Download as pdf or txt
You might also like
- Confidential Private Placement Memorandum: Offering of Preferred Limited Liability Company InterestsDocument99 pagesConfidential Private Placement Memorandum: Offering of Preferred Limited Liability Company Interestsapi-544985744100% (1)
- Kratom Feasibility ReportDocument26 pagesKratom Feasibility ReportMichael_Roberts2019No ratings yet
- The Green Wall - Story and Photos by Stephen James Independent Investigative Journalism & Photography - VC Reporter - Ventura County Weekly - California Department of Corrections whistleblower D.J. Vodicka and his litigation against the CDC.Document8 pagesThe Green Wall - Story and Photos by Stephen James Independent Investigative Journalism & Photography - VC Reporter - Ventura County Weekly - California Department of Corrections whistleblower D.J. Vodicka and his litigation against the CDC.Stephen James - Independent Investigative Journalism & PhotographyNo ratings yet
- The Workplace - Constantly ChangingDocument30 pagesThe Workplace - Constantly ChangingLowel Orias100% (1)
- Pro-Buyer Stock Purchase AgreementDocument47 pagesPro-Buyer Stock Purchase AgreementLawrence FoxNo ratings yet
- People v. Ojeda: Colorado Court of Appeals 2019 RulingDocument141 pagesPeople v. Ojeda: Colorado Court of Appeals 2019 RulingMichael_Roberts2019No ratings yet
- Andrew Buen IndictmentDocument10 pagesAndrew Buen IndictmentMichael_Roberts2019No ratings yet
- Pablo Vazquez Charging DocumentsDocument3 pagesPablo Vazquez Charging DocumentsMichael_Roberts2019No ratings yet
- Jordan Steinke Charging DocumentsDocument2 pagesJordan Steinke Charging DocumentsMichael_Roberts2019No ratings yet
- Jennifer Lobato LawsuitDocument48 pagesJennifer Lobato LawsuitMichael_Lee_RobertsNo ratings yet
- 2008-09 Solano County Grand Jury Health and Social Services Child Abuse ReportingDocument6 pages2008-09 Solano County Grand Jury Health and Social Services Child Abuse ReportingRick ThomaNo ratings yet
- US DEA 2020 National Drug Threat AssessmentDocument100 pagesUS DEA 2020 National Drug Threat Assessmentnelson during100% (1)
- Carlos AlvarezDocument18 pagesCarlos AlvarezNeal McNamaraNo ratings yet
- Bandidos Arrest InfoDocument2 pagesBandidos Arrest InfoEmily Porter0% (1)
- IndictmentsDocument6 pagesIndictmentsABC15 NewsNo ratings yet
- Sequel LawsuitDocument9 pagesSequel LawsuitMike BrownNo ratings yet
- Fowler ComplaintDocument9 pagesFowler ComplaintWilliam BergerNo ratings yet
- Estate of John Patrick Walter v. Correctional Healthcare Companies, Et. Al.Document66 pagesEstate of John Patrick Walter v. Correctional Healthcare Companies, Et. Al.Michael_Lee_RobertsNo ratings yet
- Trujillo ComplaintDocument58 pagesTrujillo ComplaintJames JusticeNo ratings yet
- Libro Guia MethamphetamineDocument115 pagesLibro Guia MethamphetamineRoman_1988No ratings yet
- Berkeley CopWatch - The Criminalization of Copwatching - Report October 2011Document41 pagesBerkeley CopWatch - The Criminalization of Copwatching - Report October 2011aparadise2No ratings yet
- ACLU Report Documents Rampant Abuse in L.A. County JailsDocument32 pagesACLU Report Documents Rampant Abuse in L.A. County JailsSGVNewsNo ratings yet
- Dasha Fincher LawsuitDocument15 pagesDasha Fincher LawsuitEllyn SantiagoNo ratings yet
- House Republicans Fentanyl MemoDocument5 pagesHouse Republicans Fentanyl MemoAdrian NormanNo ratings yet
- Documents Detail Misconduct by L.A. Sheriff's Deputies - Documents - Los Angeles TimesDocument44 pagesDocuments Detail Misconduct by L.A. Sheriff's Deputies - Documents - Los Angeles TimesBIGBOYNo ratings yet
- Court of Appeal JudgmentDocument103 pagesCourt of Appeal JudgmentLaura WaltersNo ratings yet
- Criminal Justice Sequestration Sign-On Letter - 12-10-12 - Final With SignaturesDocument51 pagesCriminal Justice Sequestration Sign-On Letter - 12-10-12 - Final With SignaturesThe Vera Institute of JusticeNo ratings yet
- Operation Halfway House HuntersDocument21 pagesOperation Halfway House HuntersmbwegrzynNo ratings yet
- House Hearing, 109TH Congress - Comprehensively Combating Methamphetamines: Impacts On Health and The EnvironmentDocument85 pagesHouse Hearing, 109TH Congress - Comprehensively Combating Methamphetamines: Impacts On Health and The EnvironmentScribd Government DocsNo ratings yet
- Canton Ohio Police Department: Policy ManualDocument6 pagesCanton Ohio Police Department: Policy ManualRona ProudfootNo ratings yet
- Child AbuseDocument4 pagesChild AbuseIan RomanNo ratings yet
- Smith, Et Al. - IndictmentDocument20 pagesSmith, Et Al. - IndictmentWLUCTV6No ratings yet
- Moreno Money SeizureDocument20 pagesMoreno Money Seizureray sternNo ratings yet
- Russell Strong v. City and County of DenverDocument49 pagesRussell Strong v. City and County of DenverMichael_Roberts2019No ratings yet
- United States v. Lawrence Salvatore Iorizzo, 786 F.2d 52, 2d Cir. (1986)Document14 pagesUnited States v. Lawrence Salvatore Iorizzo, 786 F.2d 52, 2d Cir. (1986)Scribd Government DocsNo ratings yet
- Kelly Boren vs. The City and County of DenverDocument42 pagesKelly Boren vs. The City and County of DenverNickNo ratings yet
- Complaint Against Banditos LASD GangDocument63 pagesComplaint Against Banditos LASD GangWayl0nNo ratings yet
- Parchman Emergency MotionDocument62 pagesParchman Emergency MotionLuke R100% (1)
- Travis Barker v. WVSPDocument18 pagesTravis Barker v. WVSPjhbryan1715No ratings yet
- FM 11.14.18 - ANGELINA County - State Court Complaint - FINALDocument221 pagesFM 11.14.18 - ANGELINA County - State Court Complaint - FINALAshley SlaytonNo ratings yet
- MethDocument2 pagesMethBrandon ZennerNo ratings yet
- LE Explainer Free SpeechDocument5 pagesLE Explainer Free SpeechKristopher Trotter100% (1)
- OCSD Seth Tunstall SW AffidavitDocument15 pagesOCSD Seth Tunstall SW AffidavitLisa BartleyNo ratings yet
- Marlowe v. City and County of San Francisco Et Al.Document15 pagesMarlowe v. City and County of San Francisco Et Al.KQED NewsNo ratings yet
- Karen Garner v. City of Loveland, Et Al.Document52 pagesKaren Garner v. City of Loveland, Et Al.Michael_Roberts2019100% (1)
- Loveland Co Karen GarnerDocument52 pagesLoveland Co Karen GarnerJames JusticeNo ratings yet
- US Indictment Against Mongols Bikie GangDocument177 pagesUS Indictment Against Mongols Bikie GangABC News OnlineNo ratings yet
- Prescott Vs BCSO LawsuitDocument16 pagesPrescott Vs BCSO LawsuitDavid Ibanez100% (1)
- Looney v. Moore: Opinion Granting Defendants' Motion For Summary Judgment To Defendants in SUPPORT Study LawsuitDocument15 pagesLooney v. Moore: Opinion Granting Defendants' Motion For Summary Judgment To Defendants in SUPPORT Study LawsuitMichelle MeyerNo ratings yet
- Federal, State, and Local Authorities Arrest Seven San Antonio Eastside Blood Gang Members and Associates On Drug Trafficking ChargesDocument7 pagesFederal, State, and Local Authorities Arrest Seven San Antonio Eastside Blood Gang Members and Associates On Drug Trafficking ChargesMyTexasDaily.comNo ratings yet
- Opioid ComplaintDocument190 pagesOpioid ComplaintAnonymous 6f8RIS6No ratings yet
- List of Defendants in Arkansas White Supremacist CaseDocument9 pagesList of Defendants in Arkansas White Supremacist CaseScott Carroll100% (3)
- Dpa Drug Induced Homicide Report 0Document80 pagesDpa Drug Induced Homicide Report 0Tahsina A MalihaNo ratings yet
- Coldwater Police LawsuitDocument26 pagesColdwater Police LawsuitWWMTNo ratings yet
- Almodovar ComplaintDocument46 pagesAlmodovar ComplaintjroneillNo ratings yet
- LawsuitDocument193 pagesLawsuitAnonymous u5mW3lhyNo ratings yet
- EDNY IndictmentDocument33 pagesEDNY IndictmentDavid Oscar MarkusNo ratings yet
- SW 54 Probable Cause RedactedDocument12 pagesSW 54 Probable Cause Redactedmark.stevensNo ratings yet
- Christopher Cooper and Shelley Smith Vs PfizerDocument11 pagesChristopher Cooper and Shelley Smith Vs PfizerNick100% (1)
- United States v. Justin A. Volpe, 224 F.3d 72, 2d Cir. (2000)Document9 pagesUnited States v. Justin A. Volpe, 224 F.3d 72, 2d Cir. (2000)Scribd Government DocsNo ratings yet
- Turner Et Al Trial - Press ReleaseDocument2 pagesTurner Et Al Trial - Press ReleaseWTVC NewsChannel 9No ratings yet
- Nearly 30K Drunken Driving Cases in Mass. in Jeopardy Over Faulty Breathalyzer Tests, SJC SaysDocument46 pagesNearly 30K Drunken Driving Cases in Mass. in Jeopardy Over Faulty Breathalyzer Tests, SJC SaysFox Boston StaffNo ratings yet
- Estate of Jeffrey Scott Lillis v. Correct Care Solutions LLC, Et. Al.Document42 pagesEstate of Jeffrey Scott Lillis v. Correct Care Solutions LLC, Et. Al.Michael_Lee_RobertsNo ratings yet
- Estate of Tomas Beauford v. Mesa County, Colorado, Et. Al.Document45 pagesEstate of Tomas Beauford v. Mesa County, Colorado, Et. Al.Michael_Lee_RobertsNo ratings yet
- EstateDocument38 pagesEstateMichael_Lee_RobertsNo ratings yet
- Dillon Blodgett Complaint and Jury DemandDocument27 pagesDillon Blodgett Complaint and Jury DemandMichael_Lee_RobertsNo ratings yet
- Denver Police Officer Cody Lane 2020 Discipline LetterDocument7 pagesDenver Police Officer Cody Lane 2020 Discipline LetterMichael_Roberts2019No ratings yet
- Denver Police Officer Cody Lane Internal-Affairs History SummaryDocument2 pagesDenver Police Officer Cody Lane Internal-Affairs History SummaryMichael_Roberts2019No ratings yet
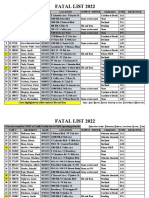
- Denver Traffic Fatalities List For 2022Document5 pagesDenver Traffic Fatalities List For 2022Michael_Roberts2019No ratings yet
- Brandon Ramos IndictmentDocument7 pagesBrandon Ramos IndictmentMichael_Roberts2019No ratings yet
- Denver Crime Statistics by Neighborhood in 2022Document17 pagesDenver Crime Statistics by Neighborhood in 2022Michael_Roberts2019No ratings yet
- Kratom Feasibility Report SupplementDocument92 pagesKratom Feasibility Report SupplementMichael_Roberts2019No ratings yet
- Anderson Lee Aldrich Charges, Part 1Document26 pagesAnderson Lee Aldrich Charges, Part 1Michael_Roberts2019No ratings yet
- People v. Ojeda: Colorado Supreme Court 2022 OpinionDocument25 pagesPeople v. Ojeda: Colorado Supreme Court 2022 OpinionMichael_Roberts2019No ratings yet
- Ruby Johnson v. Gary StaabDocument15 pagesRuby Johnson v. Gary StaabMichael_Roberts2019No ratings yet
- Anderson Lee Aldrich Charges, Part 3Document27 pagesAnderson Lee Aldrich Charges, Part 3Michael_Roberts2019No ratings yet
- Anderson Lee Aldrich AffidavitDocument5 pagesAnderson Lee Aldrich AffidavitMichael_Roberts2019100% (1)
- Dominick v. City of Denver: Motion To DismissDocument16 pagesDominick v. City of Denver: Motion To DismissMichael_Roberts2019No ratings yet
- Kyle Gould IndictmentDocument10 pagesKyle Gould IndictmentMichael_Roberts2019No ratings yet
- Marquis Dominick, Et Al., v. City and County of Denver, Et Al.Document70 pagesMarquis Dominick, Et Al., v. City and County of Denver, Et Al.Michael_Roberts2019No ratings yet
- Michael Driscoll v. City and County of Denver, Et Al.Document53 pagesMichael Driscoll v. City and County of Denver, Et Al.Michael_Roberts2019No ratings yet
- Eric Brandt v. City and County of Denver, Et Al.Document32 pagesEric Brandt v. City and County of Denver, Et Al.Michael_Roberts2019No ratings yet
- Yareni Rios-Gonzalez Charging DocumentsDocument2 pagesYareni Rios-Gonzalez Charging DocumentsMichael_Roberts2019No ratings yet
- Victor Bentley Arrest AffidavitDocument5 pagesVictor Bentley Arrest AffidavitMichael_Roberts2019No ratings yet
- Aaron Patrick v. National Football League, Et Al.Document19 pagesAaron Patrick v. National Football League, Et Al.Michael_Roberts2019No ratings yet
- Denver Public Schools: November 2022 School Unification PlanDocument51 pagesDenver Public Schools: November 2022 School Unification PlanMichael_Roberts2019No ratings yet
- Kayla Mooney Arrest AffidavitDocument5 pagesKayla Mooney Arrest AffidavitMichael_Roberts2019No ratings yet
- Denver Metro Association of Realtors: November 2022 Market Trends ReportDocument29 pagesDenver Metro Association of Realtors: November 2022 Market Trends ReportMichael_Roberts2019No ratings yet
- Trevor Hughes: Denver Settlement AgreementDocument5 pagesTrevor Hughes: Denver Settlement AgreementMichael_Roberts2019No ratings yet
- Sergio and Andrew Rodarte IndictmentDocument7 pagesSergio and Andrew Rodarte IndictmentMichael_Roberts2019No ratings yet
- Trevor Hughes v. Denver, Et Al.Document55 pagesTrevor Hughes v. Denver, Et Al.Michael_Roberts2019No ratings yet
- Consolidated Invoice - Natixis Real Estate Capital LLC, A Delaware Limited Liability Company - Project TPG Warehouse FacilityDocument5 pagesConsolidated Invoice - Natixis Real Estate Capital LLC, A Delaware Limited Liability Company - Project TPG Warehouse FacilityrhenkeNo ratings yet
- Benevis Bankruptcy Doc 33 - Exhibit 1 PDFDocument57 pagesBenevis Bankruptcy Doc 33 - Exhibit 1 PDFDentist The MenaceNo ratings yet
- Lahore Smart CityDocument2 pagesLahore Smart CitychatroomvistaNo ratings yet
- Complete Download Financial Management Principles and Applications 12th Edition Titman Test BankDocument27 pagesComplete Download Financial Management Principles and Applications 12th Edition Titman Test BankRey Lister JuarezNo ratings yet
- Precision Hawk Drone Business Guide 2018Document33 pagesPrecision Hawk Drone Business Guide 2018Allan Z McMaken100% (5)
- NIMC EXPRESSION OF INTEREST Full PG B&W-1Document1 pageNIMC EXPRESSION OF INTEREST Full PG B&W-1SETHNo ratings yet
- Building The Business: Because Learning Changes EverythingDocument37 pagesBuilding The Business: Because Learning Changes EverythingMax SinghNo ratings yet
- Rick Fox ComplaintDocument162 pagesRick Fox ComplaintGMG EditorialNo ratings yet
- FL2533 R29 Ae 2023 01 26 Final Er Certainteed Modbit FL2533-R29Document79 pagesFL2533 R29 Ae 2023 01 26 Final Er Certainteed Modbit FL2533-R29Irene BorgesNo ratings yet
- Prolific Energy LLCDocument5 pagesProlific Energy LLCprolificenergyNo ratings yet
- Multiple Choice Questions of Business ClassificationDocument3 pagesMultiple Choice Questions of Business ClassificationMarkNo ratings yet
- Understanding TrademarksDocument2 pagesUnderstanding TrademarksChuck EastNo ratings yet
- Economic-Impact - Resort Industry Student3Document30 pagesEconomic-Impact - Resort Industry Student3Jhen BonNo ratings yet
- Us 2022 Tax UpdateDocument19 pagesUs 2022 Tax Updateapi-263318846No ratings yet
- FDIC V Bear Sterns 12-Cv-05360, S.D.N.Y. DocketDocument28 pagesFDIC V Bear Sterns 12-Cv-05360, S.D.N.Y. Docketlarry-612445No ratings yet
- Corporation. The LLC Will Be Treated As A Corporation As of The Effective Date of The SDocument2 pagesCorporation. The LLC Will Be Treated As A Corporation As of The Effective Date of The SJhonel PilapilNo ratings yet
- Rihanna ComplaintDocument26 pagesRihanna ComplaintgmaddausNo ratings yet
- Caesars Entertainment LawsuitDocument35 pagesCaesars Entertainment LawsuitGreg SaulmonNo ratings yet
- Belava v. SkinAct - ComplaintDocument12 pagesBelava v. SkinAct - ComplaintSarah BursteinNo ratings yet
- 99cents Store AppDocument2 pages99cents Store AppAnonymous d4PK3FNo ratings yet
- TruckSpace PackageDocument3 pagesTruckSpace PackageTom MillerNo ratings yet
- 2018-09-06 DOC Re Statement of Information (DSJ Real Estate Holdings, LLC)Document2 pages2018-09-06 DOC Re Statement of Information (DSJ Real Estate Holdings, LLC)Doo Soo KimNo ratings yet
- Unit 4 Seed ModelDocument8 pagesUnit 4 Seed ModelJastine AnneNo ratings yet
- An Introduction To The Foundations of Financial ManagementDocument25 pagesAn Introduction To The Foundations of Financial ManagementAhmed El KhateebNo ratings yet
- Prospects Potentials of Mining Industry in OmanDocument8 pagesProspects Potentials of Mining Industry in OmanrajataimurNo ratings yet
- Different Types of Legal Entity DocumentsDocument4 pagesDifferent Types of Legal Entity DocumentsКристи АбдушаNo ratings yet
- Orianne Collins and Thomas Bates Response To Phil Collins ComplaintDocument25 pagesOrianne Collins and Thomas Bates Response To Phil Collins ComplaintPeterBurkeNo ratings yet