
CC 2021 BMC-MusculoskeletalDisorders 22-364 1-8
CC 2021 BMC-MusculoskeletalDisorders 22-364 1-8
You might also like
- Holistic Health and The Critique of Western Medicine - Janet McKeeDocument3 pagesHolistic Health and The Critique of Western Medicine - Janet McKeeAlex CosiNo ratings yet
- CHLH 575 Community Assessment 1Document3 pagesCHLH 575 Community Assessment 1api-338166341No ratings yet
- Evaluation and Management of Small-Bowel Obstruction: An Eastern Association For The Surgery of Trauma Practice Management GuidelineDocument8 pagesEvaluation and Management of Small-Bowel Obstruction: An Eastern Association For The Surgery of Trauma Practice Management GuidelineAndreia MattiuciNo ratings yet
- 21925682211063854Document14 pages21925682211063854Dr Juan Carlos Ordóñez LegardaNo ratings yet
- Epidemiological Characterization of Tibial Plateau FracturesDocument7 pagesEpidemiological Characterization of Tibial Plateau FracturesArmando RodriguezNo ratings yet
- Iba. Managing Sepsis and Septic Shock in An Endothelial Glycocalyx-Friendly WayDocument12 pagesIba. Managing Sepsis and Septic Shock in An Endothelial Glycocalyx-Friendly WayAna Celia Terreros ChantaNo ratings yet
- 111 PDFDocument8 pages111 PDFMaría José Díaz RojasNo ratings yet
- King ShannonDocument9 pagesKing Shannonarifin hidayatNo ratings yet
- What Is Better For Rotator Cuff Tendinopathy: Dextrose Prolotherapy, Platelet-Rich Plasma, or Corticosteroid Injections? A Randomized Controlled StudyDocument7 pagesWhat Is Better For Rotator Cuff Tendinopathy: Dextrose Prolotherapy, Platelet-Rich Plasma, or Corticosteroid Injections? A Randomized Controlled StudyFreddy ChurataNo ratings yet
- Low Calf Circumference Is Associated With Frailty in Diabetic Adults Aged Over 80 YearsDocument7 pagesLow Calf Circumference Is Associated With Frailty in Diabetic Adults Aged Over 80 YearsJennifer AnguloNo ratings yet
- 28 1561634191Document5 pages28 1561634191Trần Duy TânNo ratings yet
- Adhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyDocument6 pagesAdhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyRuben FigueroaNo ratings yet
- Nagai 2020 Nutrition Status and Functional ProDocument7 pagesNagai 2020 Nutrition Status and Functional ProMiguel de Caso VillarroelNo ratings yet
- The Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForDocument13 pagesThe Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForAntofa V EndeNo ratings yet
- Sternectomy Bota Et AlDocument10 pagesSternectomy Bota Et AlOli BotaNo ratings yet
- Sarcopenic Obesity Is Associated With Frailty Among Community-Dwelling Older Adults: Findings From The WCHAT StudyDocument8 pagesSarcopenic Obesity Is Associated With Frailty Among Community-Dwelling Older Adults: Findings From The WCHAT StudyFlorencia BanicevichNo ratings yet
- 2020 Article 3872Document10 pages2020 Article 3872Gustavo BECERRA PERDOMONo ratings yet
- Low Intensity Whole Body Vs High Intensity Resis - Fragility FXDocument19 pagesLow Intensity Whole Body Vs High Intensity Resis - Fragility FXappiiNo ratings yet
- Polymers 15 01205Document25 pagesPolymers 15 01205ANNE LOUISE FALCAO PASCOALNo ratings yet
- The Rate and Assessment of Muscular Wasting During Critical IllnesDocument26 pagesThe Rate and Assessment of Muscular Wasting During Critical IllnesAdiel OjedaNo ratings yet
- International Wound Journal - 2016 - Li - Vascular Assessment of Wound Healing A Clinical ReviewDocument10 pagesInternational Wound Journal - 2016 - Li - Vascular Assessment of Wound Healing A Clinical Reviewapi-654112138No ratings yet
- The Future of Intensive Care, Microcirculation C. InceDocument13 pagesThe Future of Intensive Care, Microcirculation C. IncemjvaldezNo ratings yet
- Age of Red Cells and Transfusion in Critically IllDocument11 pagesAge of Red Cells and Transfusion in Critically IllTajala .su.17.034No ratings yet
- Vitamin D Supplementation in Systemic Lupus Erythematosus: Relationship To Disease Activity, Fatigue and The Interferon Signature Gene ExpressionDocument8 pagesVitamin D Supplementation in Systemic Lupus Erythematosus: Relationship To Disease Activity, Fatigue and The Interferon Signature Gene ExpressionRengganis Prastami MumpuniNo ratings yet
- Optimizing The Application of Surgery For Degenerative Cervical Myelopathy (AO Spine RECODE-DCM Research Priority Number 10)Document12 pagesOptimizing The Application of Surgery For Degenerative Cervical Myelopathy (AO Spine RECODE-DCM Research Priority Number 10)Dr Juan Carlos Ordóñez LegardaNo ratings yet
- 2022 Article 3254Document8 pages2022 Article 3254Mendoza Vázquez MarcoNo ratings yet
- Journal of Regenerative Medicine & Biology ResearchDocument10 pagesJournal of Regenerative Medicine & Biology ResearchAthenaeum Scientific PublishersNo ratings yet
- 2018 Article 2834Document11 pages2018 Article 2834mitroisergiuNo ratings yet
- Ijerph 19 10510Document15 pagesIjerph 19 10510Victor CristianNo ratings yet
- Nursing Pharmacology 2Document26 pagesNursing Pharmacology 2milkah mwauraNo ratings yet
- The Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForDocument13 pagesThe Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForPatyNo ratings yet
- Int Endodontic J - 2022 - Segura Egea - Impact of Systemic Health On Treatment Outcomes in Endodontics-1Document17 pagesInt Endodontic J - 2022 - Segura Egea - Impact of Systemic Health On Treatment Outcomes in Endodontics-1Nishant ChauhanNo ratings yet
- Jurnal MantapDocument6 pagesJurnal MantapAhmad Fathul AdzmiNo ratings yet
- Orthopaedic Surgery - 2023 - Wang - Comparison of Robot Assisted Percutaneous Cannulated Screws Versus Open Reduction andDocument7 pagesOrthopaedic Surgery - 2023 - Wang - Comparison of Robot Assisted Percutaneous Cannulated Screws Versus Open Reduction andOnSolomonNo ratings yet
- Diagnostics 12 01289Document15 pagesDiagnostics 12 01289Sushmica BaquiranNo ratings yet
- Efficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisChangjing ZhangNo ratings yet
- 2020 Article 3188Document9 pages2020 Article 3188Abril SantiagoNo ratings yet
- 2021 Article 623Document17 pages2021 Article 623Skola paperNo ratings yet
- Randomized Controlled Trial of Vitamin D Supplementation in Older People To Optimize Bone HealthDocument11 pagesRandomized Controlled Trial of Vitamin D Supplementation in Older People To Optimize Bone HealthsmartgalgemscribdNo ratings yet
- 2022 Article 6111Document8 pages2022 Article 6111meriamhfaidh91No ratings yet
- Fracture Healing in Elderly Distal Radius Fracture With Type II Diabetes MellitusDocument7 pagesFracture Healing in Elderly Distal Radius Fracture With Type II Diabetes MellitusAthenaeum Scientific PublishersNo ratings yet
- 2022 Article 5894Document13 pages2022 Article 5894sadaka.mohamedNo ratings yet
- SH 3Document8 pagesSH 3ع الNo ratings yet
- A Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyDocument9 pagesA Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyPIR BanjarmasinNo ratings yet
- 2022 - Pharmaceutics 14, 1644Document22 pages2022 - Pharmaceutics 14, 1644LuisNo ratings yet
- 18 Los Ejercicios de Schroth Mejoran La Calidad de Vida Relacionada Con La SaludDocument8 pages18 Los Ejercicios de Schroth Mejoran La Calidad de Vida Relacionada Con La SaludMike Bukowski MoreidaNo ratings yet
- Ofad 488Document8 pagesOfad 488fahaxa7201No ratings yet
- Doxycline Aneurysmal Bone CystDocument9 pagesDoxycline Aneurysmal Bone CystIskolar MorenoNo ratings yet
- Ijms 22 08855 v2Document22 pagesIjms 22 08855 v2angelNo ratings yet
- Hook Plate With or Without CoracoclavicularDocument6 pagesHook Plate With or Without Coracoclavicularmex487No ratings yet
- Vanco y OsteoDocument22 pagesVanco y OsteoAdrian ReynelNo ratings yet
- Collagen Dressing in The Treatment of Diabetic Foot Ulcer: A Prospective, Randomized, Placebo-Controlled, Single-Center StudyDocument8 pagesCollagen Dressing in The Treatment of Diabetic Foot Ulcer: A Prospective, Randomized, Placebo-Controlled, Single-Center StudylatifaNo ratings yet
- Malignant Bone Tumors - Sparing Vs AmpDocument13 pagesMalignant Bone Tumors - Sparing Vs AmpAnonymous wJTlxhINo ratings yet
- 2023 Complications and Treatment Errors in Peri-Implant Hard Tissue ManagementDocument22 pages2023 Complications and Treatment Errors in Peri-Implant Hard Tissue Managementmatias cofreNo ratings yet
- Platillo Medial + LCP + Angulo PosteroextDocument8 pagesPlatillo Medial + LCP + Angulo PosteroextThiagoNo ratings yet
- Ortodoncia y CirugiaDocument68 pagesOrtodoncia y CirugiaCicse RondanelliNo ratings yet
- Bioengineering 10 00330Document17 pagesBioengineering 10 00330Gabiich AlvaradoNo ratings yet
- Clinical Utility of Integrants FrameItDocument8 pagesClinical Utility of Integrants FrameItAthenaeum Scientific PublishersNo ratings yet
- Microfracture and Microfracture PlusDocument7 pagesMicrofracture and Microfracture PlusdrjorgewtorresNo ratings yet
- s40634 021 00334 1Document6 pagess40634 021 00334 1Saffa AzharaaniNo ratings yet
- Jamasurg E216902 s003Document30 pagesJamasurg E216902 s003Génesis HermidaNo ratings yet
- Wound Healing: Stem Cells Repair and Restorations, Basic and Clinical AspectsFrom EverandWound Healing: Stem Cells Repair and Restorations, Basic and Clinical AspectsNo ratings yet
- ISMOAC - 20241 - Read-OnlyDocument30 pagesISMOAC - 20241 - Read-Onlyaditya galih wicaksonoNo ratings yet
- PR 2021 PlosOne Publ-Online Jan20 1-14Document14 pagesPR 2021 PlosOne Publ-Online Jan20 1-14aditya galih wicaksonoNo ratings yet
- PR 2021 MolecularPsychiatry Publ-Online Nov24 1-11Document11 pagesPR 2021 MolecularPsychiatry Publ-Online Nov24 1-11aditya galih wicaksonoNo ratings yet
- PR 2021 PainPhysician 24 E511-E520Document11 pagesPR 2021 PainPhysician 24 E511-E520aditya galih wicaksonoNo ratings yet
- PR 2021 Internat-J-BasicClinPharmacol 10-1 64-69Document6 pagesPR 2021 Internat-J-BasicClinPharmacol 10-1 64-69aditya galih wicaksonoNo ratings yet
- PR 2021 Healthcare 9-1281 1-12Document12 pagesPR 2021 Healthcare 9-1281 1-12aditya galih wicaksonoNo ratings yet
- PR 2021 Hindawi ID-5559981 CaseReports-in-Medicine 1-4Document4 pagesPR 2021 Hindawi ID-5559981 CaseReports-in-Medicine 1-4aditya galih wicaksonoNo ratings yet
- CC 2021 ACTAS-Dermo-Sifiliográficas 112 199-200Document2 pagesCC 2021 ACTAS-Dermo-Sifiliográficas 112 199-200aditya galih wicaksonoNo ratings yet
- PR 2021 Cureus 13-1-E12870 1-9Document9 pagesPR 2021 Cureus 13-1-E12870 1-9aditya galih wicaksonoNo ratings yet
- Evaluation of Brushing Techniques and Toothbrush Grips Among Rural and Urban ChildrenDocument4 pagesEvaluation of Brushing Techniques and Toothbrush Grips Among Rural and Urban ChildrenSalsabila Farah AzzahraNo ratings yet
- Conrad Research ProposalDocument26 pagesConrad Research Proposalyvette kinyuy100% (1)
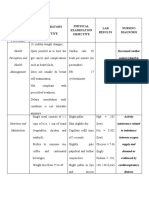
- Gordon'S Functiona L Health Pattern Nursing History Subjective Physical Examination Objective LAB Results Nursing DiagnosisDocument4 pagesGordon'S Functiona L Health Pattern Nursing History Subjective Physical Examination Objective LAB Results Nursing DiagnosischarmaineNo ratings yet
- Flexor Tendon InjuriesDocument12 pagesFlexor Tendon InjuriesFrancis CarterNo ratings yet
- Disposables-and-Consumables GSTDocument64 pagesDisposables-and-Consumables GSTlemmabekeleNo ratings yet
- Water Pollution, Causes and EffectsDocument28 pagesWater Pollution, Causes and EffectsRuchir Gupta67% (3)
- 2023학년도 1학기 대학원 외국인 신입생 모집 요강 (영문)Document22 pages2023학년도 1학기 대학원 외국인 신입생 모집 요강 (영문)Asilbek OrtiqovNo ratings yet
- MIMS Petunjuk Konsultasi - RemovedDocument3 pagesMIMS Petunjuk Konsultasi - RemovedShafaNo ratings yet
- Condon Corkindale 1997Document14 pagesCondon Corkindale 1997Raul Alvarez0% (1)
- Volleyball Training PlanDocument4 pagesVolleyball Training PlanCJ Dayaganon100% (1)
- Resin Bonded Fixed Dental ProsthesisDocument48 pagesResin Bonded Fixed Dental ProsthesismanasviNo ratings yet
- The Effect of Overbite and Overjet On Clinical Par PDFDocument6 pagesThe Effect of Overbite and Overjet On Clinical Par PDFfennilubisNo ratings yet
- Hans India Hyderabad - 25-04-20 PDFDocument10 pagesHans India Hyderabad - 25-04-20 PDFShubham NathNo ratings yet
- Parole AgreementDocument6 pagesParole AgreementKUTV 2News100% (1)
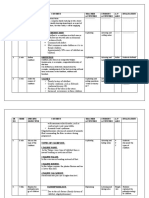
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- Tooth Numbering System: Whydoweneed?Document3 pagesTooth Numbering System: Whydoweneed?najwan domaNo ratings yet
- Budenberg Operation Manual XX SeriesDocument26 pagesBudenberg Operation Manual XX SeriesBram ANo ratings yet
- Newborn Critical Care Center (NCCC) Guidelines: Umbilical Line PlacementDocument5 pagesNewborn Critical Care Center (NCCC) Guidelines: Umbilical Line PlacementMyra BuellaNo ratings yet
- Mapeh7 q1 Melc4 Growthanddeelopment v1Document32 pagesMapeh7 q1 Melc4 Growthanddeelopment v1NICKY SANCHEZNo ratings yet
- MannualonOccupationalHealthSafety WHODocument107 pagesMannualonOccupationalHealthSafety WHOKarthick MNo ratings yet
- Doc-20240119-Wa0001 240120 193556Document3 pagesDoc-20240119-Wa0001 240120 193556madhujeevnaniNo ratings yet
- Usat Premises, Facilities and Educational StandardsDocument31 pagesUsat Premises, Facilities and Educational StandardsUSATPGANo ratings yet
- Application Form Linindo Pacific International (Group of Companies)Document3 pagesApplication Form Linindo Pacific International (Group of Companies)Yehezkiel BayuNo ratings yet
- EC Certificate - Full Quality Assurance System EC Certificate - Full Quality Assurance SystemDocument11 pagesEC Certificate - Full Quality Assurance System EC Certificate - Full Quality Assurance SystemWalid DougaishNo ratings yet
- Pre-Extern Tutorial, 2013Document70 pagesPre-Extern Tutorial, 2013Surat TanprawateNo ratings yet
- 2456.2 EMEA en Hi Fatigue and Optivac Brochure FinalDocument20 pages2456.2 EMEA en Hi Fatigue and Optivac Brochure Finaltran hoanNo ratings yet
- Module 2 Community Organizing - 2140354780 PDFDocument10 pagesModule 2 Community Organizing - 2140354780 PDFAlyssa marieNo ratings yet
- Three Dimensional Imaging in DentistryDocument26 pagesThree Dimensional Imaging in Dentistrydorasani99No ratings yet

































































































Download as pdf or txt
You might also like
- Holistic Health and The Critique of Western Medicine - Janet McKeeDocument3 pagesHolistic Health and The Critique of Western Medicine - Janet McKeeAlex CosiNo ratings yet
- CHLH 575 Community Assessment 1Document3 pagesCHLH 575 Community Assessment 1api-338166341No ratings yet
- Evaluation and Management of Small-Bowel Obstruction: An Eastern Association For The Surgery of Trauma Practice Management GuidelineDocument8 pagesEvaluation and Management of Small-Bowel Obstruction: An Eastern Association For The Surgery of Trauma Practice Management GuidelineAndreia MattiuciNo ratings yet
- 21925682211063854Document14 pages21925682211063854Dr Juan Carlos Ordóñez LegardaNo ratings yet
- Epidemiological Characterization of Tibial Plateau FracturesDocument7 pagesEpidemiological Characterization of Tibial Plateau FracturesArmando RodriguezNo ratings yet
- Iba. Managing Sepsis and Septic Shock in An Endothelial Glycocalyx-Friendly WayDocument12 pagesIba. Managing Sepsis and Septic Shock in An Endothelial Glycocalyx-Friendly WayAna Celia Terreros ChantaNo ratings yet
- 111 PDFDocument8 pages111 PDFMaría José Díaz RojasNo ratings yet
- King ShannonDocument9 pagesKing Shannonarifin hidayatNo ratings yet
- What Is Better For Rotator Cuff Tendinopathy: Dextrose Prolotherapy, Platelet-Rich Plasma, or Corticosteroid Injections? A Randomized Controlled StudyDocument7 pagesWhat Is Better For Rotator Cuff Tendinopathy: Dextrose Prolotherapy, Platelet-Rich Plasma, or Corticosteroid Injections? A Randomized Controlled StudyFreddy ChurataNo ratings yet
- Low Calf Circumference Is Associated With Frailty in Diabetic Adults Aged Over 80 YearsDocument7 pagesLow Calf Circumference Is Associated With Frailty in Diabetic Adults Aged Over 80 YearsJennifer AnguloNo ratings yet
- 28 1561634191Document5 pages28 1561634191Trần Duy TânNo ratings yet
- Adhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyDocument6 pagesAdhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyRuben FigueroaNo ratings yet
- Nagai 2020 Nutrition Status and Functional ProDocument7 pagesNagai 2020 Nutrition Status and Functional ProMiguel de Caso VillarroelNo ratings yet
- The Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForDocument13 pagesThe Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForAntofa V EndeNo ratings yet
- Sternectomy Bota Et AlDocument10 pagesSternectomy Bota Et AlOli BotaNo ratings yet
- Sarcopenic Obesity Is Associated With Frailty Among Community-Dwelling Older Adults: Findings From The WCHAT StudyDocument8 pagesSarcopenic Obesity Is Associated With Frailty Among Community-Dwelling Older Adults: Findings From The WCHAT StudyFlorencia BanicevichNo ratings yet
- 2020 Article 3872Document10 pages2020 Article 3872Gustavo BECERRA PERDOMONo ratings yet
- Low Intensity Whole Body Vs High Intensity Resis - Fragility FXDocument19 pagesLow Intensity Whole Body Vs High Intensity Resis - Fragility FXappiiNo ratings yet
- Polymers 15 01205Document25 pagesPolymers 15 01205ANNE LOUISE FALCAO PASCOALNo ratings yet
- The Rate and Assessment of Muscular Wasting During Critical IllnesDocument26 pagesThe Rate and Assessment of Muscular Wasting During Critical IllnesAdiel OjedaNo ratings yet
- International Wound Journal - 2016 - Li - Vascular Assessment of Wound Healing A Clinical ReviewDocument10 pagesInternational Wound Journal - 2016 - Li - Vascular Assessment of Wound Healing A Clinical Reviewapi-654112138No ratings yet
- The Future of Intensive Care, Microcirculation C. InceDocument13 pagesThe Future of Intensive Care, Microcirculation C. IncemjvaldezNo ratings yet
- Age of Red Cells and Transfusion in Critically IllDocument11 pagesAge of Red Cells and Transfusion in Critically IllTajala .su.17.034No ratings yet
- Vitamin D Supplementation in Systemic Lupus Erythematosus: Relationship To Disease Activity, Fatigue and The Interferon Signature Gene ExpressionDocument8 pagesVitamin D Supplementation in Systemic Lupus Erythematosus: Relationship To Disease Activity, Fatigue and The Interferon Signature Gene ExpressionRengganis Prastami MumpuniNo ratings yet
- Optimizing The Application of Surgery For Degenerative Cervical Myelopathy (AO Spine RECODE-DCM Research Priority Number 10)Document12 pagesOptimizing The Application of Surgery For Degenerative Cervical Myelopathy (AO Spine RECODE-DCM Research Priority Number 10)Dr Juan Carlos Ordóñez LegardaNo ratings yet
- 2022 Article 3254Document8 pages2022 Article 3254Mendoza Vázquez MarcoNo ratings yet
- Journal of Regenerative Medicine & Biology ResearchDocument10 pagesJournal of Regenerative Medicine & Biology ResearchAthenaeum Scientific PublishersNo ratings yet
- 2018 Article 2834Document11 pages2018 Article 2834mitroisergiuNo ratings yet
- Ijerph 19 10510Document15 pagesIjerph 19 10510Victor CristianNo ratings yet
- Nursing Pharmacology 2Document26 pagesNursing Pharmacology 2milkah mwauraNo ratings yet
- The Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForDocument13 pagesThe Journal of Physiology - 2022 - Boytar - Exercise Induced Changes To The Human Gut Microbiota and Implications ForPatyNo ratings yet
- Int Endodontic J - 2022 - Segura Egea - Impact of Systemic Health On Treatment Outcomes in Endodontics-1Document17 pagesInt Endodontic J - 2022 - Segura Egea - Impact of Systemic Health On Treatment Outcomes in Endodontics-1Nishant ChauhanNo ratings yet
- Jurnal MantapDocument6 pagesJurnal MantapAhmad Fathul AdzmiNo ratings yet
- Orthopaedic Surgery - 2023 - Wang - Comparison of Robot Assisted Percutaneous Cannulated Screws Versus Open Reduction andDocument7 pagesOrthopaedic Surgery - 2023 - Wang - Comparison of Robot Assisted Percutaneous Cannulated Screws Versus Open Reduction andOnSolomonNo ratings yet
- Diagnostics 12 01289Document15 pagesDiagnostics 12 01289Sushmica BaquiranNo ratings yet
- Efficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisChangjing ZhangNo ratings yet
- 2020 Article 3188Document9 pages2020 Article 3188Abril SantiagoNo ratings yet
- 2021 Article 623Document17 pages2021 Article 623Skola paperNo ratings yet
- Randomized Controlled Trial of Vitamin D Supplementation in Older People To Optimize Bone HealthDocument11 pagesRandomized Controlled Trial of Vitamin D Supplementation in Older People To Optimize Bone HealthsmartgalgemscribdNo ratings yet
- 2022 Article 6111Document8 pages2022 Article 6111meriamhfaidh91No ratings yet
- Fracture Healing in Elderly Distal Radius Fracture With Type II Diabetes MellitusDocument7 pagesFracture Healing in Elderly Distal Radius Fracture With Type II Diabetes MellitusAthenaeum Scientific PublishersNo ratings yet
- 2022 Article 5894Document13 pages2022 Article 5894sadaka.mohamedNo ratings yet
- SH 3Document8 pagesSH 3ع الNo ratings yet
- A Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyDocument9 pagesA Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyPIR BanjarmasinNo ratings yet
- 2022 - Pharmaceutics 14, 1644Document22 pages2022 - Pharmaceutics 14, 1644LuisNo ratings yet
- 18 Los Ejercicios de Schroth Mejoran La Calidad de Vida Relacionada Con La SaludDocument8 pages18 Los Ejercicios de Schroth Mejoran La Calidad de Vida Relacionada Con La SaludMike Bukowski MoreidaNo ratings yet
- Ofad 488Document8 pagesOfad 488fahaxa7201No ratings yet
- Doxycline Aneurysmal Bone CystDocument9 pagesDoxycline Aneurysmal Bone CystIskolar MorenoNo ratings yet
- Ijms 22 08855 v2Document22 pagesIjms 22 08855 v2angelNo ratings yet
- Hook Plate With or Without CoracoclavicularDocument6 pagesHook Plate With or Without Coracoclavicularmex487No ratings yet
- Vanco y OsteoDocument22 pagesVanco y OsteoAdrian ReynelNo ratings yet
- Collagen Dressing in The Treatment of Diabetic Foot Ulcer: A Prospective, Randomized, Placebo-Controlled, Single-Center StudyDocument8 pagesCollagen Dressing in The Treatment of Diabetic Foot Ulcer: A Prospective, Randomized, Placebo-Controlled, Single-Center StudylatifaNo ratings yet
- Malignant Bone Tumors - Sparing Vs AmpDocument13 pagesMalignant Bone Tumors - Sparing Vs AmpAnonymous wJTlxhINo ratings yet
- 2023 Complications and Treatment Errors in Peri-Implant Hard Tissue ManagementDocument22 pages2023 Complications and Treatment Errors in Peri-Implant Hard Tissue Managementmatias cofreNo ratings yet
- Platillo Medial + LCP + Angulo PosteroextDocument8 pagesPlatillo Medial + LCP + Angulo PosteroextThiagoNo ratings yet
- Ortodoncia y CirugiaDocument68 pagesOrtodoncia y CirugiaCicse RondanelliNo ratings yet
- Bioengineering 10 00330Document17 pagesBioengineering 10 00330Gabiich AlvaradoNo ratings yet
- Clinical Utility of Integrants FrameItDocument8 pagesClinical Utility of Integrants FrameItAthenaeum Scientific PublishersNo ratings yet
- Microfracture and Microfracture PlusDocument7 pagesMicrofracture and Microfracture PlusdrjorgewtorresNo ratings yet
- s40634 021 00334 1Document6 pagess40634 021 00334 1Saffa AzharaaniNo ratings yet
- Jamasurg E216902 s003Document30 pagesJamasurg E216902 s003Génesis HermidaNo ratings yet
- Wound Healing: Stem Cells Repair and Restorations, Basic and Clinical AspectsFrom EverandWound Healing: Stem Cells Repair and Restorations, Basic and Clinical AspectsNo ratings yet
- ISMOAC - 20241 - Read-OnlyDocument30 pagesISMOAC - 20241 - Read-Onlyaditya galih wicaksonoNo ratings yet
- PR 2021 PlosOne Publ-Online Jan20 1-14Document14 pagesPR 2021 PlosOne Publ-Online Jan20 1-14aditya galih wicaksonoNo ratings yet
- PR 2021 MolecularPsychiatry Publ-Online Nov24 1-11Document11 pagesPR 2021 MolecularPsychiatry Publ-Online Nov24 1-11aditya galih wicaksonoNo ratings yet
- PR 2021 PainPhysician 24 E511-E520Document11 pagesPR 2021 PainPhysician 24 E511-E520aditya galih wicaksonoNo ratings yet
- PR 2021 Internat-J-BasicClinPharmacol 10-1 64-69Document6 pagesPR 2021 Internat-J-BasicClinPharmacol 10-1 64-69aditya galih wicaksonoNo ratings yet
- PR 2021 Healthcare 9-1281 1-12Document12 pagesPR 2021 Healthcare 9-1281 1-12aditya galih wicaksonoNo ratings yet
- PR 2021 Hindawi ID-5559981 CaseReports-in-Medicine 1-4Document4 pagesPR 2021 Hindawi ID-5559981 CaseReports-in-Medicine 1-4aditya galih wicaksonoNo ratings yet
- CC 2021 ACTAS-Dermo-Sifiliográficas 112 199-200Document2 pagesCC 2021 ACTAS-Dermo-Sifiliográficas 112 199-200aditya galih wicaksonoNo ratings yet
- PR 2021 Cureus 13-1-E12870 1-9Document9 pagesPR 2021 Cureus 13-1-E12870 1-9aditya galih wicaksonoNo ratings yet
- Evaluation of Brushing Techniques and Toothbrush Grips Among Rural and Urban ChildrenDocument4 pagesEvaluation of Brushing Techniques and Toothbrush Grips Among Rural and Urban ChildrenSalsabila Farah AzzahraNo ratings yet
- Conrad Research ProposalDocument26 pagesConrad Research Proposalyvette kinyuy100% (1)
- Gordon'S Functiona L Health Pattern Nursing History Subjective Physical Examination Objective LAB Results Nursing DiagnosisDocument4 pagesGordon'S Functiona L Health Pattern Nursing History Subjective Physical Examination Objective LAB Results Nursing DiagnosischarmaineNo ratings yet
- Flexor Tendon InjuriesDocument12 pagesFlexor Tendon InjuriesFrancis CarterNo ratings yet
- Disposables-and-Consumables GSTDocument64 pagesDisposables-and-Consumables GSTlemmabekeleNo ratings yet
- Water Pollution, Causes and EffectsDocument28 pagesWater Pollution, Causes and EffectsRuchir Gupta67% (3)
- 2023학년도 1학기 대학원 외국인 신입생 모집 요강 (영문)Document22 pages2023학년도 1학기 대학원 외국인 신입생 모집 요강 (영문)Asilbek OrtiqovNo ratings yet
- MIMS Petunjuk Konsultasi - RemovedDocument3 pagesMIMS Petunjuk Konsultasi - RemovedShafaNo ratings yet
- Condon Corkindale 1997Document14 pagesCondon Corkindale 1997Raul Alvarez0% (1)
- Volleyball Training PlanDocument4 pagesVolleyball Training PlanCJ Dayaganon100% (1)
- Resin Bonded Fixed Dental ProsthesisDocument48 pagesResin Bonded Fixed Dental ProsthesismanasviNo ratings yet
- The Effect of Overbite and Overjet On Clinical Par PDFDocument6 pagesThe Effect of Overbite and Overjet On Clinical Par PDFfennilubisNo ratings yet
- Hans India Hyderabad - 25-04-20 PDFDocument10 pagesHans India Hyderabad - 25-04-20 PDFShubham NathNo ratings yet
- Parole AgreementDocument6 pagesParole AgreementKUTV 2News100% (1)
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- Tooth Numbering System: Whydoweneed?Document3 pagesTooth Numbering System: Whydoweneed?najwan domaNo ratings yet
- Budenberg Operation Manual XX SeriesDocument26 pagesBudenberg Operation Manual XX SeriesBram ANo ratings yet
- Newborn Critical Care Center (NCCC) Guidelines: Umbilical Line PlacementDocument5 pagesNewborn Critical Care Center (NCCC) Guidelines: Umbilical Line PlacementMyra BuellaNo ratings yet
- Mapeh7 q1 Melc4 Growthanddeelopment v1Document32 pagesMapeh7 q1 Melc4 Growthanddeelopment v1NICKY SANCHEZNo ratings yet
- MannualonOccupationalHealthSafety WHODocument107 pagesMannualonOccupationalHealthSafety WHOKarthick MNo ratings yet
- Doc-20240119-Wa0001 240120 193556Document3 pagesDoc-20240119-Wa0001 240120 193556madhujeevnaniNo ratings yet
- Usat Premises, Facilities and Educational StandardsDocument31 pagesUsat Premises, Facilities and Educational StandardsUSATPGANo ratings yet
- Application Form Linindo Pacific International (Group of Companies)Document3 pagesApplication Form Linindo Pacific International (Group of Companies)Yehezkiel BayuNo ratings yet
- EC Certificate - Full Quality Assurance System EC Certificate - Full Quality Assurance SystemDocument11 pagesEC Certificate - Full Quality Assurance System EC Certificate - Full Quality Assurance SystemWalid DougaishNo ratings yet
- Pre-Extern Tutorial, 2013Document70 pagesPre-Extern Tutorial, 2013Surat TanprawateNo ratings yet
- 2456.2 EMEA en Hi Fatigue and Optivac Brochure FinalDocument20 pages2456.2 EMEA en Hi Fatigue and Optivac Brochure Finaltran hoanNo ratings yet
- Module 2 Community Organizing - 2140354780 PDFDocument10 pagesModule 2 Community Organizing - 2140354780 PDFAlyssa marieNo ratings yet
- Three Dimensional Imaging in DentistryDocument26 pagesThree Dimensional Imaging in Dentistrydorasani99No ratings yet