Download as pdf or txt
You might also like
- ANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFDocument8 pagesANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFRong LiuNo ratings yet
- (583950958) Journal Leucopenia Treatment Effiicacy NPCDocument8 pages(583950958) Journal Leucopenia Treatment Effiicacy NPCDaniel HoseaNo ratings yet
- Primary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyDocument7 pagesPrimary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyLuvita Amallia SyadhatinNo ratings yet
- Characteristics, Treatment Patterns and Outcomes of Patients With Small Cell Lung Cancer-A Retrospective Single Institution AnalysisDocument4 pagesCharacteristics, Treatment Patterns and Outcomes of Patients With Small Cell Lung Cancer-A Retrospective Single Institution AnalysismaleticjNo ratings yet
- Prognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentDocument7 pagesPrognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentChairul Nurdin AzaliNo ratings yet
- Otolaryngol - Head Neck Surg - 2023 - Patel - Elective Neck Dissection For cT1 4 N0M0 Head and Neck Verrucous CarcinomaDocument13 pagesOtolaryngol - Head Neck Surg - 2023 - Patel - Elective Neck Dissection For cT1 4 N0M0 Head and Neck Verrucous CarcinomadrsubhajitfaciomaxsurgeonNo ratings yet
- The Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFDocument7 pagesThe Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFJorge JaraNo ratings yet
- Bacciu 2013Document10 pagesBacciu 2013AshokNo ratings yet
- Lung Cancer Current Therapies and New Targeted TreatmentsDocument13 pagesLung Cancer Current Therapies and New Targeted TreatmentsWlad PaCaNo ratings yet
- 1919 FullDocument6 pages1919 FullEMIRZA NUR WICAKSONONo ratings yet
- Cancer - 2003 - Greenberg - Extent of Extracapsular SpreadDocument7 pagesCancer - 2003 - Greenberg - Extent of Extracapsular SpreadVaredis T.No ratings yet
- Prognostic Significance of Hematologic Markers in Patients With Head and Neck Squamous Cell CarcinomasDocument11 pagesPrognostic Significance of Hematologic Markers in Patients With Head and Neck Squamous Cell CarcinomasLeyla M HattaNo ratings yet
- 3 The Risk of Second Primary Tumors in Head and Neck Cancer. A Systematic ReviewDocument11 pages3 The Risk of Second Primary Tumors in Head and Neck Cancer. A Systematic Review2211801733No ratings yet
- 10.1007@s00405 020 06019 2Document12 pages10.1007@s00405 020 06019 2luca totongNo ratings yet
- Metastase Cerebrale 3Document9 pagesMetastase Cerebrale 3Nouhad BenNo ratings yet
- Prognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated RadiotherapyDocument7 pagesPrognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated Radiotherapypp kabsemarangNo ratings yet
- Atm 07 14 323Document9 pagesAtm 07 14 323Ethel GeanNo ratings yet
- Dziegielewski2017 Adressing The Contralateral TonsilDocument8 pagesDziegielewski2017 Adressing The Contralateral Tonsilnatalia.gallinoNo ratings yet
- Cancers-14-03105-With-CoverDocument16 pagesCancers-14-03105-With-CoverNovi OktaviantiNo ratings yet
- Extracranial ChondrosarcomaDocument8 pagesExtracranial ChondrosarcomaSyedNo ratings yet
- Me Hanna 2016Document11 pagesMe Hanna 2016eswarNo ratings yet
- Temporal Bone Carcinoma Classical Prognostic Vari - 2016 - Reports of PracticalDocument5 pagesTemporal Bone Carcinoma Classical Prognostic Vari - 2016 - Reports of PracticalOana VarvariNo ratings yet
- Prognostic Nomogram For Patients With Tongue Squamous Cell Carcinoma: A SEER-based StudyDocument15 pagesPrognostic Nomogram For Patients With Tongue Squamous Cell Carcinoma: A SEER-based Studymahmud.meftahNo ratings yet
- 1 s2.0 S0748798321001232 MainDocument12 pages1 s2.0 S0748798321001232 MainRoberto BarronNo ratings yet
- J Joms 2016 03 037Document12 pagesJ Joms 2016 03 037Gisela LalitaNo ratings yet
- OCOXIN Head Neck CancerDocument12 pagesOCOXIN Head Neck Cancerdarmayanti ibnuNo ratings yet
- GP 96Document24 pagesGP 96Study MaterialNo ratings yet
- Radiotherapy and OncologyDocument6 pagesRadiotherapy and OncologyIntan Kartika NursyahbaniNo ratings yet
- Prognostic Factors Affecting Survial and Recurrence in Patientes With Early Cervical Squamous Cell Cancer Following Radical HTDocument13 pagesPrognostic Factors Affecting Survial and Recurrence in Patientes With Early Cervical Squamous Cell Cancer Following Radical HTfernandallmagalhaesNo ratings yet
- Keratocystic Odontogenic Tumour in A Hong Kong Community: The Clinical and Radiological FeaturesDocument9 pagesKeratocystic Odontogenic Tumour in A Hong Kong Community: The Clinical and Radiological FeaturesYenita AdetamaNo ratings yet
- EBM 2018 - Head and CancersDocument136 pagesEBM 2018 - Head and CancersChandramohan SettyNo ratings yet
- 10.12921 cmst.2006.12.02.143-147 MoczkoDocument5 pages10.12921 cmst.2006.12.02.143-147 Moczkoshital shermaleNo ratings yet
- Cancers 13 04912Document12 pagesCancers 13 04912mirzaNo ratings yet
- Ebm IpaDocument7 pagesEbm IparivahazmarNo ratings yet
- Effets Pronostiques de La Chirurgie Ou de La Radiothérapie Sur Le Carcinome Adénoïde Kystique de La Tête Et Du CouDocument17 pagesEffets Pronostiques de La Chirurgie Ou de La Radiothérapie Sur Le Carcinome Adénoïde Kystique de La Tête Et Du CouMamadou DIENENo ratings yet
- Seminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresDocument13 pagesSeminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresseruniallisaaslimNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Piis0167814019331123 230304 134522Document7 pagesPiis0167814019331123 230304 134522Samuel Kelvin RuslimNo ratings yet
- Systemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewDocument11 pagesSystemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewLorena Sánchez PérezNo ratings yet
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaNo ratings yet
- Development and Validation of A Prognostic Model For Predicting Overall Survival in Patients With Bladder Cancer: A SEER-Based StudyDocument10 pagesDevelopment and Validation of A Prognostic Model For Predicting Overall Survival in Patients With Bladder Cancer: A SEER-Based Studymahmud.meftahNo ratings yet
- Cancer de HipofaringeDocument8 pagesCancer de HipofaringeBrandaNo ratings yet
- Metastasis of Differentiated Thyroid Carcinoma A Descriptive Study of 75 PatientsDocument10 pagesMetastasis of Differentiated Thyroid Carcinoma A Descriptive Study of 75 PatientsAthenaeum Scientific PublishersNo ratings yet
- Wa0011Document4 pagesWa0011PatrickNicholsNo ratings yet
- Esophageal Cancer Recurrence Patterns and Implicati 2013 Journal of ThoracicDocument5 pagesEsophageal Cancer Recurrence Patterns and Implicati 2013 Journal of ThoracicFlorin AchimNo ratings yet
- Head NeckDocument8 pagesHead NeckerandolphsavageNo ratings yet
- Argiris 2008Document15 pagesArgiris 2008Lisbeth TurraNo ratings yet
- Elective Neck Irradiation N0 Neck Jia KouDocument13 pagesElective Neck Irradiation N0 Neck Jia KouSanjog SinghNo ratings yet
- Submandibular Salivary Gland Tumors: Clinical Course and Outcome of A 20-Year Multicenter StudyDocument4 pagesSubmandibular Salivary Gland Tumors: Clinical Course and Outcome of A 20-Year Multicenter StudyDiornald MogiNo ratings yet
- 2017 Diagnostic Relevance of Metastatic Renal Cell Carcinoma in The Head and Neck An Evaluation of 22 Cases in 671 PatientsDocument7 pages2017 Diagnostic Relevance of Metastatic Renal Cell Carcinoma in The Head and Neck An Evaluation of 22 Cases in 671 PatientsAlfonsoSánchezNo ratings yet
- Rcsann 2016 0300Document4 pagesRcsann 2016 0300Siti Ayu kamsiahNo ratings yet
- P. Wang Et Al.2019Document6 pagesP. Wang Et Al.2019Mai M. AlshalNo ratings yet
- Outcomes Following Surgery For Colorectal Live 2016 International Journal ofDocument1 pageOutcomes Following Surgery For Colorectal Live 2016 International Journal ofoomculunNo ratings yet
- 10 1016@j Critrevonc 2020 102962Document16 pages10 1016@j Critrevonc 2020 102962bouh aichetouNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- Jurnal 4 Prognosis PDFDocument6 pagesJurnal 4 Prognosis PDFSurya DharmadiNo ratings yet
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 pagesHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsNo ratings yet
- Zumsteg Et Al 2015Document8 pagesZumsteg Et Al 2015Alyssa Anne GrandaNo ratings yet
- Gastrointestinal Malignancies: A Practical Guide on Treatment TechniquesFrom EverandGastrointestinal Malignancies: A Practical Guide on Treatment TechniquesSuzanne RussoNo ratings yet
- Follicular Lymphoma: Current Management and Novel ApproachesFrom EverandFollicular Lymphoma: Current Management and Novel ApproachesNathan H. FowlerNo ratings yet
- Li Et Al., 2017Document5 pagesLi Et Al., 2017James BondNo ratings yet
- Uddin Et Al., 2022Document4 pagesUddin Et Al., 2022James BondNo ratings yet
- Second Primary OSCC 666Document5 pagesSecond Primary OSCC 666James BondNo ratings yet
- Second Primary OSCC 222Document2 pagesSecond Primary OSCC 222James BondNo ratings yet
- Second Primary OSCC 55Document1 pageSecond Primary OSCC 55James BondNo ratings yet
- Second Primary OSCC 2Document6 pagesSecond Primary OSCC 2James BondNo ratings yet
- Journal Second Primary OSCCDocument8 pagesJournal Second Primary OSCCJames BondNo ratings yet
- Second Primary TumorDocument7 pagesSecond Primary TumorJames BondNo ratings yet
- Survival AnalysisDocument16 pagesSurvival AnalysisMeNo ratings yet
- AlcoooDocument8 pagesAlcooofilimon ioanaNo ratings yet
- Analisis Aitem KLMPK 10Document5 pagesAnalisis Aitem KLMPK 10yola amanthaNo ratings yet
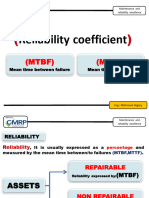
- Reliability Coefficient (MTBF, MTTF)Document9 pagesReliability Coefficient (MTBF, MTTF)Mahmoud ElemamNo ratings yet
- Premium Calculation On Health Insurance Implementing DeductibleDocument8 pagesPremium Calculation On Health Insurance Implementing DeductibleParakh AhoojaNo ratings yet
- SurvLIME A Method For Explaining Machine Learning Survival ModelsDocument20 pagesSurvLIME A Method For Explaining Machine Learning Survival Modelsh4md4nNo ratings yet
- Artificial Intelligence in Cancer Diagnosis and Prognosis: Opportunities and ChallengesDocument26 pagesArtificial Intelligence in Cancer Diagnosis and Prognosis: Opportunities and ChallengesameyaNo ratings yet
- Sample Survival NokeyDocument6 pagesSample Survival NokeyKamya AndrewNo ratings yet
- Hazard Rate Theory and InferenceDocument296 pagesHazard Rate Theory and InferencedwimahrNo ratings yet
- Statistical Lifetime ModelsDocument197 pagesStatistical Lifetime Modelsgmert58No ratings yet
- Survival - Notes (Lecture 6)Document27 pagesSurvival - Notes (Lecture 6)Kimondo KingNo ratings yet
- SR A38x Clearfog Base Rev1.1 MTBFDocument18 pagesSR A38x Clearfog Base Rev1.1 MTBFAnonymous wz3pZ5No ratings yet
- Reliability With Cronbach's Alpha If Item DeletedDocument2 pagesReliability With Cronbach's Alpha If Item DeletedGede SukadanaNo ratings yet
- IandF CS2 Paper A 202204 Examiner ReportDocument13 pagesIandF CS2 Paper A 202204 Examiner ReportAlvis LeeNo ratings yet
- Shane & Delmar (2004) - Planning For The Market - Business Planning Before Marketing and The Continuation of Organizing EffortsDocument19 pagesShane & Delmar (2004) - Planning For The Market - Business Planning Before Marketing and The Continuation of Organizing EffortsRos FlannelaNo ratings yet
- Reliability Functions of Generalized Log Normal Model - Gupta-Lvin PDFDocument8 pagesReliability Functions of Generalized Log Normal Model - Gupta-Lvin PDFgmitsutaNo ratings yet
- Survival Analysis: Ani KatchovaDocument10 pagesSurvival Analysis: Ani KatchovaShahabuddin ProdhanNo ratings yet
- Ebeling-Chapter 4.1 Part I-EbelingDocument37 pagesEbeling-Chapter 4.1 Part I-Ebelingimagine dragonNo ratings yet
- Survival Distributions in RDocument3 pagesSurvival Distributions in Rpuja_malhNo ratings yet
- CT4 Models PDFDocument6 pagesCT4 Models PDFVignesh Srinivasan0% (1)
- The Kaplan-Meier Estimate of The Survival FunctionDocument23 pagesThe Kaplan-Meier Estimate of The Survival Functionrodicasept1967No ratings yet
- Belajar Menghitung ReliabilityDocument103 pagesBelajar Menghitung ReliabilityIkhsan LyNo ratings yet
- Introduction To Reliability Engineering: Prof. Neeraj Kumar GoyalDocument712 pagesIntroduction To Reliability Engineering: Prof. Neeraj Kumar GoyalraidhabyanNo ratings yet
- Paper 2Document5 pagesPaper 2fernanda cornejoNo ratings yet
- Cohort StudiesDocument5 pagesCohort StudiesIlma NafiaNo ratings yet
- MTBF MTTR CalculationDocument2 pagesMTBF MTTR Calculationluc.ayresNo ratings yet
- ReliabilityDocument13 pagesReliabilityAbdulateaf Abdulrazig SattiNo ratings yet
- International Phase 3 Study of Azacitidine Vs Conventional Care Regimens in Older Patients With Newly Diagnosed AML With 30% BlastsDocument9 pagesInternational Phase 3 Study of Azacitidine Vs Conventional Care Regimens in Older Patients With Newly Diagnosed AML With 30% BlastsOrxan HumbetovNo ratings yet
- Laboratory Turnaround TimeDocument17 pagesLaboratory Turnaround TimeNicole HoNo ratings yet