
Check Request Form 32
Check Request Form 32
You might also like
- Ar 600-8-14 - Identification CardsDocument277 pagesAr 600-8-14 - Identification CardsMark CheneyNo ratings yet
- Full Download Community and Public Health Nursing 2nd Edition Harkness Demarco Test Bank PDF Full ChapterDocument36 pagesFull Download Community and Public Health Nursing 2nd Edition Harkness Demarco Test Bank PDF Full Chapterspicymeditate.ujqh2100% (18)
- The Great Train Race: RRR RRRR RDocument6 pagesThe Great Train Race: RRR RRRR RHanaNo ratings yet
- Haynes Full Catalogue 2019Document177 pagesHaynes Full Catalogue 2019LlewellynNo ratings yet
- Renault Wiring DiagramDocument4 pagesRenault Wiring Diagramkamaleon dorado100% (1)
- Basics of Medical Billing & CodingDocument86 pagesBasics of Medical Billing & CodingRic Sánchez100% (3)
- IncytepdfDocument14 pagesIncytepdfnate_raymondNo ratings yet
- Purchase OrderDocument2 pagesPurchase OrderLemuel PetronioNo ratings yet
- Hayes Alex Excel02 ExpendituresDocument4 pagesHayes Alex Excel02 Expendituresapi-665988166No ratings yet
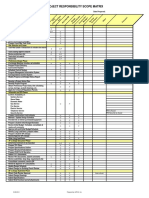
- GTF-COR-21016 Inspection and Test Plan (ITP) Intervention Matrix Rev 0, Jun 2021Document48 pagesGTF-COR-21016 Inspection and Test Plan (ITP) Intervention Matrix Rev 0, Jun 2021Milandro Lou AcuzarNo ratings yet
- PS CH EPA Orion Drinking Water Wastewater Compliance ENDocument8 pagesPS CH EPA Orion Drinking Water Wastewater Compliance ENMaryNo ratings yet
- Business Proposal Title: Business ManagerDocument18 pagesBusiness Proposal Title: Business ManagerJansen Carl UsiNo ratings yet
- Theory of National Income DeterminationDocument50 pagesTheory of National Income DeterminationKunal KunduNo ratings yet
- Co M Pa Rti M en Te Nr. Cu Ren T M Arc A Nu M Ep Ren Um E Fu Ncti A Da Tan Ast Erii Ve CH Im E Nr. Co Pii Sa Lari Ub AzaDocument3 pagesCo M Pa Rti M en Te Nr. Cu Ren T M Arc A Nu M Ep Ren Um E Fu Ncti A Da Tan Ast Erii Ve CH Im E Nr. Co Pii Sa Lari Ub AzaRobert GhitaNo ratings yet
- Freeland Daniel Excel02 ExpendituresDocument4 pagesFreeland Daniel Excel02 Expendituresapi-666431419No ratings yet
- Micropile-One - System-Many-ApplicationsDocument16 pagesMicropile-One - System-Many-Applicationsahmed.naeem66No ratings yet
- Template Quarterly KRADocument5 pagesTemplate Quarterly KRASuba SriramNo ratings yet
- Sugarca Juice Making PlantDocument21 pagesSugarca Juice Making PlantNs3 ProjectsNo ratings yet
- EPA Methods Water Analysis B EPA EN PDFDocument8 pagesEPA Methods Water Analysis B EPA EN PDFDOUGLAS SÁNCHEZNo ratings yet
- Conference Template A4Document4 pagesConference Template A4Frank TangNo ratings yet
- Atherton Jordan Excel02 ExpendituresDocument4 pagesAtherton Jordan Excel02 Expendituresapi-666704587No ratings yet
- Heart Backback Free Pattern Sew Much AdoDocument4 pagesHeart Backback Free Pattern Sew Much Adofateme74.aghNo ratings yet
- Operation ManualDocument42 pagesOperation ManualRadiología e Imagen para EstudiantesNo ratings yet
- Group1 DFD 2Document3 pagesGroup1 DFD 2Tuhin AbdullahNo ratings yet
- Recognizing Expenses When Incurred Rather Than When PaidDocument2 pagesRecognizing Expenses When Incurred Rather Than When PaidNath BongalonNo ratings yet
- Core-Yp: Male Female Client IDDocument1 pageCore-Yp: Male Female Client IDcarla sousa100% (1)
- Lesson No. 7A Evolution of Politics and President 1Document39 pagesLesson No. 7A Evolution of Politics and President 1Mariel ObradoNo ratings yet
- AppealsDocument37 pagesAppealssomya jainNo ratings yet
- Det-Tronics Flame DetectionDocument2 pagesDet-Tronics Flame DetectionGabriel MendezNo ratings yet
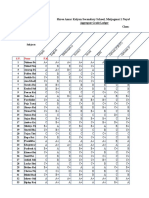
- Co Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDocument4 pagesCo Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDB BhandariNo ratings yet
- Balanced Living WheelDocument1 pageBalanced Living WheeljessicaNo ratings yet
- CD103M Technical Specification: Standard Pump Material SpecificationDocument2 pagesCD103M Technical Specification: Standard Pump Material SpecificationmuahdibNo ratings yet
- Fy13 Service Contract Inventory 12162013Document288 pagesFy13 Service Contract Inventory 12162013German ToledoNo ratings yet
- Route 133 8 22 04 MAPDocument1 pageRoute 133 8 22 04 MAPJason BentleyNo ratings yet
- Menahga School District's 2023-2024 Certified Staff Seniority ListDocument7 pagesMenahga School District's 2023-2024 Certified Staff Seniority ListShannon GeisenNo ratings yet
- MatrixDocument3 pagesMatrixfarhanyazdaniNo ratings yet
- AGi32 v19 Quick ReferenceDocument8 pagesAGi32 v19 Quick ReferenceNalex GeeNo ratings yet
- P-Release and PPAP To Be Secured According IB Deadlines For A Predictable LaunchDocument5 pagesP-Release and PPAP To Be Secured According IB Deadlines For A Predictable LaunchPANDIAN PERIASAMYNo ratings yet
- Comparison of Percentage Weightage of Top Ten Topics in JEE MainDocument1 pageComparison of Percentage Weightage of Top Ten Topics in JEE Mainrineeth22745No ratings yet
- De Rebus September 2018Document48 pagesDe Rebus September 2018ConeliusNo ratings yet
- QM - Monitoring Defect Reject 2020 (Week 2)Document28 pagesQM - Monitoring Defect Reject 2020 (Week 2)NurhadiNo ratings yet
- Resistron: Temperature Controllers For Heatsealing Plastic FilmsDocument2 pagesResistron: Temperature Controllers For Heatsealing Plastic FilmsIulian LupuNo ratings yet
- Routes by Number All - R3Document9 pagesRoutes by Number All - R3Chamin HewaNo ratings yet
- SS 304plates-0.5mm, 1.5mm, 2mm, 3mmDocument1 pageSS 304plates-0.5mm, 1.5mm, 2mm, 3mmvtalexNo ratings yet
- National Standards For Music Education LKDocument1 pageNational Standards For Music Education LKMary Maxwell100% (1)
- Handbook AiAX Coatings EngDocument20 pagesHandbook AiAX Coatings EngfinhasNo ratings yet
- Adesivos Edm 004Document1 pageAdesivos Edm 004montenegrojoaol55No ratings yet
- DineshDocument3 pagesDineshMUNI Raja AkkalaNo ratings yet
- Scroll Air Selection MatrixDocument1 pageScroll Air Selection MatrixStefy CarrascoNo ratings yet
- Smart Champ Insurance Brochure 2017Document12 pagesSmart Champ Insurance Brochure 2017RahulNo ratings yet
- UNESCO WHEUR World Higher Education University Ranking Top 1000 Universities in The WorldDocument87 pagesUNESCO WHEUR World Higher Education University Ranking Top 1000 Universities in The WorldDaniel OdinNo ratings yet
- March Pump Chemical Guide Rev15 2Document9 pagesMarch Pump Chemical Guide Rev15 2Velan ThrumaranNo ratings yet
- Reglamento Nemesis CastellanoDocument24 pagesReglamento Nemesis CastellanoeesbdocumentsNo ratings yet
- PRC IV SutureDocument4 pagesPRC IV SutureFreyjaa MabelinNo ratings yet
- Program Bus PitDocument1 pageProgram Bus PitTudor AlinNo ratings yet
- STRAP Software - Client Projects - Emirates Stadium - Atir EngineeringDocument6 pagesSTRAP Software - Client Projects - Emirates Stadium - Atir EngineeringAreaya mahetemNo ratings yet
- Novum IQ Platform Core Brochure (Includes LVP and SYR) - CCDocument5 pagesNovum IQ Platform Core Brochure (Includes LVP and SYR) - CCsvetlana123197No ratings yet
- Electronicsw 1Document3 pagesElectronicsw 1Princes May MartizanoNo ratings yet
- Pharmacoepidemiology Part 1 Merged CompressedDocument271 pagesPharmacoepidemiology Part 1 Merged CompressedJanella GarciaNo ratings yet
- TG Original Service DimensionsDocument1 pageTG Original Service DimensionsgrantNo ratings yet
- Case Study EdFinancial Services Achieves NIST Compliance For Service AccountsDocument2 pagesCase Study EdFinancial Services Achieves NIST Compliance For Service AccountsRadu CostinNo ratings yet
- Medicare BasicsDocument56 pagesMedicare Basicsapi-239463541No ratings yet
- Bulletin 201015 (HTML Edition)Document110 pagesBulletin 201015 (HTML Edition)Donnie100% (1)
- DD 2527Document2 pagesDD 2527Paul MilesNo ratings yet
- Mountaineer March 2008Document8 pagesMountaineer March 2008Jeremy O'BryanNo ratings yet
- WomeninMilitary PDFDocument10 pagesWomeninMilitary PDFAnksheNo ratings yet
- Newsletter July 2011-Part IDocument28 pagesNewsletter July 2011-Part IMatthew X. HauserNo ratings yet
- Form-Cms1500 - MARGARITA GUTIÉRREZ ALONSODocument2 pagesForm-Cms1500 - MARGARITA GUTIÉRREZ ALONSOAna SotoNo ratings yet
- Frequently Asked Questions Regarding Reserve RetirementDocument4 pagesFrequently Asked Questions Regarding Reserve RetirementKevin HolcombNo ratings yet
- 67 A B C D E F G H: Hospital General AltoDocument2 pages67 A B C D E F G H: Hospital General AltoAlejandra Ramos BaezNo ratings yet
- Plans Vs WalgreensDocument68 pagesPlans Vs WalgreensAnonymous 6f8RIS6No ratings yet
- VP-8 Deployment GuideDocument46 pagesVP-8 Deployment Guideclayw05No ratings yet
- Ar 600-8-7 - Retirement Services ProgramDocument27 pagesAr 600-8-7 - Retirement Services ProgramMark CheneyNo ratings yet
- Bulletin 190315 (HTML Edition)Document148 pagesBulletin 190315 (HTML Edition)DonnieNo ratings yet
- AR Billing Manual - V1212-1Document14 pagesAR Billing Manual - V1212-1spicypoova_899586184100% (1)
- The Healthcare Administrators Desk ReferenceDocument197 pagesThe Healthcare Administrators Desk ReferenceJonathan_Hicks_6507100% (1)
- DODD 6010.04 Healthcare For Uniformed Services Members and BeneficiariesDocument5 pagesDODD 6010.04 Healthcare For Uniformed Services Members and BeneficiariesRobert ValeNo ratings yet
- TRICARE Behavioral Health Care ServicesDocument4 pagesTRICARE Behavioral Health Care ServicesMatthew X. HauserNo ratings yet
- H.R. 4310-Fy13 National Defense Authorization BillDocument595 pagesH.R. 4310-Fy13 National Defense Authorization BillDaveNo ratings yet
- Retiring With V RsDocument36 pagesRetiring With V RsRISHIKESH VAJPAYEENo ratings yet
- Automated Blood Coagulation Analyzer Sysmex CA620Document3 pagesAutomated Blood Coagulation Analyzer Sysmex CA620ОлександрNo ratings yet
- DD 2870 Health Release Form - Scan PDFDocument1 pageDD 2870 Health Release Form - Scan PDFremolacha147No ratings yet
- Galderma Pharmaceutical BrochureDocument1 pageGalderma Pharmaceutical BrochureJamesNo ratings yet
- Access Program CouponDocument1 pageAccess Program CouponipkwokhungNo ratings yet
- Bulletin 190115 (HTML Edition)Document134 pagesBulletin 190115 (HTML Edition)DonnieNo ratings yet
- CLB-451 Newsletter-Nov13Document12 pagesCLB-451 Newsletter-Nov13Kati Toney-FroNo ratings yet
- Change Healthcare Real-Time Payer ListDocument13 pagesChange Healthcare Real-Time Payer ListData hi DataNo ratings yet





















































































Download as doc, pdf, or txt
You might also like
- Ar 600-8-14 - Identification CardsDocument277 pagesAr 600-8-14 - Identification CardsMark CheneyNo ratings yet
- Full Download Community and Public Health Nursing 2nd Edition Harkness Demarco Test Bank PDF Full ChapterDocument36 pagesFull Download Community and Public Health Nursing 2nd Edition Harkness Demarco Test Bank PDF Full Chapterspicymeditate.ujqh2100% (18)
- The Great Train Race: RRR RRRR RDocument6 pagesThe Great Train Race: RRR RRRR RHanaNo ratings yet
- Haynes Full Catalogue 2019Document177 pagesHaynes Full Catalogue 2019LlewellynNo ratings yet
- Renault Wiring DiagramDocument4 pagesRenault Wiring Diagramkamaleon dorado100% (1)
- Basics of Medical Billing & CodingDocument86 pagesBasics of Medical Billing & CodingRic Sánchez100% (3)
- IncytepdfDocument14 pagesIncytepdfnate_raymondNo ratings yet
- Purchase OrderDocument2 pagesPurchase OrderLemuel PetronioNo ratings yet
- Hayes Alex Excel02 ExpendituresDocument4 pagesHayes Alex Excel02 Expendituresapi-665988166No ratings yet
- GTF-COR-21016 Inspection and Test Plan (ITP) Intervention Matrix Rev 0, Jun 2021Document48 pagesGTF-COR-21016 Inspection and Test Plan (ITP) Intervention Matrix Rev 0, Jun 2021Milandro Lou AcuzarNo ratings yet
- PS CH EPA Orion Drinking Water Wastewater Compliance ENDocument8 pagesPS CH EPA Orion Drinking Water Wastewater Compliance ENMaryNo ratings yet
- Business Proposal Title: Business ManagerDocument18 pagesBusiness Proposal Title: Business ManagerJansen Carl UsiNo ratings yet
- Theory of National Income DeterminationDocument50 pagesTheory of National Income DeterminationKunal KunduNo ratings yet
- Co M Pa Rti M en Te Nr. Cu Ren T M Arc A Nu M Ep Ren Um E Fu Ncti A Da Tan Ast Erii Ve CH Im E Nr. Co Pii Sa Lari Ub AzaDocument3 pagesCo M Pa Rti M en Te Nr. Cu Ren T M Arc A Nu M Ep Ren Um E Fu Ncti A Da Tan Ast Erii Ve CH Im E Nr. Co Pii Sa Lari Ub AzaRobert GhitaNo ratings yet
- Freeland Daniel Excel02 ExpendituresDocument4 pagesFreeland Daniel Excel02 Expendituresapi-666431419No ratings yet
- Micropile-One - System-Many-ApplicationsDocument16 pagesMicropile-One - System-Many-Applicationsahmed.naeem66No ratings yet
- Template Quarterly KRADocument5 pagesTemplate Quarterly KRASuba SriramNo ratings yet
- Sugarca Juice Making PlantDocument21 pagesSugarca Juice Making PlantNs3 ProjectsNo ratings yet
- EPA Methods Water Analysis B EPA EN PDFDocument8 pagesEPA Methods Water Analysis B EPA EN PDFDOUGLAS SÁNCHEZNo ratings yet
- Conference Template A4Document4 pagesConference Template A4Frank TangNo ratings yet
- Atherton Jordan Excel02 ExpendituresDocument4 pagesAtherton Jordan Excel02 Expendituresapi-666704587No ratings yet
- Heart Backback Free Pattern Sew Much AdoDocument4 pagesHeart Backback Free Pattern Sew Much Adofateme74.aghNo ratings yet
- Operation ManualDocument42 pagesOperation ManualRadiología e Imagen para EstudiantesNo ratings yet
- Group1 DFD 2Document3 pagesGroup1 DFD 2Tuhin AbdullahNo ratings yet
- Recognizing Expenses When Incurred Rather Than When PaidDocument2 pagesRecognizing Expenses When Incurred Rather Than When PaidNath BongalonNo ratings yet
- Core-Yp: Male Female Client IDDocument1 pageCore-Yp: Male Female Client IDcarla sousa100% (1)
- Lesson No. 7A Evolution of Politics and President 1Document39 pagesLesson No. 7A Evolution of Politics and President 1Mariel ObradoNo ratings yet
- AppealsDocument37 pagesAppealssomya jainNo ratings yet
- Det-Tronics Flame DetectionDocument2 pagesDet-Tronics Flame DetectionGabriel MendezNo ratings yet
- Co Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDocument4 pagesCo Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDB BhandariNo ratings yet
- Balanced Living WheelDocument1 pageBalanced Living WheeljessicaNo ratings yet
- CD103M Technical Specification: Standard Pump Material SpecificationDocument2 pagesCD103M Technical Specification: Standard Pump Material SpecificationmuahdibNo ratings yet
- Fy13 Service Contract Inventory 12162013Document288 pagesFy13 Service Contract Inventory 12162013German ToledoNo ratings yet
- Route 133 8 22 04 MAPDocument1 pageRoute 133 8 22 04 MAPJason BentleyNo ratings yet
- Menahga School District's 2023-2024 Certified Staff Seniority ListDocument7 pagesMenahga School District's 2023-2024 Certified Staff Seniority ListShannon GeisenNo ratings yet
- MatrixDocument3 pagesMatrixfarhanyazdaniNo ratings yet
- AGi32 v19 Quick ReferenceDocument8 pagesAGi32 v19 Quick ReferenceNalex GeeNo ratings yet
- P-Release and PPAP To Be Secured According IB Deadlines For A Predictable LaunchDocument5 pagesP-Release and PPAP To Be Secured According IB Deadlines For A Predictable LaunchPANDIAN PERIASAMYNo ratings yet
- Comparison of Percentage Weightage of Top Ten Topics in JEE MainDocument1 pageComparison of Percentage Weightage of Top Ten Topics in JEE Mainrineeth22745No ratings yet
- De Rebus September 2018Document48 pagesDe Rebus September 2018ConeliusNo ratings yet
- QM - Monitoring Defect Reject 2020 (Week 2)Document28 pagesQM - Monitoring Defect Reject 2020 (Week 2)NurhadiNo ratings yet
- Resistron: Temperature Controllers For Heatsealing Plastic FilmsDocument2 pagesResistron: Temperature Controllers For Heatsealing Plastic FilmsIulian LupuNo ratings yet
- Routes by Number All - R3Document9 pagesRoutes by Number All - R3Chamin HewaNo ratings yet
- SS 304plates-0.5mm, 1.5mm, 2mm, 3mmDocument1 pageSS 304plates-0.5mm, 1.5mm, 2mm, 3mmvtalexNo ratings yet
- National Standards For Music Education LKDocument1 pageNational Standards For Music Education LKMary Maxwell100% (1)
- Handbook AiAX Coatings EngDocument20 pagesHandbook AiAX Coatings EngfinhasNo ratings yet
- Adesivos Edm 004Document1 pageAdesivos Edm 004montenegrojoaol55No ratings yet
- DineshDocument3 pagesDineshMUNI Raja AkkalaNo ratings yet
- Scroll Air Selection MatrixDocument1 pageScroll Air Selection MatrixStefy CarrascoNo ratings yet
- Smart Champ Insurance Brochure 2017Document12 pagesSmart Champ Insurance Brochure 2017RahulNo ratings yet
- UNESCO WHEUR World Higher Education University Ranking Top 1000 Universities in The WorldDocument87 pagesUNESCO WHEUR World Higher Education University Ranking Top 1000 Universities in The WorldDaniel OdinNo ratings yet
- March Pump Chemical Guide Rev15 2Document9 pagesMarch Pump Chemical Guide Rev15 2Velan ThrumaranNo ratings yet
- Reglamento Nemesis CastellanoDocument24 pagesReglamento Nemesis CastellanoeesbdocumentsNo ratings yet
- PRC IV SutureDocument4 pagesPRC IV SutureFreyjaa MabelinNo ratings yet
- Program Bus PitDocument1 pageProgram Bus PitTudor AlinNo ratings yet
- STRAP Software - Client Projects - Emirates Stadium - Atir EngineeringDocument6 pagesSTRAP Software - Client Projects - Emirates Stadium - Atir EngineeringAreaya mahetemNo ratings yet
- Novum IQ Platform Core Brochure (Includes LVP and SYR) - CCDocument5 pagesNovum IQ Platform Core Brochure (Includes LVP and SYR) - CCsvetlana123197No ratings yet
- Electronicsw 1Document3 pagesElectronicsw 1Princes May MartizanoNo ratings yet
- Pharmacoepidemiology Part 1 Merged CompressedDocument271 pagesPharmacoepidemiology Part 1 Merged CompressedJanella GarciaNo ratings yet
- TG Original Service DimensionsDocument1 pageTG Original Service DimensionsgrantNo ratings yet
- Case Study EdFinancial Services Achieves NIST Compliance For Service AccountsDocument2 pagesCase Study EdFinancial Services Achieves NIST Compliance For Service AccountsRadu CostinNo ratings yet
- Medicare BasicsDocument56 pagesMedicare Basicsapi-239463541No ratings yet
- Bulletin 201015 (HTML Edition)Document110 pagesBulletin 201015 (HTML Edition)Donnie100% (1)
- DD 2527Document2 pagesDD 2527Paul MilesNo ratings yet
- Mountaineer March 2008Document8 pagesMountaineer March 2008Jeremy O'BryanNo ratings yet
- WomeninMilitary PDFDocument10 pagesWomeninMilitary PDFAnksheNo ratings yet
- Newsletter July 2011-Part IDocument28 pagesNewsletter July 2011-Part IMatthew X. HauserNo ratings yet
- Form-Cms1500 - MARGARITA GUTIÉRREZ ALONSODocument2 pagesForm-Cms1500 - MARGARITA GUTIÉRREZ ALONSOAna SotoNo ratings yet
- Frequently Asked Questions Regarding Reserve RetirementDocument4 pagesFrequently Asked Questions Regarding Reserve RetirementKevin HolcombNo ratings yet
- 67 A B C D E F G H: Hospital General AltoDocument2 pages67 A B C D E F G H: Hospital General AltoAlejandra Ramos BaezNo ratings yet
- Plans Vs WalgreensDocument68 pagesPlans Vs WalgreensAnonymous 6f8RIS6No ratings yet
- VP-8 Deployment GuideDocument46 pagesVP-8 Deployment Guideclayw05No ratings yet
- Ar 600-8-7 - Retirement Services ProgramDocument27 pagesAr 600-8-7 - Retirement Services ProgramMark CheneyNo ratings yet
- Bulletin 190315 (HTML Edition)Document148 pagesBulletin 190315 (HTML Edition)DonnieNo ratings yet
- AR Billing Manual - V1212-1Document14 pagesAR Billing Manual - V1212-1spicypoova_899586184100% (1)
- The Healthcare Administrators Desk ReferenceDocument197 pagesThe Healthcare Administrators Desk ReferenceJonathan_Hicks_6507100% (1)
- DODD 6010.04 Healthcare For Uniformed Services Members and BeneficiariesDocument5 pagesDODD 6010.04 Healthcare For Uniformed Services Members and BeneficiariesRobert ValeNo ratings yet
- TRICARE Behavioral Health Care ServicesDocument4 pagesTRICARE Behavioral Health Care ServicesMatthew X. HauserNo ratings yet
- H.R. 4310-Fy13 National Defense Authorization BillDocument595 pagesH.R. 4310-Fy13 National Defense Authorization BillDaveNo ratings yet
- Retiring With V RsDocument36 pagesRetiring With V RsRISHIKESH VAJPAYEENo ratings yet
- Automated Blood Coagulation Analyzer Sysmex CA620Document3 pagesAutomated Blood Coagulation Analyzer Sysmex CA620ОлександрNo ratings yet
- DD 2870 Health Release Form - Scan PDFDocument1 pageDD 2870 Health Release Form - Scan PDFremolacha147No ratings yet
- Galderma Pharmaceutical BrochureDocument1 pageGalderma Pharmaceutical BrochureJamesNo ratings yet
- Access Program CouponDocument1 pageAccess Program CouponipkwokhungNo ratings yet
- Bulletin 190115 (HTML Edition)Document134 pagesBulletin 190115 (HTML Edition)DonnieNo ratings yet
- CLB-451 Newsletter-Nov13Document12 pagesCLB-451 Newsletter-Nov13Kati Toney-FroNo ratings yet
- Change Healthcare Real-Time Payer ListDocument13 pagesChange Healthcare Real-Time Payer ListData hi DataNo ratings yet