Download as docx, pdf, or txt
You might also like
- DocxDocument6 pagesDocxScott Russell McGillivray89% (9)
- Peds Exam 2 Review QuestionsDocument11 pagesPeds Exam 2 Review Questionschristalh7460% (5)
- Pediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument24 pagesPediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUmukhtar abddiNo ratings yet
- Bronchiolitis - Discharge SummaryDocument2 pagesBronchiolitis - Discharge SummaryIndranil SinhaNo ratings yet
- Asthma - Case PresentationDocument56 pagesAsthma - Case Presentationsarooah199467% (6)
- Case StudyDocument14 pagesCase StudyJulia NeriNo ratings yet
- Case Write Up - Dengue FeverDocument22 pagesCase Write Up - Dengue FevervijayaNo ratings yet
- Unit VII - International Health Agencies: Topic: Who & UnicefDocument46 pagesUnit VII - International Health Agencies: Topic: Who & UnicefA J Fathima100% (1)
- QCM Ped PulmoDocument8 pagesQCM Ped PulmoWahbi KhalidNo ratings yet
- Contoh Soal MCQDocument13 pagesContoh Soal MCQrororukmiNo ratings yet
- Work SheetDocument5 pagesWork Sheettefesih tube ተፈስሕ ቲዮብNo ratings yet
- Pulm Board ReviewDocument19 pagesPulm Board ReviewAli LaftaNo ratings yet
- Pediatrics 2Document33 pagesPediatrics 2kyydz7vpdjNo ratings yet
- Case Scenario 1Document3 pagesCase Scenario 1Mafy AlisonNo ratings yet
- Respiratory Conditions (Chapter 15) Flashcards - QuizletDocument4 pagesRespiratory Conditions (Chapter 15) Flashcards - QuizletEmily CallerNo ratings yet
- Lower Respiratory Disorders Case Study AsthmaDocument3 pagesLower Respiratory Disorders Case Study AsthmaElsayed MohamedNo ratings yet
- URTIDocument2 pagesURTIYogeshRavalNo ratings yet
- MCQ Ke-5 2009Document10 pagesMCQ Ke-5 2009WirawanSiregar100% (1)
- Case Study of Pediatric CareDocument4 pagesCase Study of Pediatric CareazafatimatuzzahraNo ratings yet
- Pediatric Respiratory EmergencyDocument35 pagesPediatric Respiratory EmergencyImran FaisalNo ratings yet
- Sas 26Document2 pagesSas 26Gwenn SalazarNo ratings yet
- Pulmonary Medicine - Case StudyDocument9 pagesPulmonary Medicine - Case StudyFerdinand YuzonNo ratings yet
- Imci Test Quest SamplerDocument6 pagesImci Test Quest Samplerjenalyn_ingaran_sanluisNo ratings yet
- General ObjectivesDocument28 pagesGeneral ObjectivesMei MeiNo ratings yet
- DANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateDocument5 pagesDANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateMallory ZaborNo ratings yet
- Bronchiolitis ScriptDocument6 pagesBronchiolitis ScriptAhmed RmelahNo ratings yet
- Case Presentation: Alcover, Llewell T. David, Kyna B. Deunida, Ronecar V. Obida, Arianne A. Tarroja, Cyrille AgnesDocument36 pagesCase Presentation: Alcover, Llewell T. David, Kyna B. Deunida, Ronecar V. Obida, Arianne A. Tarroja, Cyrille AgnesKBDNo ratings yet
- Cases - CoughDocument5 pagesCases - CoughSarthak DubeyNo ratings yet
- Case Study - PneumoniaDocument41 pagesCase Study - PneumoniaCaleb Mcmahon67% (6)
- Case Write UpDocument9 pagesCase Write UpAbdulaziz Al-eisa33% (3)
- Chapter One Assessment of Patient and FamilyDocument49 pagesChapter One Assessment of Patient and FamilyEnoch OseiNo ratings yet
- MicroDocument12 pagesMicroSuman MahmoodNo ratings yet
- Ped Paper CaseDocument9 pagesPed Paper CaseImmah PinedaNo ratings yet
- Respiratory Recalls Printable Version SMADocument26 pagesRespiratory Recalls Printable Version SMAAleksandr ShnyrovNo ratings yet
- Case Study PneumoniaDocument12 pagesCase Study PneumoniaFretzie Mae RamasNo ratings yet
- A Case Study of A Patient W PowerpointDocument37 pagesA Case Study of A Patient W PowerpointMarivic Labartinos BacunganNo ratings yet
- BronchiolitisDocument3 pagesBronchiolitisDelaNo ratings yet
- C. Betadine Compress: Kumpulan Soal MCQ 4 Februari 2022Document21 pagesC. Betadine Compress: Kumpulan Soal MCQ 4 Februari 2022firaNo ratings yet
- AEMT - Obstetrics and Pediatrics Exam PracticeDocument26 pagesAEMT - Obstetrics and Pediatrics Exam PracticeEMS DirectorNo ratings yet
- CasesDocument25 pagesCasesfatemaNo ratings yet
- Pediatric Asthma TBL QuestionsDocument4 pagesPediatric Asthma TBL QuestionsVladimir BasurtoNo ratings yet
- Asthma Case Report FinalDocument6 pagesAsthma Case Report FinalJiaYee GoNo ratings yet
- Pneumonia QuizDocument7 pagesPneumonia QuizJennah JozelleNo ratings yet
- Control of Acute Respiratory Infections 2Document6 pagesControl of Acute Respiratory Infections 2إحسان ماجد محمدNo ratings yet
- Case 1 PcapDocument16 pagesCase 1 PcapJane LaquihonNo ratings yet
- Pediatric Nursing Sample Test QuestionsDocument14 pagesPediatric Nursing Sample Test QuestionsFilipino Nurses Central100% (9)
- A&e Case SummaryDocument1 pageA&e Case SummaryYOS HANANo ratings yet
- AEBADocument6 pagesAEBAAtirah Aa100% (1)
- BetuaDocument3 pagesBetuaSamuelNo ratings yet
- Pneumonia Case StudyDocument5 pagesPneumonia Case StudycrisolandNo ratings yet
- Paediatrics SbaDocument34 pagesPaediatrics SbaAhmad Syahmi YZ100% (1)
- وتين ٦Document29 pagesوتين ٦Mohammad AlrefaiNo ratings yet
- Paeds MCQs Part 1Document34 pagesPaeds MCQs Part 1SsNo ratings yet
- Chest FinalDocument56 pagesChest FinalLwayNo ratings yet
- Cases Resp - SystemDocument12 pagesCases Resp - SystemJerin XavierNo ratings yet
- First 35 QuestionsDocument10 pagesFirst 35 QuestionsDahir Ahmed DahirNo ratings yet
- Kiottoman Pediatric Possibles Md5 @semester 9&10 FireeeDocument107 pagesKiottoman Pediatric Possibles Md5 @semester 9&10 FireeeSatrumin ShirimaNo ratings yet
- Asthma CDDocument3 pagesAsthma CDr.s.a22942No ratings yet
- PediatricsDocument84 pagesPediatricsMoataz TrabehNo ratings yet
- The Asthma and Allergy Action Plan for Kids: A Complete Program to Help Your Child Live a Full and Active LifeFrom EverandThe Asthma and Allergy Action Plan for Kids: A Complete Program to Help Your Child Live a Full and Active LifeNo ratings yet
- Clostridium Difficile InfectionDocument20 pagesClostridium Difficile InfectionTony ZhangNo ratings yet
- Risk Factors For Cutaneous Adverse Drug ReactionsDocument26 pagesRisk Factors For Cutaneous Adverse Drug ReactionsMukesh Kumar SharmaNo ratings yet
- Drug Name Dosage Mechanism of Action Specific Interactions Contraindications and Cautions Adverse Reaction Nursing ConsiderationsDocument4 pagesDrug Name Dosage Mechanism of Action Specific Interactions Contraindications and Cautions Adverse Reaction Nursing ConsiderationsCeelin RoblesNo ratings yet
- Compton M. T. The Union of Religion and Health in Ancient AsklepieiaDocument13 pagesCompton M. T. The Union of Religion and Health in Ancient AsklepieiaLena SkNo ratings yet
- Guidelines For Surgical Treatment of Gastroesophageal Reflux Disease GERDDocument48 pagesGuidelines For Surgical Treatment of Gastroesophageal Reflux Disease GERDMateo TamayoNo ratings yet
- Exam #4 Study Blueprint 2019Document2 pagesExam #4 Study Blueprint 2019Stephanie DeeNo ratings yet
- Dr. Muslim N. Saeed Family & Community Medicine Dept. March 14, 2022Document10 pagesDr. Muslim N. Saeed Family & Community Medicine Dept. March 14, 2022hussain AltaherNo ratings yet
- History Taking SurgeryDocument8 pagesHistory Taking SurgeryKingston HoNo ratings yet
- NCP Pancreatic MassDocument4 pagesNCP Pancreatic MassJan Lianne BernalesNo ratings yet
- Cardiovascular Disorders: Annette HaynesDocument69 pagesCardiovascular Disorders: Annette HaynesBinh Yen Quach TranNo ratings yet
- Question Chapter 6 Cerebellum and Its ConnectionsDocument13 pagesQuestion Chapter 6 Cerebellum and Its ConnectionsTrang BuiNo ratings yet
- OCDE - Health at A Glance 2019 - 4dd50c09-En PDFDocument243 pagesOCDE - Health at A Glance 2019 - 4dd50c09-En PDFJosé Anselmo de Carvalho JúniorNo ratings yet
- Health 6 - Q1 - DW1Document3 pagesHealth 6 - Q1 - DW1Mark Patrics VerderaNo ratings yet
- EnglishDocument5 pagesEnglishMarthe KateNo ratings yet
- Deworming of PetsDocument5 pagesDeworming of PetsRehan Ashraf BandeshaNo ratings yet
- Cataract Surgery - : After The ProcedureDocument16 pagesCataract Surgery - : After The ProcedureAmandeep Singh GandhiNo ratings yet
- Corrosive PoisonsDocument55 pagesCorrosive PoisonsIoana IsarieNo ratings yet
- Tanzania - SOPs For Case Management and Infection Prevention and ControlDocument115 pagesTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- Case Study Copd P. CongestionDocument80 pagesCase Study Copd P. CongestionBryant Riego IIINo ratings yet
- 3 ValvulopatiasDocument31 pages3 ValvulopatiasLeonardoLapasNo ratings yet
- Kode Icd 10Document38 pagesKode Icd 10interna squardNo ratings yet
- Drmercola Judymikovits Covid 19 Vaccination2Document22 pagesDrmercola Judymikovits Covid 19 Vaccination2Didier BarbierNo ratings yet
- NCM 116 Endocrine DisordersDocument106 pagesNCM 116 Endocrine DisordersAnthony Seth AguilandoNo ratings yet
- 10/03/2020 Asbestosis: Dr. A. Sau MBBS, MD (Gold Medalist) DD (Medical) 1Document20 pages10/03/2020 Asbestosis: Dr. A. Sau MBBS, MD (Gold Medalist) DD (Medical) 1puneet100% (1)
- Non Spore Forming Gram Positive Rods: CorynebacteriumDocument6 pagesNon Spore Forming Gram Positive Rods: CorynebacteriumggzgzhhsNo ratings yet
- Script On AssessmentDocument14 pagesScript On AssessmentissaiahnicolleNo ratings yet
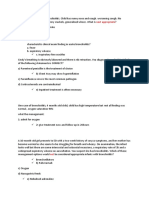
- Sample MCQs (Respiratory)Document12 pagesSample MCQs (Respiratory)Evan O'FlahertyNo ratings yet
- COVID-19 Epidemiology and Response: Group IV OCTOBER 24, 2020Document50 pagesCOVID-19 Epidemiology and Response: Group IV OCTOBER 24, 2020Lemlem ArgawNo ratings yet
- Congenital Anomalies of The KidneyDocument21 pagesCongenital Anomalies of The KidneyRaghu Rajan100% (1)