Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hyundai Getz 2003 1 1 1 3 PDFDocument109 pagesHyundai Getz 2003 1 1 1 3 PDFSuyog patil100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Instrumental Methods For The Analysis and Identification of Bioactive MoleculesDocument370 pagesInstrumental Methods For The Analysis and Identification of Bioactive MoleculesSuyog patilNo ratings yet
- Local Youth Development PlanDocument7 pagesLocal Youth Development PlanClaire Janiola100% (5)
- About Cogent™ HPLC Columns - General Information - MicroSolv Technology Corp MTC-USADocument2 pagesAbout Cogent™ HPLC Columns - General Information - MicroSolv Technology Corp MTC-USASuyog patilNo ratings yet
- Ascentis Express 5 Micron - A Fused-Core Particle HPLC Column For Faster HPLC Separations With No Backpressure ConcernsDocument2 pagesAscentis Express 5 Micron - A Fused-Core Particle HPLC Column For Faster HPLC Separations With No Backpressure ConcernsSuyog patilNo ratings yet
- Advances in HPLC Stationary Phases in Monolithic HPLC ColumnsDocument7 pagesAdvances in HPLC Stationary Phases in Monolithic HPLC ColumnsSuyog patilNo ratings yet
- A Survey of Polar Stationary Phases For Hydrophilic Interaction Chromatography and Recent Progress in Understanding Retention and SelectivityDocument2 pagesA Survey of Polar Stationary Phases For Hydrophilic Interaction Chromatography and Recent Progress in Understanding Retention and SelectivitySuyog patilNo ratings yet
- Detection of Choline and Acetylcholine IDocument11 pagesDetection of Choline and Acetylcholine ISuyog patilNo ratings yet
- Atracurium, HPLC SuicideDocument5 pagesAtracurium, HPLC SuicideSuyog patilNo ratings yet
- Nutrition Evaluation Laboratory - Jean Mayer USDA Human Nutrition Research Center On AgingDocument6 pagesNutrition Evaluation Laboratory - Jean Mayer USDA Human Nutrition Research Center On AgingSuyog patilNo ratings yet
- Overview and Intro To LCMS and LCMSMSDocument84 pagesOverview and Intro To LCMS and LCMSMSSuyog patilNo ratings yet
- Dietary Intake and Food Sources of Choline in European PopulationsDocument10 pagesDietary Intake and Food Sources of Choline in European PopulationsSuyog patilNo ratings yet
- Propofol AtracuriumDocument3 pagesPropofol AtracuriumSuyog patilNo ratings yet
- Firearms InconclusiveDocument8 pagesFirearms InconclusiveSuyog patilNo ratings yet
- Phenolic, HPLCDocument7 pagesPhenolic, HPLCSuyog patilNo ratings yet
- Nitrosamines AnalysisDocument8 pagesNitrosamines AnalysisSuyog patilNo ratings yet
- Total NitrosaminesDocument8 pagesTotal NitrosaminesSuyog patilNo ratings yet
- Eleven NitrosaminesDocument9 pagesEleven NitrosaminesSuyog patilNo ratings yet
- Fluorescent Labelling - NitrosaminesDocument9 pagesFluorescent Labelling - NitrosaminesSuyog patilNo ratings yet
- Nitrosamines Sartans AnalysisDocument9 pagesNitrosamines Sartans AnalysisSuyog patilNo ratings yet
- Vitamin AnalysisDocument2 pagesVitamin AnalysisSuyog patilNo ratings yet
- LC MS Based MetabolomicsDocument280 pagesLC MS Based MetabolomicsSuyog patilNo ratings yet
- Polymers For Personal UseDocument316 pagesPolymers For Personal UseSuyog patil100% (3)
- LiquidChromatography MassSpecDocument9 pagesLiquidChromatography MassSpecSuyog patilNo ratings yet
- AnnexureDocument10 pagesAnnexureSuyog patilNo ratings yet
- Anew HPLCmethodforazithromycinquantitationDocument5 pagesAnew HPLCmethodforazithromycinquantitationSuyog patilNo ratings yet
- Folic Acid and FolatesDocument443 pagesFolic Acid and FolatesSuyog patilNo ratings yet
- Analytical Techniques in Forensic Science 2021Document447 pagesAnalytical Techniques in Forensic Science 2021Suyog patilNo ratings yet
- 7.62mm X 39mm - Military CartridgesDocument5 pages7.62mm X 39mm - Military CartridgesSuyog patilNo ratings yet
- Polymers For Personal UseDocument316 pagesPolymers For Personal UseSuyog patil100% (3)
- Quick Reference Guide: Getz - Indd 1 4/10/08 8:21:51 PMDocument20 pagesQuick Reference Guide: Getz - Indd 1 4/10/08 8:21:51 PMSuyog patil100% (1)
- PCMP (Guzman, Renz N. Bped Ep21)Document4 pagesPCMP (Guzman, Renz N. Bped Ep21)Renz N. GuzmanNo ratings yet
- G6RNDocument3 pagesG6RNValeri Luht Eurocargo FinlandNo ratings yet
- GENERAL 5pgDocument5 pagesGENERAL 5pgeee beeNo ratings yet
- SAF Holland Mechanical Suspension KitsDocument4 pagesSAF Holland Mechanical Suspension KitsshenoibrijithmaxNo ratings yet
- Massive Migration From The Steppe SuppleDocument141 pagesMassive Migration From The Steppe SuppleJonNo ratings yet
- Acquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingDocument3 pagesAcquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingAnonymous iZJv305rNo ratings yet
- ERBEJETDocument8 pagesERBEJETHossain TanjilaaNo ratings yet
- Combined Cellulitis - FinalDocument78 pagesCombined Cellulitis - Finalsaru_patel0% (1)
- TVL SHSAnjillyDocument12 pagesTVL SHSAnjillyANJILLY IBRAHIMNo ratings yet
- Human TraffickingDocument26 pagesHuman TraffickingNiyoga Singarimbun100% (3)
- The Employees' Compensation Act, 1923Document23 pagesThe Employees' Compensation Act, 1923Charan Kamal SinghNo ratings yet
- CRU-83 Combat Edge RegulatorDocument1 pageCRU-83 Combat Edge RegulatorfuccioniNo ratings yet
- CEM1008F Applied Solution Chemistry Part 1 2021Document29 pagesCEM1008F Applied Solution Chemistry Part 1 2021Simlindile NgobelaNo ratings yet
- Peugeot 607 Owners Manual 2005Document206 pagesPeugeot 607 Owners Manual 2005AndreiNo ratings yet
- Major Trauma Fellowship Senior Fellow Job Description: VisionDocument10 pagesMajor Trauma Fellowship Senior Fellow Job Description: VisionM LubisNo ratings yet
- CHCCCS015 Assessment Tool V1.4 Nov 2018Document12 pagesCHCCCS015 Assessment Tool V1.4 Nov 2018yESHEy T100% (1)
- P - Chapter 7Document17 pagesP - Chapter 7usa2017lapNo ratings yet
- 2.0 17-02-IM-f (Installation Manual)Document90 pages2.0 17-02-IM-f (Installation Manual)ARMANDOROSAS100% (1)
- Manual 2 PDFDocument442 pagesManual 2 PDFSebastian CoraisacaNo ratings yet
- AssignmentDocument12 pagesAssignmentShubham Jain ModiNo ratings yet
- The Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocDocument43 pagesThe Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocKenberly DingleNo ratings yet
- Calibration of Dosimeters Used in Radiation TherapyDocument122 pagesCalibration of Dosimeters Used in Radiation TherapySOHON SINHA MAHAPATRANo ratings yet
- Raising Permit: Office of The Building OfficialDocument2 pagesRaising Permit: Office of The Building OfficialJc JüsäyänNo ratings yet
- Standard Muster List: NYK SMS Manual (Rev:2020/01/01)Document2 pagesStandard Muster List: NYK SMS Manual (Rev:2020/01/01)Cleanard HidalgoNo ratings yet
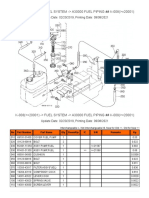
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- String of Pearls Slide ShowDocument23 pagesString of Pearls Slide Showjimhtolbert434No ratings yet
- Review of WAG Field ExperienceDocument10 pagesReview of WAG Field ExperienceJavier E. Guerrero ArrietaNo ratings yet
- Nameplate PDFDocument8 pagesNameplate PDFobida adailehNo ratings yet
- Insurance Loss DigestDocument12 pagesInsurance Loss DigestRyan AcostaNo ratings yet