Download as pdf or txt
You might also like
- Trigger Point Therapy for Myofascial Pain: The Practice of Informed TouchFrom EverandTrigger Point Therapy for Myofascial Pain: The Practice of Informed TouchRating: 4 out of 5 stars4/5 (5)
- Specimen (IAL) QP - Unit 6 Edexcel BiologyDocument14 pagesSpecimen (IAL) QP - Unit 6 Edexcel BiologyFathmath MohamedNo ratings yet
- Progressive Strengthening and Stretching Exercises and Ultrasound For Chronic Lateral EpicondylitisDocument9 pagesProgressive Strengthening and Stretching Exercises and Ultrasound For Chronic Lateral EpicondylitisTomBrambo100% (1)
- Academic Stress and Coping StrategiesDocument11 pagesAcademic Stress and Coping StrategiesParty PeopleNo ratings yet
- Hypothesis RoadmapDocument1 pageHypothesis RoadmapJames Head100% (4)
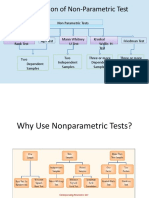
- Nonparametric Tests: Larson/Farber 4th EdDocument94 pagesNonparametric Tests: Larson/Farber 4th EdWasif KhanNo ratings yet
- Schwerla 2020Document8 pagesSchwerla 2020João Paulo Vila Nova GomesNo ratings yet
- ArchRheumatol 33 418Document6 pagesArchRheumatol 33 418qwerty hrNo ratings yet
- Use of The Kinesio Taping Method in Painful Shoulder SyndromeDocument6 pagesUse of The Kinesio Taping Method in Painful Shoulder SyndromeAl BnNo ratings yet
- CE (Ra1) F (SHU) PF1 (PAB) PN (SHU)Document4 pagesCE (Ra1) F (SHU) PF1 (PAB) PN (SHU)Rizky Meilynno CrisvantiknoNo ratings yet
- Mechanical Neckpain Article 1Document8 pagesMechanical Neckpain Article 1Zulaikatu MustaphaNo ratings yet
- PQ Art 37583-10Document7 pagesPQ Art 37583-10Vinay KumarNo ratings yet
- Background:: TH ST THDocument6 pagesBackground:: TH ST THRahayu WindariNo ratings yet
- Pulsed Electromagnetic Field in Patients With Shoulder Impingement SyndromeDocument6 pagesPulsed Electromagnetic Field in Patients With Shoulder Impingement SyndromeHanna RikaswaniNo ratings yet
- Tens 1Document8 pagesTens 1marcelogascon.oNo ratings yet
- Bachelor of PhysiotherapyDocument9 pagesBachelor of Physiotherapyanushka.ganasanNo ratings yet
- To Compare The Effects of Maitland MobilizationDocument4 pagesTo Compare The Effects of Maitland MobilizationravichandragoudaNo ratings yet
- Journal ComparedDocument4 pagesJournal ComparedRisalah Al KhaerNo ratings yet
- International Journal of Physical Medicine & RehabilitationDocument8 pagesInternational Journal of Physical Medicine & RehabilitationfaisalNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchAritha HandricoNo ratings yet
- 3 8 24 398Document6 pages3 8 24 398brain jackNo ratings yet
- Lumbar StabilizationDocument16 pagesLumbar StabilizationSahithya MNo ratings yet
- Sweedish Massage On RADocument69 pagesSweedish Massage On RADr Vaishali MathapatiNo ratings yet
- Ijhrs NeckDocument9 pagesIjhrs Necksulis tiyowatiNo ratings yet
- M W M K C W S e P P S: R C TDocument10 pagesM W M K C W S e P P S: R C TDaniel GuevaraNo ratings yet
- Efficacy of Muscle Energy Technique Versus MyofascialDocument7 pagesEfficacy of Muscle Energy Technique Versus Myofascialmuhammad yaminNo ratings yet
- Artigo - US Pra Dor CrônicaDocument12 pagesArtigo - US Pra Dor CrônicaJose Carlos CamposNo ratings yet
- Ilter 2015Document8 pagesIlter 2015Ahmad Awaludin TaslimNo ratings yet
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiNo ratings yet
- The Effect of Muscle Energy Technique On HeadacheDocument10 pagesThe Effect of Muscle Energy Technique On HeadacheDavid FehertyNo ratings yet
- Chest Physiotherapy After Surgical Treatment of Adolescent Idiopathic ScoliosisDocument2 pagesChest Physiotherapy After Surgical Treatment of Adolescent Idiopathic ScoliosisDaniel GuevaraNo ratings yet
- Tens Us Ic Neck PainDocument5 pagesTens Us Ic Neck PainMahnoor AqeelNo ratings yet
- Article 9Document8 pagesArticle 9umair muqriNo ratings yet
- Estudio 7 - 10.1016@j.clinbDocument9 pagesEstudio 7 - 10.1016@j.clinbOLGUIN HUERTA CRISTIAN RODRIGONo ratings yet
- Pain Motion and Function CompDocument12 pagesPain Motion and Function CompDewi HanaNo ratings yet
- Comparison of Conservative Exercise Therapy With and Without Maitland Thoracic Manipulative Therapy in Patients With Subacromial Pain: Clinical TrialDocument8 pagesComparison of Conservative Exercise Therapy With and Without Maitland Thoracic Manipulative Therapy in Patients With Subacromial Pain: Clinical Trialelchinovichileno420No ratings yet
- Musculoskeletal Science and PracticeDocument11 pagesMusculoskeletal Science and PracticeAnii warikarNo ratings yet
- The Effects of Taping Neuromuscular Compare To Physical Therapies Modalities in Patients With Adhesive Capsulitis of The ShoulderDocument8 pagesThe Effects of Taping Neuromuscular Compare To Physical Therapies Modalities in Patients With Adhesive Capsulitis of The ShouldersilviaNo ratings yet
- 10.1016 - j.jcm.2018.10.001 SMT Effect On GH ROM PDFDocument8 pages10.1016 - j.jcm.2018.10.001 SMT Effect On GH ROM PDFsbachorickNo ratings yet
- Jurnal MassageDocument8 pagesJurnal Massagesaidah arianyNo ratings yet
- Article 8Document4 pagesArticle 8umair muqriNo ratings yet
- I C M M, M O, H P A M T P - F H P: A R C TDocument9 pagesI C M M, M O, H P A M T P - F H P: A R C TAngie D. AndradesNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- Treating Lumbar SpondylosisDocument10 pagesTreating Lumbar SpondylosisDiyya Awaliah Nurhakiimah IbrahimNo ratings yet
- Final PPRDocument24 pagesFinal PPRAman hussainNo ratings yet
- Research Paper 1Document14 pagesResearch Paper 1Ayesha HabibNo ratings yet
- Hipopresivos y Dolor Lumbar Cronico 2021Document9 pagesHipopresivos y Dolor Lumbar Cronico 2021klgarivasNo ratings yet
- EFFECTS OF MOBILIZATION WITH MOVEMENT ON Shoulder PainDocument8 pagesEFFECTS OF MOBILIZATION WITH MOVEMENT ON Shoulder PainDimasPrasetyoNo ratings yet
- Literature Review Paper PTH 662 - PolskiDocument7 pagesLiterature Review Paper PTH 662 - Polskiapi-647278206No ratings yet
- Effectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisDocument8 pagesEffectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of Ultrasound and Extracorporeal Shock Wave Therapy in Lateral EpicondylosisDocument6 pagesComparison of Ultrasound and Extracorporeal Shock Wave Therapy in Lateral EpicondylosisWilliam ChienNo ratings yet
- EJOM-Volume 38-Issue 2 - Page 125-139 TCC - En.ptDocument15 pagesEJOM-Volume 38-Issue 2 - Page 125-139 TCC - En.ptDeby FonsecaNo ratings yet
- A Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyDocument8 pagesA Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyQuiroprácticaParaTodosNo ratings yet
- Fisio 4Document12 pagesFisio 4Daniel Garcia del PinoNo ratings yet
- Conventional Therapy Versus Positional Release Technique in The Treatment of Chronic Low Back DysfunctionDocument7 pagesConventional Therapy Versus Positional Release Technique in The Treatment of Chronic Low Back DysfunctionEmad Eldin Mohamed AbdelatiefNo ratings yet
- Artikel Mahasiswa AkhirDocument5 pagesArtikel Mahasiswa AkhirAfdan Tegar NugrohoNo ratings yet
- Pi Is 000399931300453 XDocument7 pagesPi Is 000399931300453 XFarhaanKhanHaleemNo ratings yet
- 5 Spinal Mobilization Vs Conventional PhysiotherapyDocument11 pages5 Spinal Mobilization Vs Conventional PhysiotherapyEstrella SegniniNo ratings yet
- The Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyDocument8 pagesThe Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyAlexandra-Andreea BroascăNo ratings yet
- 7 Cochrane - UltrasoundGuided Percutaneous Electrolysis andDocument10 pages7 Cochrane - UltrasoundGuided Percutaneous Electrolysis andFranco Suazo MoralesNo ratings yet
- Treatment of Chronic Lower Back Pain With Lumbar Extension and Whole-Body Vibration ExerciseDocument6 pagesTreatment of Chronic Lower Back Pain With Lumbar Extension and Whole-Body Vibration ExerciseSuci NivlaharmyNo ratings yet
- Atlanto-Occipital Joint Manipulation and Suboccipital Inhibition Technique in The Osteopathic Treatment of Patients With Tension-Type HeadacheDocument12 pagesAtlanto-Occipital Joint Manipulation and Suboccipital Inhibition Technique in The Osteopathic Treatment of Patients With Tension-Type HeadacheyoverNo ratings yet
- Cervical StretchingDocument5 pagesCervical StretchingSulthan PhysioNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- DMF Drug Master FileDocument43 pagesDMF Drug Master FileMuhammad AbdullahNo ratings yet
- Pathology Physiology ThaleDocument23 pagesPathology Physiology ThaleMuhammad AbdullahNo ratings yet
- Cup WettingDocument47 pagesCup WettingMuhammad AbdullahNo ratings yet
- Radial Nerve Rehab Program Exercise RecoverDocument2 pagesRadial Nerve Rehab Program Exercise RecoverMuhammad AbdullahNo ratings yet
- Lecture No. 6 Hand X Rays Part 1Document31 pagesLecture No. 6 Hand X Rays Part 1Muhammad AbdullahNo ratings yet
- BillPayReceipt 1696084811655Document1 pageBillPayReceipt 1696084811655Muhammad AbdullahNo ratings yet
- 10 4328acam 6123Document4 pages10 4328acam 6123Muhammad AbdullahNo ratings yet
- Ijerph 18 03267 v2Document15 pagesIjerph 18 03267 v2Muhammad AbdullahNo ratings yet
- Effects of Cervical Stabilisation Exercises On Respiratory Strength in Chronic Neck Pain Patients With Forward Head PostureDocument4 pagesEffects of Cervical Stabilisation Exercises On Respiratory Strength in Chronic Neck Pain Patients With Forward Head PostureMuhammad AbdullahNo ratings yet
- Journal Pone 0273471Document15 pagesJournal Pone 0273471Muhammad AbdullahNo ratings yet
- SSRN Id4093327Document24 pagesSSRN Id4093327Muhammad AbdullahNo ratings yet
- Inspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled TrialDocument8 pagesInspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled TrialMuhammad AbdullahNo ratings yet
- Article JCDRDocument4 pagesArticle JCDRMuhammad AbdullahNo ratings yet
- Complete ThesisDocument127 pagesComplete ThesisAndreia SilvaNo ratings yet
- PaperDocument4 pagesPaperGaurav PatilNo ratings yet
- Kruskal-Wallis Test: Descriptive StatisticsDocument5 pagesKruskal-Wallis Test: Descriptive StatisticsfebriNo ratings yet
- MBA-BS-Recap Session Model Questions-13-07-2023-SV1Document74 pagesMBA-BS-Recap Session Model Questions-13-07-2023-SV1seyon sithamparanathanNo ratings yet
- Nonparametric StatisticsDocument22 pagesNonparametric StatisticsAbhee RajNo ratings yet
- Effectiveness of Therapeutic Community Program Implemented in Batangas City Jail.Document40 pagesEffectiveness of Therapeutic Community Program Implemented in Batangas City Jail.ZSYROLL MATTHEW MENDEZ100% (2)
- Types of Research MethodsDocument18 pagesTypes of Research MethodsYanna Marie Porlucas MacaraegNo ratings yet
- Specimen (IAL) QP - Unit 6 Edexcel BiologyDocument14 pagesSpecimen (IAL) QP - Unit 6 Edexcel BiologyWrikhesh IbtisumNo ratings yet
- Chapter3 Lesson 2 Non - ParametricDocument26 pagesChapter3 Lesson 2 Non - ParametricLAIZA MAE FORRONo ratings yet
- Identification of Herding Behavior, Overconfidence and Risk Tolerance Based On Gender Perspective On Stock Investors in AcehDocument8 pagesIdentification of Herding Behavior, Overconfidence and Risk Tolerance Based On Gender Perspective On Stock Investors in AcehAlvin ZhayyanNo ratings yet
- OBE Syllabus BiostatisticsDocument8 pagesOBE Syllabus BiostatisticsFeona Astoga-BuelaNo ratings yet
- Homework1 StatDocument3 pagesHomework1 StatFahmid TousifNo ratings yet
- (123doc) Quantitative Methods For Second Language Research Carsten Roever Aek Phakiti Routledge 2018 ScanDocument291 pages(123doc) Quantitative Methods For Second Language Research Carsten Roever Aek Phakiti Routledge 2018 ScanYen NhiNo ratings yet
- Final Exam in StatisticsDocument12 pagesFinal Exam in StatisticsJicelle Joy RicaforteNo ratings yet
- Nonparametric Methods: Analysis of Ordinal DataDocument38 pagesNonparametric Methods: Analysis of Ordinal DataRadityaNo ratings yet
- Biostats m6 CIA 1 - Dela Cruz, Jan PhilipDocument2 pagesBiostats m6 CIA 1 - Dela Cruz, Jan PhilipjpdelacrxzNo ratings yet
- Introductory Statistics Using Spss 2nd Edition Ebook PDFDocument61 pagesIntroductory Statistics Using Spss 2nd Edition Ebook PDFjose.waller368100% (54)
- Chapter 6 Non-Parametric and Robust TestDocument43 pagesChapter 6 Non-Parametric and Robust TestgirmaNo ratings yet
- Non-Parametric Techniques: Mann-Whitney Test Wilcoxon Signed Rank TestDocument31 pagesNon-Parametric Techniques: Mann-Whitney Test Wilcoxon Signed Rank TestRahul JajuNo ratings yet
- Donation To Minorities: Is The Upper Class Less Susceptible To Empathetic Charitable Nudge?Document47 pagesDonation To Minorities: Is The Upper Class Less Susceptible To Empathetic Charitable Nudge?jie chenNo ratings yet
- A Study On The Impact of Social Media On Consumer Buying Behaviour of Mobile Phones in ChennaiDocument6 pagesA Study On The Impact of Social Media On Consumer Buying Behaviour of Mobile Phones in ChennaiHeba AliNo ratings yet
- A Study On Welfare Measures On Employee inDocument76 pagesA Study On Welfare Measures On Employee inDhanda Pani GNo ratings yet
- Assessing Entrepreneurial Skills and Awareness Among Learners of Dr. B. R. Ambedkar Open Unviersity.Document18 pagesAssessing Entrepreneurial Skills and Awareness Among Learners of Dr. B. R. Ambedkar Open Unviersity.Priyanka PinkyNo ratings yet
- Nonparametric StatisticsDocument5 pagesNonparametric Statisticsjoseph676No ratings yet
- Cemetery Mapping and Digital Data Analysis: A Case Study in Minnesota, USADocument17 pagesCemetery Mapping and Digital Data Analysis: A Case Study in Minnesota, USAChell AnnNo ratings yet
- Result and Discussion: Figure 1. Respondents' Distribution When Grouped According To Their AgeDocument11 pagesResult and Discussion: Figure 1. Respondents' Distribution When Grouped According To Their AgeMaela Pollen Elumba YemaNo ratings yet