders: N.VigneshVignesh NarayananNo ratings yet
- Coagulation Cascade: Difference Between Intrinsic and Extrinsic PathwayDocument10 pagesCoagulation Cascade: Difference Between Intrinsic and Extrinsic Pathwayroshmae100% (1)
- Hemophilia and Factor Assay PDFDocument17 pagesHemophilia and Factor Assay PDFSumaira JunaidNo ratings yet
- CoagulationDocument3 pagesCoagulationHerho-nyl CesNo ratings yet
- Original Article: Costs and Utilization of Hemophilia A and B Patients With and Without InhibitorsDocument5 pagesOriginal Article: Costs and Utilization of Hemophilia A and B Patients With and Without InhibitorsMelisa ClaireNo ratings yet
- Acquired Coagulation AbnormalitiesDocument6 pagesAcquired Coagulation AbnormalitiesDrMohammad MoyassarNo ratings yet
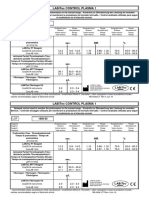
- LABiTec Control 1 Insert 1956 35 Revision 2.0Document1 pageLABiTec Control 1 Insert 1956 35 Revision 2.0Carla YcoNo ratings yet
- Warfarin Mechanism of Action, Indications AtfDocument4 pagesWarfarin Mechanism of Action, Indications AtfAmir mohammad moori MohammadiNo ratings yet
- Hemostasis and Coagulation: Miklós MolnárDocument67 pagesHemostasis and Coagulation: Miklós MolnárHamzaNo ratings yet
- Anki Hema Lab TestDocument3 pagesAnki Hema Lab TestMarietoni PicoNo ratings yet
- A Brief History of HemophiliaDocument127 pagesA Brief History of HemophiliaApurba SahaNo ratings yet
- Multifibren UDocument6 pagesMultifibren UMari Fere100% (1)
- Vas 004Document16 pagesVas 004Stephen CandinegaraNo ratings yet
- Platelet DisordersDocument12 pagesPlatelet Disorderstutor tujuhNo ratings yet
- Learning ObjectivesDocument12 pagesLearning ObjectivesjmcvicenteNo ratings yet
- Hemophilia B - StatPearls - NCBI BookshelfDocument8 pagesHemophilia B - StatPearls - NCBI BookshelflolNo ratings yet
- Data Anggit HirudinDocument5 pagesData Anggit Hirudinharyo anggitNo ratings yet
- Basic Principles of HemostasisDocument5 pagesBasic Principles of HemostasisSean Matthew100% (1)
- 6 Bleeding DisordersDocument19 pages6 Bleeding DisordersSumit GuptaNo ratings yet
- Disseminated Intravascular Coagulation in Infants and ChildrenDocument40 pagesDisseminated Intravascular Coagulation in Infants and Childrenkabulkabulovich5No ratings yet
- HEMOPHILIA Co Chat Uc Che - Ts Tuan 2024Document38 pagesHEMOPHILIA Co Chat Uc Che - Ts Tuan 2024Toàn PhùngNo ratings yet
- Labmed33 0948Document6 pagesLabmed33 0948VKTNNo ratings yet
- Introduction To HaemostasisDocument18 pagesIntroduction To Haemostasiswatchme3No ratings yet
- Hema OmgDocument82 pagesHema OmgBernadeth BaduaNo ratings yet
- Intraop - Hemorrage and Bleeding DiathesisDocument1 pageIntraop - Hemorrage and Bleeding DiathesisKezia ImanuellaNo ratings yet
- Edema: USMLE Step 1 Web Prep - Circulatory PathologyDocument9 pagesEdema: USMLE Step 1 Web Prep - Circulatory PathologyfrabziNo ratings yet
- Blood Clots: How Does Blood Clot?Document2 pagesBlood Clots: How Does Blood Clot?Pebrian Diki PrestyaNo ratings yet
- Management of Bleeding PDFDocument25 pagesManagement of Bleeding PDFGlory Owens AgbonkpoloNo ratings yet