Download as pdf or txt
You might also like
- NCM 113 Final Module 8 LectureDocument8 pagesNCM 113 Final Module 8 LectureAngel Khrisna BacasmotNo ratings yet
- MODULE 6 HealthDocument6 pagesMODULE 6 Healthtalithaonkabetse723No ratings yet
- What Is Global Health and Why Is It ImportantDocument7 pagesWhat Is Global Health and Why Is It ImportantSanty ManuelNo ratings yet
- Global Health Issues PPDocument91 pagesGlobal Health Issues PPRitaNo ratings yet
- Macroeconomic Instability "Poverty": Gul Rukh Mehboob Asst. Professor Health Economics HEM-MacroeconomicsDocument17 pagesMacroeconomic Instability "Poverty": Gul Rukh Mehboob Asst. Professor Health Economics HEM-MacroeconomicsFiza KarimNo ratings yet
- Health Crisis Brought by The PandemicDocument18 pagesHealth Crisis Brought by The PandemicCamille MoralesNo ratings yet
- Unit 4: Staying Alive READING 1: The Determinants of MortalityDocument1 pageUnit 4: Staying Alive READING 1: The Determinants of MortalityHuynhtrunghieuNo ratings yet
- Health and DevelopmentDocument40 pagesHealth and DevelopmentEbenezer AbrahamNo ratings yet
- 3rd Quarter Module Health 10 4Document7 pages3rd Quarter Module Health 10 4alumnospaul897No ratings yet
- Ii. Problems and Development Strategies: Problems of The Third World CountriesDocument21 pagesIi. Problems and Development Strategies: Problems of The Third World CountriesMicsjadeCastilloNo ratings yet
- Globalisation - Roles, Challenges and Strategies (Adriana and Iman Lg7013a)Document19 pagesGlobalisation - Roles, Challenges and Strategies (Adriana and Iman Lg7013a)Nur NajihahNo ratings yet
- Health Phenomena in 21st CenturyDocument2 pagesHealth Phenomena in 21st CenturyRegina MarshaNo ratings yet
- Day 1aDocument67 pagesDay 1aMinette BucioNo ratings yet
- Global Health Then and NowDocument4 pagesGlobal Health Then and NownameNo ratings yet
- Concepts and Principles of Public Health ProgramsDocument10 pagesConcepts and Principles of Public Health ProgramssdNo ratings yet
- Module 3 Global Health Issues StudentsDocument34 pagesModule 3 Global Health Issues StudentsqutateNo ratings yet
- WK 2Document2 pagesWK 2Ruth Margareth GuintoNo ratings yet
- CHN 1 Module 1Document9 pagesCHN 1 Module 1kcamillebautistaNo ratings yet
- Capstone Research Group 1Document6 pagesCapstone Research Group 1Arkin Zyke DomanaisNo ratings yet
- Community Health Nursing 1 Public Health Nursing in The PhilippinesDocument16 pagesCommunity Health Nursing 1 Public Health Nursing in The PhilippinesFlourence ZafranNo ratings yet
- Food Safety W07Document7 pagesFood Safety W07MelanieNo ratings yet
- Health Problems in IndiaDocument25 pagesHealth Problems in Indiashubham rathod100% (1)
- Global Heath ChallengesDocument1 pageGlobal Heath ChallengesSidNo ratings yet
- Health 10 Q3 Global Health and The Millennium Development GoalsDocument5 pagesHealth 10 Q3 Global Health and The Millennium Development Goalsrenzghidalgo0409No ratings yet
- The Philippine Health Agenda 2016 To 2022Document11 pagesThe Philippine Health Agenda 2016 To 2022Sheryl Alapad100% (3)
- Global Health Issues, Challenges and Trends The Importance of Global HealthDocument10 pagesGlobal Health Issues, Challenges and Trends The Importance of Global HealthIan James P. BranganNo ratings yet
- Mapeh 10 2nd DiscussionDocument20 pagesMapeh 10 2nd DiscussionGeovin Ashley M. SaranzaNo ratings yet
- Presentation 1Document12 pagesPresentation 1Dias ThomasNo ratings yet
- Chapter 1Document21 pagesChapter 1Nikhil ShuklaNo ratings yet
- HIV and Food Security Working WithDocument10 pagesHIV and Food Security Working WithRaymond NjengaNo ratings yet
- Campaign SpeechDocument5 pagesCampaign SpeechAE LLANo ratings yet
- Discuss About Eruption of DiseaseDocument4 pagesDiscuss About Eruption of Diseasepeter andrewNo ratings yet
- Medical SociologyDocument9 pagesMedical SociologyOmaNo ratings yet
- Diseases of PovertyDocument11 pagesDiseases of PovertyArchana BhartiNo ratings yet
- Assignment 2Document3 pagesAssignment 2tapiwa shabanNo ratings yet
- Mapeh (Health) 10 Quiz Lesson1 Week5Document2 pagesMapeh (Health) 10 Quiz Lesson1 Week5Jocel FernandezNo ratings yet
- Lesson 1Document14 pagesLesson 1Czarina Mae Quinones TadeoNo ratings yet
- Contempo ReportDocument3 pagesContempo ReportCuttie Anne GalangNo ratings yet
- Health Economy - 085121Document2 pagesHealth Economy - 085121divinzemtchou33No ratings yet
- Module 1 Overview of Public Health Nursing in The PhilippinesDocument4 pagesModule 1 Overview of Public Health Nursing in The PhilippinesJJ VeranoNo ratings yet
- Hunt JurnalDocument29 pagesHunt JurnalLily NGNo ratings yet
- CovidDocument1 pageCovidDeepanjali DasNo ratings yet
- Millennium Development GoalsDocument22 pagesMillennium Development GoalsJOSH ELORDENo ratings yet
- All For Health Health For All WHO 1717264537Document50 pagesAll For Health Health For All WHO 1717264537MoumitaNo ratings yet
- Module 1 - Overview of Public Health Nursing in The PhilippinesDocument7 pagesModule 1 - Overview of Public Health Nursing in The PhilippinesKatie HolmesNo ratings yet
- Av FinalDocument2 pagesAv FinalDeborah CrystinaNo ratings yet
- Covid-19 and The Right To Thrive ResilienceDocument2 pagesCovid-19 and The Right To Thrive ResilienceMaria Lourdes VelardeNo ratings yet
- Group 10 Global HealthDocument12 pagesGroup 10 Global HealthPearl Alex CandoNo ratings yet
- The Potential Impact of Reducing Global Malnutrition On Poverty Reduction and Economic DevelopmentDocument29 pagesThe Potential Impact of Reducing Global Malnutrition On Poverty Reduction and Economic DevelopmentWulan CerankNo ratings yet
- 6-Global Health and Globalization and Public HealthDocument67 pages6-Global Health and Globalization and Public HealthMoreiyamNo ratings yet
- Rift Valley University Department of Public Health Abichu CampusDocument22 pagesRift Valley University Department of Public Health Abichu CampusKiros Tilahun BentiNo ratings yet
- SWOT of PandemicDocument4 pagesSWOT of PandemicAizeahrhey RayoNo ratings yet
- Global Health Care Challenges and Trends Full Assignment PDFDocument16 pagesGlobal Health Care Challenges and Trends Full Assignment PDFNADISH MANZOORNo ratings yet
- 0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesDocument11 pages0.1 Chapter 1 - Overview of Public Health Nursing in The Philippinesaajeno10No ratings yet
- 0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesDocument11 pages0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesJerreca DasasNo ratings yet
- Grade 10 3RD Quarter Mapeh HealthDocument7 pagesGrade 10 3RD Quarter Mapeh HealthcreqyaqaNo ratings yet
- COVIDDocument2 pagesCOVIDANNooonynmousNo ratings yet
- Child MortalityDocument67 pagesChild MortalityjareckbanasiaNo ratings yet
- Community Health NursingDocument16 pagesCommunity Health Nursingandinur farhamNo ratings yet
- Surviving a Viral Pandemic: Thru the Lens of Naturopathic Medical DoctorFrom EverandSurviving a Viral Pandemic: Thru the Lens of Naturopathic Medical DoctorNo ratings yet
- PBBN 1St Yr Child Health Nursing CBIMNCIDocument29 pagesPBBN 1St Yr Child Health Nursing CBIMNCIcopy smart100% (1)
- Who Afro Draft Guidelines For Integrating Child Survival Interventions Into Routine ImmunizationDocument20 pagesWho Afro Draft Guidelines For Integrating Child Survival Interventions Into Routine ImmunizationtpartapNo ratings yet
- Does Zonal Disparity in Maternal Education Explain The Inequality in Child Health Outcomes Across Nigeria's Six Geopolitical Zones?Document7 pagesDoes Zonal Disparity in Maternal Education Explain The Inequality in Child Health Outcomes Across Nigeria's Six Geopolitical Zones?International Journal of Innovative Science and Research TechnologyNo ratings yet
- VaccinDocument30 pagesVaccinBestari PenyelarasNo ratings yet
- Welcome To Your Guide... To TheDocument54 pagesWelcome To Your Guide... To TheDumitrescu LaurentiuNo ratings yet
- Presentation CbimnciDocument36 pagesPresentation Cbimncikidsamir3.0No ratings yet
- Neurodevelopment, Nutrition, and Inflammation - The Evolving Global Child Health Landscape - Bhutta2017Document13 pagesNeurodevelopment, Nutrition, and Inflammation - The Evolving Global Child Health Landscape - Bhutta2017Ana Carolina TerrazzanNo ratings yet
- Programmes Related To Child Health and WelfareDocument40 pagesProgrammes Related To Child Health and WelfareAleena ShibuNo ratings yet
- United Nations Children's Fund (Unicef) : Antje Von Ungern-SternbergDocument5 pagesUnited Nations Children's Fund (Unicef) : Antje Von Ungern-SternbergSiddharth soniNo ratings yet
- CHN M CompilationDocument46 pagesCHN M CompilationRandolf CabigasNo ratings yet
- Pediatric Procedural Adaptations For Low Resource Settings A CaseDocument321 pagesPediatric Procedural Adaptations For Low Resource Settings A CaseSri PoopaseNo ratings yet
- Okuda-Time Series Analysis of Under-Five MortalityDocument61 pagesOkuda-Time Series Analysis of Under-Five MortalityBoniface Okuda100% (4)
- WHO - The World Health 2005Document243 pagesWHO - The World Health 2005esmoiponja100% (1)
- Vital Health StatisticsDocument71 pagesVital Health Statisticsritikaritika93% (14)
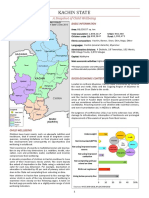
- Kachin State Profile UNICEFDocument4 pagesKachin State Profile UNICEFmarcmyomyint1663100% (1)
- Lesson Plan in Grade 8 Positive NegativeDocument15 pagesLesson Plan in Grade 8 Positive Negativerezamagdaraog.ckc.igsarNo ratings yet
- Analysis of Infant and Child Mortality Trends and Differentials in Kaduna StateDocument194 pagesAnalysis of Infant and Child Mortality Trends and Differentials in Kaduna StateJanice ScatesNo ratings yet
- Harar Health Science CollegeDocument45 pagesHarar Health Science Collegeheysem100% (1)
- Nelson's MCQ'sDocument150 pagesNelson's MCQ'sDrSheika Bawazir93% (40)
- Reproductive Child Health Care Programme: DR Bharat D. ZinjurkeDocument87 pagesReproductive Child Health Care Programme: DR Bharat D. ZinjurkeDr Bharat ZinjurkeNo ratings yet
- Sindhu Final ThesisDocument122 pagesSindhu Final Thesiskrishnasree100% (2)
- A Second Revolution ENGDocument60 pagesA Second Revolution ENGsofiabloemNo ratings yet
- Growth Chart and Care of Under Five ChildrenDocument31 pagesGrowth Chart and Care of Under Five ChildrenWek KivNo ratings yet
- Ethiop Cmyp Latest Revised May 12 2015Document127 pagesEthiop Cmyp Latest Revised May 12 2015abrhamtafere700No ratings yet
- Opportunities For Africa's Newborns: Practical Data, Policy and Programmatic Support For Newborn Care in Africa, November 2006Document250 pagesOpportunities For Africa's Newborns: Practical Data, Policy and Programmatic Support For Newborn Care in Africa, November 2006livelihoodsNo ratings yet
- Joaquim Pinto, Lic - SP, M.M, M.MTSC, DR. Lidia Gomes SKM, MPH, Dr. Avelino Guterres Correia, MPH, Ministry of Health of Timor-LesteDocument7 pagesJoaquim Pinto, Lic - SP, M.M, M.MTSC, DR. Lidia Gomes SKM, MPH, Dr. Avelino Guterres Correia, MPH, Ministry of Health of Timor-LesteInternational Journal of Innovative Science and Research Technology100% (1)
- Child Survival Action Plan - Sierra Leone 2023-2025Document36 pagesChild Survival Action Plan - Sierra Leone 2023-2025Saurav AmanNo ratings yet
- UNICEF 2009 Report (The State of The World's Children)Document168 pagesUNICEF 2009 Report (The State of The World's Children)mwenyeweNo ratings yet
- Infant and Child Mortality: Mothers and Infants, As Well As The Effectiveness ofDocument3 pagesInfant and Child Mortality: Mothers and Infants, As Well As The Effectiveness ofhendraNo ratings yet
- Press Release Piramal Foundation Covid 19 InitiativeDocument2 pagesPress Release Piramal Foundation Covid 19 Initiativeroshni4tufailNo ratings yet