Download as pdf or txt
You might also like
- HESI Blueprint For Psychiatric Health NursingDocument2 pagesHESI Blueprint For Psychiatric Health NursingJenny Vorst40% (5)
- 13 Categories of Exceptionality As Defined by IDEADocument3 pages13 Categories of Exceptionality As Defined by IDEAgelay garaNo ratings yet
- Common Diseases of NewbornDocument162 pagesCommon Diseases of NewbornMichelle ThereseNo ratings yet
- Respiratory Distress in Newborn: Presented By: Dr. Walaa MousaDocument74 pagesRespiratory Distress in Newborn: Presented By: Dr. Walaa MousasalamredNo ratings yet
- 17 Jan - Paediatrics (DR Ashutosh) DAMS DVT 2022Document60 pages17 Jan - Paediatrics (DR Ashutosh) DAMS DVT 2022Lutfi HakimNo ratings yet
- Reproductive PaedDocument150 pagesReproductive PaedThimira WaidyasekaraNo ratings yet
- PPT HMDDocument60 pagesPPT HMDadityaNo ratings yet
- Anaesthetic Management of Paediatric Emergencies Corrected 3Document51 pagesAnaesthetic Management of Paediatric Emergencies Corrected 3oriaboseNo ratings yet
- Resp DistressDocument58 pagesResp Distresskrishna mandalNo ratings yet
- Respiratory Distress in NewbornDocument52 pagesRespiratory Distress in NewbornNadia SalwaniNo ratings yet
- Respiratory Distress in NewbornDocument54 pagesRespiratory Distress in NewbornAgi Azhari SandiniNo ratings yet
- Respiratory Distress SyndromeDocument121 pagesRespiratory Distress Syndromeinno so qtNo ratings yet
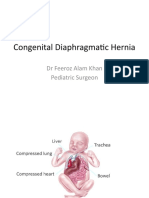
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocument21 pagesCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Respiratory DiseasesDocument58 pagesRespiratory DiseasesSarahNo ratings yet
- Dr. IkhsanDocument46 pagesDr. IkhsanandiendaNo ratings yet
- Neonatal Respiratory Dist.7476158.PowerpointDocument21 pagesNeonatal Respiratory Dist.7476158.PowerpointtyapalupiNo ratings yet
- RESPIRATORY Distress New NewDocument20 pagesRESPIRATORY Distress New NewAdegboye Sherifdeen AdedejiNo ratings yet
- Cor PulmonaleDocument22 pagesCor Pulmonalenatijahtun istiqomahNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- Respiratory Distress in NewbornDocument32 pagesRespiratory Distress in NewbornCharu KalraNo ratings yet
- Respiratory Distress in Newborn FinalDocument22 pagesRespiratory Distress in Newborn FinalajayganeshjNo ratings yet
- Approach To Respiratory Distress in NewbornDocument79 pagesApproach To Respiratory Distress in NewbornNikhil100% (1)
- Neonatal AnaesthesiaDocument61 pagesNeonatal AnaesthesianeneknoraNo ratings yet
- Baker-Acute and Chronic DistressDocument32 pagesBaker-Acute and Chronic DistressLaith AL-GurayfiiNo ratings yet
- RdsDocument26 pagesRdsAsti FiandariNo ratings yet
- Blok 25: Suryadi Susanto Pediatric Departement Krida Wacana Christian UniversityDocument57 pagesBlok 25: Suryadi Susanto Pediatric Departement Krida Wacana Christian UniversityJoseph RivaldoNo ratings yet
- Paed Respiratory DistressDocument45 pagesPaed Respiratory Distressaboje ochekwuNo ratings yet
- Lesson 3.docx SemiDocument7 pagesLesson 3.docx SemiKc-Ann GalaponNo ratings yet
- Pedi 2Document25 pagesPedi 2Roba ANo ratings yet
- PREMATURITYDocument27 pagesPREMATURITYHamizi MD HanapiahNo ratings yet
- Modul Skills KKD4 Reproduksi 2018Document31 pagesModul Skills KKD4 Reproduksi 2018rizkiya novitaNo ratings yet
- Congenital Diaphragmatic Hernia: Pediatric Surgery DepartmentDocument32 pagesCongenital Diaphragmatic Hernia: Pediatric Surgery DepartmentTuan Ahamed CassimNo ratings yet
- Respiratory Distress SyndromeDocument54 pagesRespiratory Distress SyndromeKristine CaringalNo ratings yet
- Acute Conditions of The NeonatesDocument4 pagesAcute Conditions of The NeonatesShermina JalaniNo ratings yet
- Meconium Aspiration SyndromeDocument26 pagesMeconium Aspiration SyndromeJOSLIN100% (2)
- Meconium AspirationDocument23 pagesMeconium AspirationWitneyGraceNo ratings yet
- Gynae EmerganciesDocument39 pagesGynae EmerganciesgibreilNo ratings yet
- CXR - Neonatal Respiratory Distress REVISED DECEMBER 2022Document77 pagesCXR - Neonatal Respiratory Distress REVISED DECEMBER 2022Chua Kai XiangNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- M. Year 4 Peads STudentDocument55 pagesM. Year 4 Peads STudentkamariahsamahNo ratings yet
- Pulmonary Hemorrhage: Dr. Habibur RahimDocument46 pagesPulmonary Hemorrhage: Dr. Habibur Rahimallaaobeid1987No ratings yet
- Pedia Concepts 2:: From Respiratory Problems To HematologicDocument119 pagesPedia Concepts 2:: From Respiratory Problems To HematologicarudarbmeeNo ratings yet
- Persistent Pulmonary Hypertension of The NewbornDocument32 pagesPersistent Pulmonary Hypertension of The NewbornDrSk SamimNo ratings yet
- High Risk NewbornDocument83 pagesHigh Risk Newbornbautil.jameelNo ratings yet
- Respiratory Distress SyndromeDocument30 pagesRespiratory Distress SyndromeDennis MiritiNo ratings yet
- Emergency Obstetrics2Document105 pagesEmergency Obstetrics2Alphine DalgoNo ratings yet
- Rds CaseDocument42 pagesRds Casegebby puspitaNo ratings yet
- RDSDocument34 pagesRDSomarhani517No ratings yet
- Common Congenital Git Malformations FinDocument60 pagesCommon Congenital Git Malformations FinRuth DanielNo ratings yet
- Pediatric NursingDocument105 pagesPediatric NursingPaida P. Abdulmalik75% (4)
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- Pediatric Surgery Dr. A. IgamaDocument6 pagesPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNo ratings yet
- (PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFDocument157 pages(PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFmarcelinaNo ratings yet
- TBL3-Respiratory Distress in Newborn 2Document36 pagesTBL3-Respiratory Distress in Newborn 2HanahigaNo ratings yet
- Review NTS..NCM 109Document11 pagesReview NTS..NCM 109Celline Isabelle ReyesNo ratings yet
- Infantile Respiratory Distress SyndromeDocument27 pagesInfantile Respiratory Distress SyndromeRoy D RogerNo ratings yet
- Birth AsphyxiaDocument12 pagesBirth Asphyxiaannu panchalNo ratings yet
- Extremely LBW PRETERM Case PresentationDocument41 pagesExtremely LBW PRETERM Case PresentationShami PokhrelNo ratings yet
- TandA 9912Document50 pagesTandA 9912Vinod RajNo ratings yet
- Catatonia in Adults - Epidemiology, Clinical Features, Assessment, and Diagnosis - UpToDateDocument21 pagesCatatonia in Adults - Epidemiology, Clinical Features, Assessment, and Diagnosis - UpToDateJéssica ChavesNo ratings yet
- Dizziness: Dizziness Is A Sensation of Imbalance or Faintness, Sometimes Associated With GiddinessDocument3 pagesDizziness: Dizziness Is A Sensation of Imbalance or Faintness, Sometimes Associated With GiddinessAnthony CorporalNo ratings yet
- Aakarshi Rawal Final NTCCDocument11 pagesAakarshi Rawal Final NTCCAakarshi RawalNo ratings yet
- Reviewer For AbPsyc MidtermDocument8 pagesReviewer For AbPsyc MidtermzitrohanzoNo ratings yet
- Management of Traumatic Brain Injury (TBI) - A Clinical Neuroscience-Led Pathway For The NHSDocument8 pagesManagement of Traumatic Brain Injury (TBI) - A Clinical Neuroscience-Led Pathway For The NHS彭金辉 KIVINo ratings yet
- Conduct DisorderDocument3 pagesConduct DisorderakoitsmeNo ratings yet
- Fpsyg 11 587821Document11 pagesFpsyg 11 587821Nurdini MulyaniNo ratings yet
- MFA EXIT EXAM QUESTIONS AND ANSWERS 1.0 Part ADocument5 pagesMFA EXIT EXAM QUESTIONS AND ANSWERS 1.0 Part ADiptendu ParamanickNo ratings yet
- Stroke Hemoragik: Yusi Rizky N 1 6 1 0 2 1 1 0 5 1Document19 pagesStroke Hemoragik: Yusi Rizky N 1 6 1 0 2 1 1 0 5 1Yusi RizkyNo ratings yet
- EngDocument7 pagesEngIkram BenzNo ratings yet
- Golden HourDocument2 pagesGolden Hour5047 Sucharitha.MNo ratings yet
- Sle in PregnancyDocument19 pagesSle in PregnancyShravyaNo ratings yet
- Lesson 1 The Basics of First AidDocument70 pagesLesson 1 The Basics of First AidDJ JoeNo ratings yet
- Baby BluesDocument25 pagesBaby BluesMichael AlexanderNo ratings yet
- Rendam Kaki Dengan Rebusan Jahe Merah Dapat Mencegah Terjadinya EklamsiaDocument8 pagesRendam Kaki Dengan Rebusan Jahe Merah Dapat Mencegah Terjadinya EklamsiaMellwandariskNo ratings yet
- Phenomenology of Obsessive Compulsive Disorder: Review ArticleDocument6 pagesPhenomenology of Obsessive Compulsive Disorder: Review Articlesrikantu s r rajuNo ratings yet
- Class II Neurotic DisordersDocument37 pagesClass II Neurotic DisordersNarayan K Ghorapde100% (1)
- Developmental Language Disorder Leaflet Info For TeachersDocument4 pagesDevelopmental Language Disorder Leaflet Info For TeachersAntonio Vientosur27No ratings yet
- C011171081 - Skripsi DPDocument11 pagesC011171081 - Skripsi DPDinda DeliaNo ratings yet
- Twin-Twin Transfusion Syndrome: Information Leaflet OnDocument8 pagesTwin-Twin Transfusion Syndrome: Information Leaflet Onshona SharupaniNo ratings yet
- Interview QuestionsDocument7 pagesInterview QuestionsMuhammad SaadNo ratings yet
- C2b - Hydatidiform Mole (H-Mole Pregnancy) ContentDocument4 pagesC2b - Hydatidiform Mole (H-Mole Pregnancy) ContentGLADYS MAY GUDELOS MEJIASNo ratings yet
- Anger, Hostility and AggressionDocument15 pagesAnger, Hostility and AggressionJhoe NuevoNo ratings yet
- Hypergraphia: Contributors To Wikimedia ProjectsDocument8 pagesHypergraphia: Contributors To Wikimedia ProjectsCool ArticNo ratings yet
- Reflux Disease (Nerd) Di Rsud Dr. Soetomo SurabayaDocument6 pagesReflux Disease (Nerd) Di Rsud Dr. Soetomo SurabayaFajriNo ratings yet
- Adhd PHD ThesisDocument6 pagesAdhd PHD Thesismelissadaehnmadison100% (2)
- Evidence Based Practice: SHS.423 Saba Nadeem DarDocument31 pagesEvidence Based Practice: SHS.423 Saba Nadeem DarFaheem MustafaNo ratings yet
- Personality Disorder PPT ROA FinalDocument51 pagesPersonality Disorder PPT ROA FinalDat boi50% (4)