Download as pdf or txt
You might also like
- Carbohydrates WorksheetDocument2 pagesCarbohydrates WorksheetEllaine Salcedo31% (13)
- Test Bank For Molecular Biology 5th Edition Robert WeaverDocument11 pagesTest Bank For Molecular Biology 5th Edition Robert WeaverMelindaYangtpeg100% (37)
- Non Protein CompoundsDocument64 pagesNon Protein CompoundsAbigail Mayled LausNo ratings yet
- NeonatalNutritionConversionTable PDFDocument4 pagesNeonatalNutritionConversionTable PDFEnthusNo ratings yet
- Inborn Error of MetabolismDocument27 pagesInborn Error of MetabolismNarayan GhimireNo ratings yet
- Case Reports Gout Vitamins MineralsDocument23 pagesCase Reports Gout Vitamins MineralsNasreen SultanaNo ratings yet
- Chapter X - Mechanism of Protein MetabolismDocument30 pagesChapter X - Mechanism of Protein MetabolismAngelo AngelesNo ratings yet
- Metabolic DisordersDocument59 pagesMetabolic DisordersKeannu Havana100% (1)
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomNo ratings yet
- Urine AnalysisDocument42 pagesUrine AnalysisajaysomNo ratings yet
- Uremic Toxicity: Kopple J. D. and Massry S. D.:Nutritional Management of Renal Disease, p97-190Document34 pagesUremic Toxicity: Kopple J. D. and Massry S. D.:Nutritional Management of Renal Disease, p97-190Muhammad Yusuf Arief AkbarNo ratings yet
- Investigation of Amino Acids DisordersDocument4 pagesInvestigation of Amino Acids Disorderskiedd_04100% (1)
- Amino Acid Metabolism Disorders Series 2Document5 pagesAmino Acid Metabolism Disorders Series 2kiedd_04No ratings yet
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- AnaemiaDocument71 pagesAnaemiaREETHUNo ratings yet
- Sulphur Containing AminoacidsDocument36 pagesSulphur Containing AminoacidsSaloni SaloniNo ratings yet
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- Chemical Examination of UrineDocument46 pagesChemical Examination of Urineubaidnaveed0323No ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument45 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- USMD, CSF, SEMEN - Professor'sDocument10 pagesUSMD, CSF, SEMEN - Professor'sMartin ClydeNo ratings yet
- Chemical Examination of UrineDocument46 pagesChemical Examination of UrineH GondaliyaNo ratings yet
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarNo ratings yet
- 3 - Chapter 3 Amino Acids and Protein Metabolism 2Document33 pages3 - Chapter 3 Amino Acids and Protein Metabolism 2عزوز الشمريNo ratings yet
- Ketosis & KetoacidosisDocument23 pagesKetosis & KetoacidosisrohishaakNo ratings yet
- Uric PDFDocument28 pagesUric PDFNgân TrươngNo ratings yet
- Exam Endocrine Dentistry KrokDocument7 pagesExam Endocrine Dentistry KrokRachid HissaneNo ratings yet
- Calcium, Phosphate, MagnesiumDocument55 pagesCalcium, Phosphate, MagnesiumUdochukwu EnebeNo ratings yet
- Wa0028.Document46 pagesWa0028.Ziyadan AtiqueNo ratings yet
- Hyper AmmoniaDocument10 pagesHyper AmmoniaThamizh Arasi Vinayagam100% (1)
- 4 Protein ReviewDocument87 pages4 Protein Reviewmika de guzmanNo ratings yet
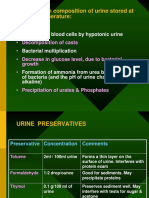
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Uric AcidDocument28 pagesUric AcidAya100% (1)
- Fate of Carbon SkeletonDocument42 pagesFate of Carbon Skeletonhassanainshahi13No ratings yet
- NM 22 Urate 2007Document35 pagesNM 22 Urate 2007api-26938624No ratings yet
- Drugs For GoutDocument29 pagesDrugs For GoutSsempijja Joshua BuyinzaNo ratings yet
- Acute Complications of DMDocument57 pagesAcute Complications of DMMalueth AnguiNo ratings yet
- Uric AcidDocument13 pagesUric Acidphoto copyhemnNo ratings yet
- Liver DiseasesDocument24 pagesLiver DiseasesAbdo HaiderNo ratings yet
- Urine Screening For Metabolic DisordersDocument55 pagesUrine Screening For Metabolic DisordersGlormina Asprec AvenaNo ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument42 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- Non-Protein Nitrogenous Constituents of Blood - Urea, Uric Acid EtcDocument50 pagesNon-Protein Nitrogenous Constituents of Blood - Urea, Uric Acid EtcBobskinnyNo ratings yet
- Inborn Errors of Amino Acid MetabolismDocument65 pagesInborn Errors of Amino Acid MetabolismSantino MajokNo ratings yet
- Diet GoutDocument50 pagesDiet GoutFaishal Muhammad Arrosyad100% (1)
- Metabolic Disorder Obtain Plasma Ammonia High Normal Obtain Blood PH and C02 Obtain Blood PH and C02Document14 pagesMetabolic Disorder Obtain Plasma Ammonia High Normal Obtain Blood PH and C02 Obtain Blood PH and C02Grace LazarragaNo ratings yet
- بايو عملي م١Document5 pagesبايو عملي م١tm31880388No ratings yet
- LM 15 Inborn ErrorsDocument18 pagesLM 15 Inborn ErrorsRafat S ZriqiNo ratings yet
- Inborn Errors of Metabolism IEM 1Document36 pagesInborn Errors of Metabolism IEM 1bhaskar chinnanandhi100% (1)
- Management of Icterus Viewed From The Clinical andDocument57 pagesManagement of Icterus Viewed From The Clinical andzanafiraNo ratings yet
- Inborn Errors of Metabolism Student LectureDocument81 pagesInborn Errors of Metabolism Student LectureFavourNo ratings yet
- Presentation 7Document12 pagesPresentation 7G.gNo ratings yet
- Qualitative Analysis of Normal and Abnormal UrineDocument28 pagesQualitative Analysis of Normal and Abnormal UrineVirendra JoshiNo ratings yet
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNo ratings yet
- Non-Protein Nitrogen (NPN) CompoundsDocument34 pagesNon-Protein Nitrogen (NPN) CompoundsAhmed GaberNo ratings yet
- Amino Acidss & AminoacidopathiesDocument55 pagesAmino Acidss & AminoacidopathiesMustafa KhandgawiNo ratings yet
- Hypomagnesemia & HypermagnesemiaDocument18 pagesHypomagnesemia & HypermagnesemiaLanzen DragneelNo ratings yet
- Hepatic Encephalopathy: Dr. Reena Residant Ward 6Document31 pagesHepatic Encephalopathy: Dr. Reena Residant Ward 6padmaNo ratings yet
- Fluid & Electrolyte ImbalanceDocument47 pagesFluid & Electrolyte ImbalanceBijeta ThapaNo ratings yet
- Fatty Acid Oxidation Part 2Document38 pagesFatty Acid Oxidation Part 2mudhugurigirishmaNo ratings yet
- Chem Lect Unit 7 Kidney FunctionDocument38 pagesChem Lect Unit 7 Kidney FunctionMustafa KhandgawiNo ratings yet
- Aminoacidopathies OCT2008 - Clinical Chem Lect 3rd Yr MT - 1st SemesterDocument19 pagesAminoacidopathies OCT2008 - Clinical Chem Lect 3rd Yr MT - 1st SemesterburdihanNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Malarial Parasites LetterheadDocument1 pageMalarial Parasites LetterheadChudasama DhruvrajsinhNo ratings yet
- JaundiceDocument17 pagesJaundiceChudasama DhruvrajsinhNo ratings yet
- Pharmaceutics, Packaging of PharmaceuticalsDocument8 pagesPharmaceutics, Packaging of PharmaceuticalsChudasama DhruvrajsinhNo ratings yet
- ChemistryDocument4 pagesChemistryChudasama DhruvrajsinhNo ratings yet
- Dietary Supplements, Nutraceuticals, Food Supplements, Food Drug InteractionsDocument39 pagesDietary Supplements, Nutraceuticals, Food Supplements, Food Drug InteractionsChudasama DhruvrajsinhNo ratings yet
- UreacycleDocument18 pagesUreacycleChudasama DhruvrajsinhNo ratings yet
- Sodium and Potassium - Atp Ase PumpDocument18 pagesSodium and Potassium - Atp Ase PumpYaswanthyadavNo ratings yet
- PDocument4 pagesPIca zaharaNo ratings yet
- Nutrition FactsDocument10 pagesNutrition FactsVignesh SelvarajNo ratings yet
- Beta Oxidation of Fatty AcidDocument27 pagesBeta Oxidation of Fatty Acidnegurii hearteuNo ratings yet
- Macromolecules 1Document31 pagesMacromolecules 1api-267079239No ratings yet
- Module (Amino Acids and Proteins)Document18 pagesModule (Amino Acids and Proteins)Edgie JunelaNo ratings yet
- Test Bank For Molecular Biology of The Cell 5th Edition Bruce AlbertsDocument36 pagesTest Bank For Molecular Biology of The Cell 5th Edition Bruce Albertsbrokeazarole6rv8pl100% (41)
- Biopharm - MidtermDocument4 pagesBiopharm - MidtermLinhNguyeNo ratings yet
- Metabolism: Written by TutorDocument4 pagesMetabolism: Written by TutorRyan Carlo CondeNo ratings yet
- Journal of The American College of Nutrition 2008Document8 pagesJournal of The American College of Nutrition 2008germanNo ratings yet
- Medicinal Chemistry and Molecular Pharmacology of GABA-C ReceptorsDocument12 pagesMedicinal Chemistry and Molecular Pharmacology of GABA-C ReceptorsHuallpa Samaniego SebastianNo ratings yet
- Molecular Biology All McqsDocument76 pagesMolecular Biology All Mcqssanullah123khan.13No ratings yet
- MBC 201 Nature of Biomolecules, Basic Concept of Metabolism, Integration of Intermediary Metabolism and Energy Generation.Document13 pagesMBC 201 Nature of Biomolecules, Basic Concept of Metabolism, Integration of Intermediary Metabolism and Energy Generation.Aina AdesolaNo ratings yet
- Genetics - For NEET, Medical & B - Sanjay KhareDocument139 pagesGenetics - For NEET, Medical & B - Sanjay Khareteamindian gamersNo ratings yet
- Viva in Biochemistry - 2E MN Chatterjea PDFDocument488 pagesViva in Biochemistry - 2E MN Chatterjea PDFSuzan Yadikar100% (4)
- Dna and Rna DLLDocument2 pagesDna and Rna DLLHeidie BalabboNo ratings yet
- Datasheet 211108Document2 pagesDatasheet 211108Magic PrinceNo ratings yet
- Selectra IDocument18 pagesSelectra IEnrique DuarteNo ratings yet
- Amali 2 BIDocument4 pagesAmali 2 BIJun Hong TeeNo ratings yet
- The Influence of Feed Supply Time On The Fatty Acid ProfileDocument5 pagesThe Influence of Feed Supply Time On The Fatty Acid ProfileSumoharjo La MpagaNo ratings yet
- Chem EnzymesDocument18 pagesChem Enzymesonnetwo10No ratings yet
- Ali Raza Tariq-Bz486811-Bio-Chemistry-4425-PresentationDocument14 pagesAli Raza Tariq-Bz486811-Bio-Chemistry-4425-PresentationM Ali SheikhNo ratings yet
- Chapter 22 - Oxidation of Fatty Acids - KetogenesisDocument14 pagesChapter 22 - Oxidation of Fatty Acids - Ketogenesisrenzo041199No ratings yet
- Bio MoleculesDocument7 pagesBio MoleculesJatt PandherNo ratings yet
- Karya Tulis IlmiahDocument31 pagesKarya Tulis IlmiahIndri DinovaNo ratings yet
- Learning Objectives: DR Finney The Innate Immune System, CMMB527 W22Document8 pagesLearning Objectives: DR Finney The Innate Immune System, CMMB527 W22rtm haiderNo ratings yet
- Lehninger Principles of Biochemistry - Albert Lester LehningerDocument2 pagesLehninger Principles of Biochemistry - Albert Lester LehningerasisthelpNo ratings yet