Download as pdf or txt
You might also like
- Atlanta Heat Island StudyDocument20 pagesAtlanta Heat Island StudyJonathan RaymondNo ratings yet
- AACR 2022 Proceedings: Part A Online-Only and April 10From EverandAACR 2022 Proceedings: Part A Online-Only and April 10No ratings yet
- Towards 2020 ScienceDocument86 pagesTowards 2020 Sciencespn100% (4)
- Kolagocarsinoma PDFDocument7 pagesKolagocarsinoma PDFBerlyan RuslanNo ratings yet
- Biology of Blood and Marrow Transplantation: Journal HomepageDocument7 pagesBiology of Blood and Marrow Transplantation: Journal HomepageYakobus Antonius SobuberNo ratings yet
- 236 297Document8 pages236 297Andrea KamóNo ratings yet
- Basophil-Biomarker-Fibrosis - PMF 2018Document8 pagesBasophil-Biomarker-Fibrosis - PMF 2018Banchob SripaNo ratings yet
- Clinical Burden of Preoperative Albumin Globulin Rat - 2017 - The American JournDocument8 pagesClinical Burden of Preoperative Albumin Globulin Rat - 2017 - The American JournFlorin AchimNo ratings yet
- Qi 2022Document12 pagesQi 2022Jonathan Billy ChristianNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- Marcadores Sericos para Cole AgudaDocument6 pagesMarcadores Sericos para Cole Agudajessica MárquezNo ratings yet
- Prognostic Significance of Lymphocyte Monocyte Ratio in Patients With Ovarian CancerDocument7 pagesPrognostic Significance of Lymphocyte Monocyte Ratio in Patients With Ovarian CancerRizka AdiNo ratings yet
- Extended Leukocyte Differential Count and C-Reactive Protein inDocument8 pagesExtended Leukocyte Differential Count and C-Reactive Protein ini chen chenNo ratings yet
- Choque Septico y Falla Multiorgano Relaciona Con Balance de FluidosDocument14 pagesChoque Septico y Falla Multiorgano Relaciona Con Balance de FluidosMiguel Angel Hernandez SerratoNo ratings yet
- Prognostic Significance of Neutrophil-to-Lymphocyte Ratio and PLRDocument9 pagesPrognostic Significance of Neutrophil-to-Lymphocyte Ratio and PLRdominguezmariela465No ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- (10920684 - Neurosurgical Focus) Impact of Preoperative Endovascular Embolization On Immediate Meningioma Resection OutcomesDocument7 pages(10920684 - Neurosurgical Focus) Impact of Preoperative Endovascular Embolization On Immediate Meningioma Resection OutcomesBedussa NuritNo ratings yet
- 2017 Article 3322Document7 pages2017 Article 3322Kevin MandakNo ratings yet
- Serum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient SurvivalDocument9 pagesSerum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient Survivalmelda lestari haidirNo ratings yet
- First-Line Treatment of Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-AnalysisDocument8 pagesFirst-Line Treatment of Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-AnalysisDr. Alexandre SatoNo ratings yet
- Preoperative Platelet-Lymphocyte Ratio Is A Superior Prognostic FactorDocument7 pagesPreoperative Platelet-Lymphocyte Ratio Is A Superior Prognostic Factordominguezmariela465No ratings yet
- Development and Validation of A Prognostic Model For Predicting Overall Survival in Patients With Bladder Cancer: A SEER-Based StudyDocument10 pagesDevelopment and Validation of A Prognostic Model For Predicting Overall Survival in Patients With Bladder Cancer: A SEER-Based Studymahmud.meftahNo ratings yet
- Molecular RCC EmtDocument8 pagesMolecular RCC EmtnadalNo ratings yet
- Journal of Critical Care: Clinical PotpourriDocument7 pagesJournal of Critical Care: Clinical PotpourriUnomoshNo ratings yet
- Prognostic Significance of Hematologic Markers in Patients With Head and Neck Squamous Cell CarcinomasDocument11 pagesPrognostic Significance of Hematologic Markers in Patients With Head and Neck Squamous Cell CarcinomasLeyla M HattaNo ratings yet
- Yu SIFDocument8 pagesYu SIFAhmed AyazNo ratings yet
- Utility of Cytometric Parameters and Indices As Predictors of Mortality in Patients With SepsisDocument6 pagesUtility of Cytometric Parameters and Indices As Predictors of Mortality in Patients With SepsisPablo VélezNo ratings yet
- Document 1Document8 pagesDocument 1JOSE PORTILLONo ratings yet
- Acute Renal Failure in Critically Ill Surgical Patients PDFDocument7 pagesAcute Renal Failure in Critically Ill Surgical Patients PDFRomán Jiménez LópezNo ratings yet
- Pancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoDocument6 pagesPancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoYeni PuspitasariNo ratings yet
- Outcome of Allogeneic Hematopoietic Stem Cell Transplantati - 2019 - Biology ofDocument9 pagesOutcome of Allogeneic Hematopoietic Stem Cell Transplantati - 2019 - Biology ofFrankenstein MelancholyNo ratings yet
- The Role of The Platelet-To-Lymphocyte Ratio and NDocument5 pagesThe Role of The Platelet-To-Lymphocyte Ratio and NRudy Arindra WijayaNo ratings yet
- Anemia Aplastic JournalDocument13 pagesAnemia Aplastic JournalGenoveva Maditias Dwi PertiwiNo ratings yet
- Ap 1Document4 pagesAp 1Claujandra PalaciosNo ratings yet
- Sadat 2013Document17 pagesSadat 2013fotea_nicoleta816No ratings yet
- JCTH 2016 00035Document8 pagesJCTH 2016 00035Rengganis PutriNo ratings yet
- 1078 0432.CCR 14 0442.fullDocument12 pages1078 0432.CCR 14 0442.fullAndrea KamóNo ratings yet
- Neutrophil To Lymphocyte and Platelet To LymphocytDocument7 pagesNeutrophil To Lymphocyte and Platelet To LymphocytpriyaNo ratings yet
- Delta Neutrophil Index and Neutrophil-to-Lymphocyte Ratio in The Differentiation of Thyroid Malignancy and Nodular GoiterDocument8 pagesDelta Neutrophil Index and Neutrophil-to-Lymphocyte Ratio in The Differentiation of Thyroid Malignancy and Nodular GoiteragusNo ratings yet
- PCRmarcador COLECISTITIS2019Document7 pagesPCRmarcador COLECISTITIS2019Daniela VahlisNo ratings yet
- The Predictive Value of Four Serum Biomarkers ForDocument8 pagesThe Predictive Value of Four Serum Biomarkers Forsebasags19No ratings yet
- Monografia MeningitisDocument4 pagesMonografia MeningitisJulian GomezNo ratings yet
- Fukunaga 2021Document7 pagesFukunaga 2021stenberg.gamesNo ratings yet
- Lotan Et Al. Molecular Marker For Rec and Cancer Specific Survival Post Radical CystectomyDocument7 pagesLotan Et Al. Molecular Marker For Rec and Cancer Specific Survival Post Radical CystectomyyuenkeithNo ratings yet
- Jkms 29 519Document8 pagesJkms 29 519Ana KhurniaNo ratings yet
- Overexpression of Mesothelin in Pancreatic Ductal Adenocarcinoma (PDAC)Document6 pagesOverexpression of Mesothelin in Pancreatic Ductal Adenocarcinoma (PDAC)Belia Bima NafisaNo ratings yet
- Cutoff 4-5Document7 pagesCutoff 4-5Ian HuangNo ratings yet
- Principales Emergencias Oncológicas en El Cáncer de Pulmón: Un Análisis de Un Único CentroDocument3 pagesPrincipales Emergencias Oncológicas en El Cáncer de Pulmón: Un Análisis de Un Único CentroJoskarla MontillaNo ratings yet
- Current Advances in Esophageal 2015 Biochimica Et Biophysica Acta BBA PDocument9 pagesCurrent Advances in Esophageal 2015 Biochimica Et Biophysica Acta BBA PFlorin AchimNo ratings yet
- A Genomic StrategyDocument11 pagesA Genomic StrategyAmirahShalehaNo ratings yet
- Prevention of Contrast Induced Renal Failure NAC ReviewDocument9 pagesPrevention of Contrast Induced Renal Failure NAC Reviewnaxo128No ratings yet
- (2020) Clinical Course and Prognosis of Non-Secretory Multiple MyelomaDocument23 pages(2020) Clinical Course and Prognosis of Non-Secretory Multiple MyelomatodosobrecoronavirusNo ratings yet
- MPV SciDocument6 pagesMPV SciMikael AngelooNo ratings yet
- Pancytopenia A Clinico Hematological StudyDocument6 pagesPancytopenia A Clinico Hematological StudyUci Rahmadhani MNo ratings yet
- 19#prognostic HCC 2021Document7 pages19#prognostic HCC 2021hitashiNo ratings yet
- Texto 2Document10 pagesTexto 2jjorge160570No ratings yet
- LeukemiaDocument10 pagesLeukemiaShapira alNo ratings yet
- A Cross-Sectional Study On Evaluation of Complete Blood Count-Associated Parameters For The Diagnosis of Acute AppendicitisDocument6 pagesA Cross-Sectional Study On Evaluation of Complete Blood Count-Associated Parameters For The Diagnosis of Acute AppendicitisJordan SugiartoNo ratings yet
- The Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsDocument11 pagesThe Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsThinh VinhNo ratings yet
- Teori Eosinopenia DewasaDocument7 pagesTeori Eosinopenia DewasaNurlyanti RustamNo ratings yet
- Comprehensive Analysis of Angiogenesis Pattern and Related Immune Landscape For Individual Treatment in OsteosarcomaDocument15 pagesComprehensive Analysis of Angiogenesis Pattern and Related Immune Landscape For Individual Treatment in OsteosarcomaoudyNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Syntel Interview Questions and Answers 42895Document13 pagesSyntel Interview Questions and Answers 42895Hari PriyaNo ratings yet
- Character AnalysisDocument3 pagesCharacter AnalysisarianmedusaNo ratings yet
- Tech Connect Retail Private Limited,: Grand TotalDocument1 pageTech Connect Retail Private Limited,: Grand TotalKaranPadhaNo ratings yet
- Homelite XL 12Document21 pagesHomelite XL 12Alberto LazzarinNo ratings yet
- Chivalry of A Failed Knight Vol. 3Document175 pagesChivalry of A Failed Knight Vol. 3SETi2003No ratings yet
- Proton Arena Engine Cooling 1.5 1.8 Service ManualDocument16 pagesProton Arena Engine Cooling 1.5 1.8 Service ManualchipestNo ratings yet
- Bertrand's Postulate Proof - Michael TangDocument7 pagesBertrand's Postulate Proof - Michael Tanggauss202No ratings yet
- Orientation On The Manual For The Evaluation (Autosaved)Document31 pagesOrientation On The Manual For The Evaluation (Autosaved)Em Boquiren CarreonNo ratings yet
- 3.1 3.4 3.5 Buku WeiDocument2 pages3.1 3.4 3.5 Buku WeiMaritaNadyahNo ratings yet
- Ref: IS:875 - 1984 (Part III), Calculation of Wind Loads On BuildingsDocument4 pagesRef: IS:875 - 1984 (Part III), Calculation of Wind Loads On BuildingsRaviKiranNo ratings yet
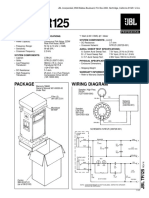
- JBL TR125Document2 pagesJBL TR125Jose Gregorio Ortega CarrilloNo ratings yet
- Programming Model of 8086Document4 pagesProgramming Model of 8086Prince VegetaNo ratings yet
- GRS CalendarDocument3 pagesGRS CalendarSACHIN KAUSHIKNo ratings yet
- Red Hat Enterprise Linux Server Operating Systems - Red HatDocument4 pagesRed Hat Enterprise Linux Server Operating Systems - Red HatBramanto MarthaNo ratings yet
- Consultants ListDocument16 pagesConsultants Listarun84No ratings yet
- Đề số 27Document5 pagesĐề số 27Mëssënġër Việt NamNo ratings yet
- Ethical-Dilemma PresentationDocument4 pagesEthical-Dilemma PresentationNaymau SuarezNo ratings yet
- Svensk Standard SS-EN ISO 6157-2:2004Document8 pagesSvensk Standard SS-EN ISO 6157-2:2004Hari PrasadNo ratings yet
- Chapter 5 Disassembly of Basic EngineDocument16 pagesChapter 5 Disassembly of Basic EnginePurnama AbhieNo ratings yet
- Invoice: Invoice Tax Date Cust Ord Acct Ref Date Due Order No. 005463400 Invoice ToDocument2 pagesInvoice: Invoice Tax Date Cust Ord Acct Ref Date Due Order No. 005463400 Invoice ToA PirzadaNo ratings yet
- Para LinguisticDocument3 pagesPara LinguisticThaiseer MohammedNo ratings yet
- Advance Numerical Mechanical SimulationDocument259 pagesAdvance Numerical Mechanical SimulationSankit SinghNo ratings yet
- Question Bank Module-1: Computer Networks 18EC71Document4 pagesQuestion Bank Module-1: Computer Networks 18EC71richa100% (1)
- SCX Series: Precision Compensated Pressure SensorsDocument10 pagesSCX Series: Precision Compensated Pressure SensorsJoel PalzaNo ratings yet
- Tuba JamilDocument1 pageTuba Jamil3J Solutions BDNo ratings yet
- Effect of Financial Ratios On Firm Performance Study of Selected Brewery Firms in NigeriaDocument8 pagesEffect of Financial Ratios On Firm Performance Study of Selected Brewery Firms in NigeriaEditor IJTSRDNo ratings yet
- Psixologiya 2 Son 2023Document265 pagesPsixologiya 2 Son 2023Otabek ShamsiddinovNo ratings yet
- Fabric v2.4 AppDevDocument27 pagesFabric v2.4 AppDevBilgehan SavguNo ratings yet