Download as pdf or txt
You might also like
- Oral Radiology Principles and Interpretation 7th Ed PDFDocument14 pagesOral Radiology Principles and Interpretation 7th Ed PDFLaura Victoria Alvarez RodriguezNo ratings yet
- Nutrition and Physical DegenerationDocument794 pagesNutrition and Physical Degenerationcspathis100% (9)
- Dialogue Physical AssessmentDocument6 pagesDialogue Physical Assessmentsonnya morisaNo ratings yet
- CnsDocument15 pagesCnsArun GeorgeNo ratings yet
- Ameloblastoma PathophysiologyDocument2 pagesAmeloblastoma PathophysiologyKongzter 康明美100% (2)
- Brain SyncDocument46 pagesBrain SyncPriox BangetzNo ratings yet
- Vocabulary of English For NursingDocument37 pagesVocabulary of English For Nursingkelvin BinhNo ratings yet
- SLE: Etiology, Pathogenesis, Clinical Manifestations, and ManagementDocument28 pagesSLE: Etiology, Pathogenesis, Clinical Manifestations, and ManagementRatna AyieNo ratings yet
- Tetanus CaseDocument12 pagesTetanus CasePam RomeroNo ratings yet
- Trigeminal NeuralgiaDocument2 pagesTrigeminal NeuralgiaBryan Lloyd RayatNo ratings yet
- EctrodactylyDocument2 pagesEctrodactylyFrianne LuxNo ratings yet
- Teaching Plan Pain Management HandoutDocument1 pageTeaching Plan Pain Management HandoutCassandraNo ratings yet
- OsteomyelitisDocument10 pagesOsteomyelitismustafaNo ratings yet
- ECG Notes - 1 PDFDocument78 pagesECG Notes - 1 PDFAzizan HannyNo ratings yet
- Juvenile Rheumatoid ArthritisDocument12 pagesJuvenile Rheumatoid ArthritisCatherine PoNo ratings yet
- Vitamin D Deficiency PathwayDocument12 pagesVitamin D Deficiency PathwayJessa MaeNo ratings yet
- Gout Is Usually Characterized by Recurrent Attacks ofDocument15 pagesGout Is Usually Characterized by Recurrent Attacks ofJimmy KusumaNo ratings yet
- Pathophysiology Hypokalemia Periodic ParalysisDocument4 pagesPathophysiology Hypokalemia Periodic Paralysisloyea0% (2)
- Dental Management of Diabetic PatientsDocument30 pagesDental Management of Diabetic PatientsChitrang KolawaleNo ratings yet
- Erosive Lichen Planus of The Oral Cavity: A CaseDocument5 pagesErosive Lichen Planus of The Oral Cavity: A CaseFuad HasanNo ratings yet
- Median Rhomboid GlossitisDocument2 pagesMedian Rhomboid Glossitisdianzalerti9240No ratings yet
- Module D Pain AssessmentDocument12 pagesModule D Pain Assessmentmwhite8051100% (1)
- Case Report Epilepsy (English)Document18 pagesCase Report Epilepsy (English)Ressa OashttamadeaNo ratings yet
- International Journal of Surgery Case Reports: Please State Any Conflicts of InterestDocument3 pagesInternational Journal of Surgery Case Reports: Please State Any Conflicts of InterestGarry WidjajaNo ratings yet
- Acute Appendicitis: Patan Academy of Health SciencesDocument10 pagesAcute Appendicitis: Patan Academy of Health Sciencessuman subediNo ratings yet
- Case Study 1Document34 pagesCase Study 1api-391842100No ratings yet
- Oral MucosaDocument109 pagesOral Mucosashahzeb memonNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- Femoral Fracture ReferatDocument21 pagesFemoral Fracture ReferatAlbertus Johan EdyNo ratings yet
- Lab Diagnosis of Bacillary DysenteryDocument3 pagesLab Diagnosis of Bacillary Dysenterysaket100% (2)
- Trigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, SiddhpurDocument15 pagesTrigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, Siddhpurandreas kevinNo ratings yet
- Preanesthetic Medication JasminaDocument44 pagesPreanesthetic Medication Jasminaanjali s100% (1)
- LCPDDocument7 pagesLCPDakoismeNo ratings yet
- Tetagam 2146469.PA0800 - 009 - 002..000001product Leaflet Approved.141017Document2 pagesTetagam 2146469.PA0800 - 009 - 002..000001product Leaflet Approved.141017abba,drNo ratings yet
- 000 JOURNAL LIST - Free APC - 22 Nov 2020Document12 pages000 JOURNAL LIST - Free APC - 22 Nov 2020kristina dewi100% (1)
- MNT StrokeDocument29 pagesMNT Strokemangalik100% (1)
- Preoperative Assessment in Diabetic PatientsDocument2 pagesPreoperative Assessment in Diabetic PatientsShilpa Pradhan100% (1)
- SiadhDocument16 pagesSiadhGokul Rajan100% (1)
- Pyeloplasty (Anderson-Hynes)Document12 pagesPyeloplasty (Anderson-Hynes)HardiTariqHammaNo ratings yet
- OSCE Scope of The OSCE in The Assessment of ClinicDocument5 pagesOSCE Scope of The OSCE in The Assessment of Clinicdruzair007No ratings yet
- Radicular CystDocument45 pagesRadicular CystPriyanka GanesanNo ratings yet
- Case Report - Deep Vein ThrombosisDocument12 pagesCase Report - Deep Vein ThrombosisAndi Meidin AnugerahNo ratings yet
- Glossitis and Other Tounge Disorder PDFDocument12 pagesGlossitis and Other Tounge Disorder PDFMuhammad Iqbal Al-ayyubiNo ratings yet
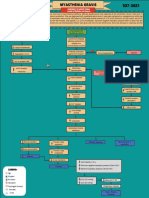
- MYASTHENIA-GRAVIS Concept Map PDFDocument1 pageMYASTHENIA-GRAVIS Concept Map PDFAngelo Dela Cruz VillaromanNo ratings yet
- Prevention of Dental Caries: Name:Huda Khan ROLL #: 753Document33 pagesPrevention of Dental Caries: Name:Huda Khan ROLL #: 753Hudh HudNo ratings yet
- Slide 14 Diseases of Salivary Glands IDocument67 pagesSlide 14 Diseases of Salivary Glands IJustDen09No ratings yet
- Preoperative Skin PreparationDocument16 pagesPreoperative Skin PreparationSyahri DzikriNo ratings yet
- Acute TonsillitisDocument7 pagesAcute TonsillitisMichael HostiadiNo ratings yet
- Patogenesis Pleomorphic AdenomaDocument6 pagesPatogenesis Pleomorphic AdenomaYeni PuspitasariNo ratings yet
- CASE STUDY (Gastro)Document3 pagesCASE STUDY (Gastro)Jake Yvan DizonNo ratings yet
- Intention To Treat AnalysisDocument34 pagesIntention To Treat AnalysisnnshghNo ratings yet
- Otitis ExternaDocument14 pagesOtitis ExternaRizkaGayoNo ratings yet
- Smoking Habits and Alcohol Consumption in Patients Diagnosed With Oral Lichen Planus: A Case ReportDocument17 pagesSmoking Habits and Alcohol Consumption in Patients Diagnosed With Oral Lichen Planus: A Case ReportkuntumNo ratings yet
- NeuroblastomaDocument4 pagesNeuroblastomaGeleine Curutan - OniaNo ratings yet
- Allergic RhinitisDocument22 pagesAllergic RhinitissuciNo ratings yet
- Trichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCDocument27 pagesTrichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCsushma shresthaNo ratings yet
- Stomatitis: Overview of The AnatomyDocument6 pagesStomatitis: Overview of The Anatomyjhing_tajulNo ratings yet
- Dr. Pradeep Daniel Gainneos .R PG Student Dept. of PedodonticsDocument130 pagesDr. Pradeep Daniel Gainneos .R PG Student Dept. of PedodonticsPradeepDanielGainneos0% (1)
- Klasifikasi Kortikosteroid TopikalDocument2 pagesKlasifikasi Kortikosteroid Topikaltaru_airiqu5741No ratings yet
- 2008 Trigeminal NeuralgiaDocument6 pages2008 Trigeminal NeuralgiaApril Rose Airoso - AramburoNo ratings yet
- Wilhour-Nahas2018 Article The NeuralgiasDocument8 pagesWilhour-Nahas2018 Article The NeuralgiasCamilo Benavides BurbanoNo ratings yet
- Acc 61 - Supp2 96Document7 pagesAcc 61 - Supp2 96intermediosamberesNo ratings yet
- Trigeminal Neuralgia and Its Management: Data Supplement ReferencesDocument6 pagesTrigeminal Neuralgia and Its Management: Data Supplement ReferencesfendiNo ratings yet
- MID TERM TEST OF BASIC LEVEL Nurse ClassyDocument5 pagesMID TERM TEST OF BASIC LEVEL Nurse ClassyAmella LaksamanaNo ratings yet
- Chemical Leukoderma To Hair DyeDocument2 pagesChemical Leukoderma To Hair DyeCHONG WEI SHENGNo ratings yet
- Lemon Verbena MonographDocument3 pagesLemon Verbena MonographEmmanuelle Soni-DessaigneNo ratings yet
- BASC-2 Q Global Score Summary SampleDocument11 pagesBASC-2 Q Global Score Summary SamplegenacartaNo ratings yet
- Test Bank For Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Wilburta Billie Q Lindh Carol D Tamparo Barbara M Dahl Julie Morris Cindy CorreaDocument13 pagesTest Bank For Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Wilburta Billie Q Lindh Carol D Tamparo Barbara M Dahl Julie Morris Cindy Correadonnamcbride10021996wqk100% (26)
- Psychedelics As Psychiatric Medications David Nutt Full Chapter PDFDocument69 pagesPsychedelics As Psychiatric Medications David Nutt Full Chapter PDFsagumagivia100% (3)
- Quality Standards For Urban Primary Health CentreDocument284 pagesQuality Standards For Urban Primary Health CentreGajendra TodakarNo ratings yet
- Suicide and Mental Health Problems in Men in PolandDocument6 pagesSuicide and Mental Health Problems in Men in PolandNatalia Alva ZavalaNo ratings yet
- Press Release: JMX International Oncology Cancer Institute Surat, GujaratDocument2 pagesPress Release: JMX International Oncology Cancer Institute Surat, GujaratPankaj Narendrasinh RajNo ratings yet
- Ahss 1170 Term Paper - Allison BakerDocument8 pagesAhss 1170 Term Paper - Allison Bakerapi-300330301No ratings yet
- PresentationDocument19 pagesPresentationSuryansh ThakkerNo ratings yet
- Trauma Triad of DeathDocument5 pagesTrauma Triad of DeathTomNo ratings yet
- Postpartum DepressionDocument1 pagePostpartum DepressionNirmala BhattNo ratings yet
- Comprehensive Review On Endonasal Endoscopic SinusDocument108 pagesComprehensive Review On Endonasal Endoscopic SinusHossam Elden Helmy HaridyNo ratings yet
- NIMH Autism Spectrum DisorderDocument8 pagesNIMH Autism Spectrum DisordertenahernanNo ratings yet
- GHB FactsheetDocument2 pagesGHB FactsheetABC Action NewsNo ratings yet
- PPT Medicine Labels (Attachment 1)Document21 pagesPPT Medicine Labels (Attachment 1)DonnNo ratings yet
- Education of Children With Special Needs in Ethiopia: Analysis of The Rhetoric of Education For All and The Reality On The GroundDocument53 pagesEducation of Children With Special Needs in Ethiopia: Analysis of The Rhetoric of Education For All and The Reality On The GroundSaalih YuunaaNo ratings yet
- Evolution of Prostate BrachytherapyDocument25 pagesEvolution of Prostate BrachytherapyStirNo ratings yet
- Meropenem VenusDocument7 pagesMeropenem VenusChirac OanaNo ratings yet
- COA 016 Audit Checklist For Coal Operation Health and Safety Management Systems PDFDocument43 pagesCOA 016 Audit Checklist For Coal Operation Health and Safety Management Systems PDFMaia FitzgeraldNo ratings yet
- Open University Isced Department of Education Sciences Portuguese Teaching Degree CourseDocument14 pagesOpen University Isced Department of Education Sciences Portuguese Teaching Degree CourseValdemiro NhantumboNo ratings yet
- Nazarita - Concept of Community and Envi HealthDocument37 pagesNazarita - Concept of Community and Envi HealthCess NazaritaNo ratings yet
- The Patient Journey ProjectDocument49 pagesThe Patient Journey ProjectAbhilasha sinhaNo ratings yet
- Different Narratives in Different Doctor Patient RelationshipsDocument20 pagesDifferent Narratives in Different Doctor Patient RelationshipsvishalatthaparNo ratings yet
- Well Prolong Long Started Subjects Find Extent: Set/groupDocument7 pagesWell Prolong Long Started Subjects Find Extent: Set/groupJohnny JohnnieeNo ratings yet
- AssignmentDocument2 pagesAssignmenttayyabauzairNo ratings yet