
3 IschemicHeartDiseases
3 IschemicHeartDiseases
You might also like
- Cusack Protocol .. Supplement Dosages Information Chart. Word PDFDocument2 pagesCusack Protocol .. Supplement Dosages Information Chart. Word PDFNaomy DC100% (6)
- Non-Communicable DiseaseDocument30 pagesNon-Communicable DiseaseLynds Nrsc100% (1)
- GRADE VI Science Baseline TestDocument4 pagesGRADE VI Science Baseline TestanthfranzNo ratings yet
- 6 B&B CirrhosisDocument30 pages6 B&B CirrhosisSara Joseph100% (1)
- CH10Document17 pagesCH10Kim BasicNo ratings yet
- 97Document79 pages97HATLERNo ratings yet
- Psy101: Psychiatric Foundations and Psychological Reaction To DisabilityDocument30 pagesPsy101: Psychiatric Foundations and Psychological Reaction To DisabilityAlexia Ofel DinsonNo ratings yet
- Respiratory Osce: AMSA Edinburgh X IMU Y4Document34 pagesRespiratory Osce: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Acute Tubular NecrosisDocument60 pagesAcute Tubular NecrosisYedesney C. LinaresNo ratings yet
- Pathoma 2087m (34h47) : 1) Growth Adaptations, Cell Injury 154 MinsDocument11 pagesPathoma 2087m (34h47) : 1) Growth Adaptations, Cell Injury 154 Minsgreen mateNo ratings yet
- Structural Biology of HIVDocument31 pagesStructural Biology of HIVLaura TapiaNo ratings yet
- Anastomosis Left Anterior Cerebral Artery BlockageDocument5 pagesAnastomosis Left Anterior Cerebral Artery BlockagemcwnotesNo ratings yet
- Chapter 3 Genetic VariationDocument21 pagesChapter 3 Genetic VariationAbdulkarimNo ratings yet
- Brainstem NucleiDocument9 pagesBrainstem Nucleiankur_1No ratings yet
- Cerebral Blood FlowDocument39 pagesCerebral Blood FlowRajat ThakurNo ratings yet
- CerebellumDocument14 pagesCerebellumapi-508474347No ratings yet
- Cardio Block 3Document62 pagesCardio Block 3Maya LaPradeNo ratings yet
- Nose & Paranasal Sinuses 2018Document63 pagesNose & Paranasal Sinuses 2018yasrul izadNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Schematic Diagram Wilson'S DiseaseDocument2 pagesSchematic Diagram Wilson'S DiseaseAmira CharmaineNo ratings yet
- Brainstem StrokesDocument4 pagesBrainstem StrokesChandniNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
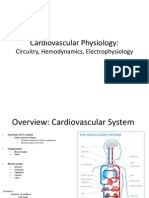
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 pagesCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3No ratings yet
- Edema Pathology by Asif AliDocument21 pagesEdema Pathology by Asif AliHassan AsifNo ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- Anat 6.3 GSA Appendix - EsguerraDocument4 pagesAnat 6.3 GSA Appendix - Esguerralovelots1234No ratings yet
- Pharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraDocument39 pagesPharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraKim Nicole Villaflores0% (1)
- Upperlimb-Clinical CasesDocument18 pagesUpperlimb-Clinical CasesKambwe ChristopherNo ratings yet
- Disease Signs and Symptoms Deficiency/Problem Notes AmyloidosisDocument14 pagesDisease Signs and Symptoms Deficiency/Problem Notes AmyloidosisSriKavya DevineniNo ratings yet
- Genetic and Metabolic DisordersDocument16 pagesGenetic and Metabolic DisordersErin HillNo ratings yet
- IKD9 - Radiological Evaluation of Renal CystsDocument26 pagesIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNo ratings yet
- Cytogenetics Course PackDocument29 pagesCytogenetics Course Packanonymous squashNo ratings yet
- Block 1 Board Review - Lecture NotesDocument127 pagesBlock 1 Board Review - Lecture NotesCece RereNo ratings yet
- Axis DeviationDocument26 pagesAxis DeviationDanial HassanNo ratings yet
- Para Compre 2Document17 pagesPara Compre 2serainie maiNo ratings yet
- Normal Body FloraDocument1 pageNormal Body FloraJulia IshakNo ratings yet
- University of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyDocument7 pagesUniversity of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyWynlor AbarcaNo ratings yet
- Microscopic Morphology Myocardial InfarctionDocument10 pagesMicroscopic Morphology Myocardial InfarctionnathanielNo ratings yet
- Diseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapDocument15 pagesDiseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapJayesh MahajanNo ratings yet
- Virology NotesDocument81 pagesVirology NotesraulNo ratings yet
- Cell and Embryology: Ii. Tissue Slide PreparationDocument9 pagesCell and Embryology: Ii. Tissue Slide Preparationashley nicholeNo ratings yet
- Acute Leukaemias: DR Nilukshi Perera Consultant HaematologistDocument60 pagesAcute Leukaemias: DR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhite100% (2)
- Kidney TumorsDocument15 pagesKidney TumorsJose SirittNo ratings yet
- Sedimen UrinDocument73 pagesSedimen UrinHerbanu PramonoNo ratings yet
- Examination of The HipDocument33 pagesExamination of The HipTumbal BroNo ratings yet
- AB-M02-CH2.2-LIVER PATH-Diffuse & Metabolic Disease-1Document26 pagesAB-M02-CH2.2-LIVER PATH-Diffuse & Metabolic Disease-1Thomas AndersonNo ratings yet
- The Hematology SectionDocument4 pagesThe Hematology SectionVENUS LIRIA PANTINo ratings yet
- Hema Lec Prefinals ExamDocument18 pagesHema Lec Prefinals ExamMark jay LlanoNo ratings yet
- 300 FCPS MCQS Solved 2Document14 pages300 FCPS MCQS Solved 2AS IFNo ratings yet
- Microscopic ExaminationDocument9 pagesMicroscopic ExaminationMariella DingleNo ratings yet
- Nerve StructureDocument53 pagesNerve StructureMedulla Oblongata100% (1)
- Renal Annotated First Aid 2019Document38 pagesRenal Annotated First Aid 2019Heran TeferiNo ratings yet
- Staphylococcus Streptococcus: Propertie S Morpholo Gy Culture & Biochemi Cal ReactionsDocument3 pagesStaphylococcus Streptococcus: Propertie S Morpholo Gy Culture & Biochemi Cal ReactionsmadhuNo ratings yet
- Flow Cytometry: An Introduction and Application To Cytology: December 2018Document12 pagesFlow Cytometry: An Introduction and Application To Cytology: December 2018ABHINABA GUPTANo ratings yet
- Chronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminDocument24 pagesChronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminMJ Putra100% (1)
- CHAPTER ONE To THREEDocument84 pagesCHAPTER ONE To THREEMonju GraceNo ratings yet
- Ischemic Heart DiseaseDocument4 pagesIschemic Heart DiseaseBanana CakeNo ratings yet
- SLE Pathogenesis, Clinical FeaturesDocument30 pagesSLE Pathogenesis, Clinical FeaturesJuwita PratiwiNo ratings yet
- Benign WBC Disorders Third YaerDocument27 pagesBenign WBC Disorders Third YaerAisho KeyfNo ratings yet
- Beri Beri: Water-Soluble Vitamins ThiamineDocument3 pagesBeri Beri: Water-Soluble Vitamins ThiamineLyan SamsonNo ratings yet
- Gluteal Region, Back of The Thigh and Popliteal Fossa.Document81 pagesGluteal Region, Back of The Thigh and Popliteal Fossa.Cupid MohNo ratings yet
- Ischemic Heart Disease (IHD)Document35 pagesIschemic Heart Disease (IHD)Ali Akand AsifNo ratings yet
- Coronary Artery DisaeseDocument48 pagesCoronary Artery DisaeseAzkaZulfiqarNo ratings yet
- MigraineDocument24 pagesMigraineHarsha MaheshwariNo ratings yet
- General Anesthetic 2016Document33 pagesGeneral Anesthetic 2016Harsha MaheshwariNo ratings yet
- LUNGS GuessDocument2 pagesLUNGS GuessHarsha MaheshwariNo ratings yet
- Community Medicine-1Document9 pagesCommunity Medicine-1Harsha MaheshwariNo ratings yet
- Epilepsy2018Document41 pagesEpilepsy2018Harsha MaheshwariNo ratings yet
- 4 5958464350862706598Document8 pages4 5958464350862706598Harsha MaheshwariNo ratings yet
- Cyanide Poisoning SlidesDocument22 pagesCyanide Poisoning SlidesHarsha MaheshwariNo ratings yet
- Overview of LymphomasDocument44 pagesOverview of LymphomasHarsha MaheshwariNo ratings yet
- Gastrulationin MammalsDocument16 pagesGastrulationin MammalsHarsha MaheshwariNo ratings yet
- Stroke Volume, Work, Cardiac Output, Ficks Principal, Laplace Law, Preload CVS by TKJDocument13 pagesStroke Volume, Work, Cardiac Output, Ficks Principal, Laplace Law, Preload CVS by TKJHarsha MaheshwariNo ratings yet
- Faiq AhmedDocument76 pagesFaiq AhmedHarsha MaheshwariNo ratings yet
- Respo-1 MBBS'26Document48 pagesRespo-1 MBBS'26Harsha MaheshwariNo ratings yet
- CHAPTER-04 (TESTt-01)Document10 pagesCHAPTER-04 (TESTt-01)Harsha MaheshwariNo ratings yet
- Physics Points-Chapter-4Document7 pagesPhysics Points-Chapter-4Harsha MaheshwariNo ratings yet
- 1 GluconeogenesisDocument7 pages1 GluconeogenesisHarsha MaheshwariNo ratings yet
- Loco - Respo TEHSEENDocument9 pagesLoco - Respo TEHSEENHarsha MaheshwariNo ratings yet
- Blood Vessels L2Document40 pagesBlood Vessels L2tas xoNo ratings yet
- Test About Circulatory SystemDocument5 pagesTest About Circulatory SystemThảo VânNo ratings yet
- Cardiac ImagingDocument118 pagesCardiac ImagingSay DieukayNo ratings yet
- Jurnal Kulit VaskulitisDocument7 pagesJurnal Kulit VaskulitisSMA N 1 TOROHNo ratings yet
- BFO-Review of Pathology AFODocument32 pagesBFO-Review of Pathology AFOnovitaNo ratings yet
- Life Sciences Grade 10 Learner Support Document MAFUMANI SECONDARYDocument40 pagesLife Sciences Grade 10 Learner Support Document MAFUMANI SECONDARYdeveloping habit and lifestyle of praise and worshNo ratings yet
- RLE FUNDA Test CompilationDocument25 pagesRLE FUNDA Test CompilationAngelika VeluzNo ratings yet
- Burns: Pathophysiology Types Degree PercentageDocument19 pagesBurns: Pathophysiology Types Degree PercentageanuzNo ratings yet
- Sample Book: Vasodilator DrugsDocument4 pagesSample Book: Vasodilator DrugsManangioma ManNo ratings yet
- General Biology II q4 Week 2Document26 pagesGeneral Biology II q4 Week 2Educhamp Learning CenterNo ratings yet
- Lesson 4: Homeostasis and Cells:: The Cell As An OrganismDocument6 pagesLesson 4: Homeostasis and Cells:: The Cell As An Organismrakan ilyasNo ratings yet
- Medical TerminologiesDocument14 pagesMedical TerminologiesShannine Del Rosario BeridaNo ratings yet
- Lesson 4 Blood VesselsDocument14 pagesLesson 4 Blood VesselsCarolyn D MayugaNo ratings yet
- Dar 1997Document3 pagesDar 1997Sarly FebrianaNo ratings yet
- 27 GuytonDocument6 pages27 GuytonBianca Louise Chan LimNo ratings yet
- Mercury Mercruiser Marine Engine 32-4-3l Mpi Gasoline Service ManualDocument22 pagesMercury Mercruiser Marine Engine 32-4-3l Mpi Gasoline Service Manualjamesmiller060901qms100% (33)
- Avascular Necrosis - Causes, Symptoms, Prevention & TreatmentDocument26 pagesAvascular Necrosis - Causes, Symptoms, Prevention & TreatmentSatrio Bangun NegoroNo ratings yet
- Digestive Tract Detoxification GI Health Depends PDFDocument20 pagesDigestive Tract Detoxification GI Health Depends PDFPablo CrespoNo ratings yet
- Inflammation: Cardinal Signs of InflammationDocument9 pagesInflammation: Cardinal Signs of InflammationGeoffreyNo ratings yet
- 6 Seeds To Heaven PDFDocument37 pages6 Seeds To Heaven PDFSarbu Stacy100% (1)
- 7.1 Petermann PCLACDocument11 pages7.1 Petermann PCLACbob marley100% (1)
- Respiration and Transportation WorksheetDocument4 pagesRespiration and Transportation WorksheetAarjav JainNo ratings yet
- NCA - CVA InfarctDocument126 pagesNCA - CVA InfarctRosaree Mae PantojaNo ratings yet
- Fish OilsDocument36 pagesFish OilsGabiNo ratings yet
- Chapter 6. The Circulatory System: Short QuestionsDocument31 pagesChapter 6. The Circulatory System: Short QuestionsParardha DharNo ratings yet
- Arterial UlcersDocument8 pagesArterial Ulcerspka25No ratings yet
- Aging Changes in The Heart and Blood VesselsDocument4 pagesAging Changes in The Heart and Blood VesselsTotalenesya Reforrent SutiknoNo ratings yet





































































































Download as pdf or txt
You might also like
- Cusack Protocol .. Supplement Dosages Information Chart. Word PDFDocument2 pagesCusack Protocol .. Supplement Dosages Information Chart. Word PDFNaomy DC100% (6)
- Non-Communicable DiseaseDocument30 pagesNon-Communicable DiseaseLynds Nrsc100% (1)
- GRADE VI Science Baseline TestDocument4 pagesGRADE VI Science Baseline TestanthfranzNo ratings yet
- 6 B&B CirrhosisDocument30 pages6 B&B CirrhosisSara Joseph100% (1)
- CH10Document17 pagesCH10Kim BasicNo ratings yet
- 97Document79 pages97HATLERNo ratings yet
- Psy101: Psychiatric Foundations and Psychological Reaction To DisabilityDocument30 pagesPsy101: Psychiatric Foundations and Psychological Reaction To DisabilityAlexia Ofel DinsonNo ratings yet
- Respiratory Osce: AMSA Edinburgh X IMU Y4Document34 pagesRespiratory Osce: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Acute Tubular NecrosisDocument60 pagesAcute Tubular NecrosisYedesney C. LinaresNo ratings yet
- Pathoma 2087m (34h47) : 1) Growth Adaptations, Cell Injury 154 MinsDocument11 pagesPathoma 2087m (34h47) : 1) Growth Adaptations, Cell Injury 154 Minsgreen mateNo ratings yet
- Structural Biology of HIVDocument31 pagesStructural Biology of HIVLaura TapiaNo ratings yet
- Anastomosis Left Anterior Cerebral Artery BlockageDocument5 pagesAnastomosis Left Anterior Cerebral Artery BlockagemcwnotesNo ratings yet
- Chapter 3 Genetic VariationDocument21 pagesChapter 3 Genetic VariationAbdulkarimNo ratings yet
- Brainstem NucleiDocument9 pagesBrainstem Nucleiankur_1No ratings yet
- Cerebral Blood FlowDocument39 pagesCerebral Blood FlowRajat ThakurNo ratings yet
- CerebellumDocument14 pagesCerebellumapi-508474347No ratings yet
- Cardio Block 3Document62 pagesCardio Block 3Maya LaPradeNo ratings yet
- Nose & Paranasal Sinuses 2018Document63 pagesNose & Paranasal Sinuses 2018yasrul izadNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Schematic Diagram Wilson'S DiseaseDocument2 pagesSchematic Diagram Wilson'S DiseaseAmira CharmaineNo ratings yet
- Brainstem StrokesDocument4 pagesBrainstem StrokesChandniNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 pagesCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3No ratings yet
- Edema Pathology by Asif AliDocument21 pagesEdema Pathology by Asif AliHassan AsifNo ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- Anat 6.3 GSA Appendix - EsguerraDocument4 pagesAnat 6.3 GSA Appendix - Esguerralovelots1234No ratings yet
- Pharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraDocument39 pagesPharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraKim Nicole Villaflores0% (1)
- Upperlimb-Clinical CasesDocument18 pagesUpperlimb-Clinical CasesKambwe ChristopherNo ratings yet
- Disease Signs and Symptoms Deficiency/Problem Notes AmyloidosisDocument14 pagesDisease Signs and Symptoms Deficiency/Problem Notes AmyloidosisSriKavya DevineniNo ratings yet
- Genetic and Metabolic DisordersDocument16 pagesGenetic and Metabolic DisordersErin HillNo ratings yet
- IKD9 - Radiological Evaluation of Renal CystsDocument26 pagesIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNo ratings yet
- Cytogenetics Course PackDocument29 pagesCytogenetics Course Packanonymous squashNo ratings yet
- Block 1 Board Review - Lecture NotesDocument127 pagesBlock 1 Board Review - Lecture NotesCece RereNo ratings yet
- Axis DeviationDocument26 pagesAxis DeviationDanial HassanNo ratings yet
- Para Compre 2Document17 pagesPara Compre 2serainie maiNo ratings yet
- Normal Body FloraDocument1 pageNormal Body FloraJulia IshakNo ratings yet
- University of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyDocument7 pagesUniversity of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyWynlor AbarcaNo ratings yet
- Microscopic Morphology Myocardial InfarctionDocument10 pagesMicroscopic Morphology Myocardial InfarctionnathanielNo ratings yet
- Diseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapDocument15 pagesDiseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapJayesh MahajanNo ratings yet
- Virology NotesDocument81 pagesVirology NotesraulNo ratings yet
- Cell and Embryology: Ii. Tissue Slide PreparationDocument9 pagesCell and Embryology: Ii. Tissue Slide Preparationashley nicholeNo ratings yet
- Acute Leukaemias: DR Nilukshi Perera Consultant HaematologistDocument60 pagesAcute Leukaemias: DR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhite100% (2)
- Kidney TumorsDocument15 pagesKidney TumorsJose SirittNo ratings yet
- Sedimen UrinDocument73 pagesSedimen UrinHerbanu PramonoNo ratings yet
- Examination of The HipDocument33 pagesExamination of The HipTumbal BroNo ratings yet
- AB-M02-CH2.2-LIVER PATH-Diffuse & Metabolic Disease-1Document26 pagesAB-M02-CH2.2-LIVER PATH-Diffuse & Metabolic Disease-1Thomas AndersonNo ratings yet
- The Hematology SectionDocument4 pagesThe Hematology SectionVENUS LIRIA PANTINo ratings yet
- Hema Lec Prefinals ExamDocument18 pagesHema Lec Prefinals ExamMark jay LlanoNo ratings yet
- 300 FCPS MCQS Solved 2Document14 pages300 FCPS MCQS Solved 2AS IFNo ratings yet
- Microscopic ExaminationDocument9 pagesMicroscopic ExaminationMariella DingleNo ratings yet
- Nerve StructureDocument53 pagesNerve StructureMedulla Oblongata100% (1)
- Renal Annotated First Aid 2019Document38 pagesRenal Annotated First Aid 2019Heran TeferiNo ratings yet
- Staphylococcus Streptococcus: Propertie S Morpholo Gy Culture & Biochemi Cal ReactionsDocument3 pagesStaphylococcus Streptococcus: Propertie S Morpholo Gy Culture & Biochemi Cal ReactionsmadhuNo ratings yet
- Flow Cytometry: An Introduction and Application To Cytology: December 2018Document12 pagesFlow Cytometry: An Introduction and Application To Cytology: December 2018ABHINABA GUPTANo ratings yet
- Chronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminDocument24 pagesChronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminMJ Putra100% (1)
- CHAPTER ONE To THREEDocument84 pagesCHAPTER ONE To THREEMonju GraceNo ratings yet
- Ischemic Heart DiseaseDocument4 pagesIschemic Heart DiseaseBanana CakeNo ratings yet
- SLE Pathogenesis, Clinical FeaturesDocument30 pagesSLE Pathogenesis, Clinical FeaturesJuwita PratiwiNo ratings yet
- Benign WBC Disorders Third YaerDocument27 pagesBenign WBC Disorders Third YaerAisho KeyfNo ratings yet
- Beri Beri: Water-Soluble Vitamins ThiamineDocument3 pagesBeri Beri: Water-Soluble Vitamins ThiamineLyan SamsonNo ratings yet
- Gluteal Region, Back of The Thigh and Popliteal Fossa.Document81 pagesGluteal Region, Back of The Thigh and Popliteal Fossa.Cupid MohNo ratings yet
- Ischemic Heart Disease (IHD)Document35 pagesIschemic Heart Disease (IHD)Ali Akand AsifNo ratings yet
- Coronary Artery DisaeseDocument48 pagesCoronary Artery DisaeseAzkaZulfiqarNo ratings yet
- MigraineDocument24 pagesMigraineHarsha MaheshwariNo ratings yet
- General Anesthetic 2016Document33 pagesGeneral Anesthetic 2016Harsha MaheshwariNo ratings yet
- LUNGS GuessDocument2 pagesLUNGS GuessHarsha MaheshwariNo ratings yet
- Community Medicine-1Document9 pagesCommunity Medicine-1Harsha MaheshwariNo ratings yet
- Epilepsy2018Document41 pagesEpilepsy2018Harsha MaheshwariNo ratings yet
- 4 5958464350862706598Document8 pages4 5958464350862706598Harsha MaheshwariNo ratings yet
- Cyanide Poisoning SlidesDocument22 pagesCyanide Poisoning SlidesHarsha MaheshwariNo ratings yet
- Overview of LymphomasDocument44 pagesOverview of LymphomasHarsha MaheshwariNo ratings yet
- Gastrulationin MammalsDocument16 pagesGastrulationin MammalsHarsha MaheshwariNo ratings yet
- Stroke Volume, Work, Cardiac Output, Ficks Principal, Laplace Law, Preload CVS by TKJDocument13 pagesStroke Volume, Work, Cardiac Output, Ficks Principal, Laplace Law, Preload CVS by TKJHarsha MaheshwariNo ratings yet
- Faiq AhmedDocument76 pagesFaiq AhmedHarsha MaheshwariNo ratings yet
- Respo-1 MBBS'26Document48 pagesRespo-1 MBBS'26Harsha MaheshwariNo ratings yet
- CHAPTER-04 (TESTt-01)Document10 pagesCHAPTER-04 (TESTt-01)Harsha MaheshwariNo ratings yet
- Physics Points-Chapter-4Document7 pagesPhysics Points-Chapter-4Harsha MaheshwariNo ratings yet
- 1 GluconeogenesisDocument7 pages1 GluconeogenesisHarsha MaheshwariNo ratings yet
- Loco - Respo TEHSEENDocument9 pagesLoco - Respo TEHSEENHarsha MaheshwariNo ratings yet
- Blood Vessels L2Document40 pagesBlood Vessels L2tas xoNo ratings yet
- Test About Circulatory SystemDocument5 pagesTest About Circulatory SystemThảo VânNo ratings yet
- Cardiac ImagingDocument118 pagesCardiac ImagingSay DieukayNo ratings yet
- Jurnal Kulit VaskulitisDocument7 pagesJurnal Kulit VaskulitisSMA N 1 TOROHNo ratings yet
- BFO-Review of Pathology AFODocument32 pagesBFO-Review of Pathology AFOnovitaNo ratings yet
- Life Sciences Grade 10 Learner Support Document MAFUMANI SECONDARYDocument40 pagesLife Sciences Grade 10 Learner Support Document MAFUMANI SECONDARYdeveloping habit and lifestyle of praise and worshNo ratings yet
- RLE FUNDA Test CompilationDocument25 pagesRLE FUNDA Test CompilationAngelika VeluzNo ratings yet
- Burns: Pathophysiology Types Degree PercentageDocument19 pagesBurns: Pathophysiology Types Degree PercentageanuzNo ratings yet
- Sample Book: Vasodilator DrugsDocument4 pagesSample Book: Vasodilator DrugsManangioma ManNo ratings yet
- General Biology II q4 Week 2Document26 pagesGeneral Biology II q4 Week 2Educhamp Learning CenterNo ratings yet
- Lesson 4: Homeostasis and Cells:: The Cell As An OrganismDocument6 pagesLesson 4: Homeostasis and Cells:: The Cell As An Organismrakan ilyasNo ratings yet
- Medical TerminologiesDocument14 pagesMedical TerminologiesShannine Del Rosario BeridaNo ratings yet
- Lesson 4 Blood VesselsDocument14 pagesLesson 4 Blood VesselsCarolyn D MayugaNo ratings yet
- Dar 1997Document3 pagesDar 1997Sarly FebrianaNo ratings yet
- 27 GuytonDocument6 pages27 GuytonBianca Louise Chan LimNo ratings yet
- Mercury Mercruiser Marine Engine 32-4-3l Mpi Gasoline Service ManualDocument22 pagesMercury Mercruiser Marine Engine 32-4-3l Mpi Gasoline Service Manualjamesmiller060901qms100% (33)
- Avascular Necrosis - Causes, Symptoms, Prevention & TreatmentDocument26 pagesAvascular Necrosis - Causes, Symptoms, Prevention & TreatmentSatrio Bangun NegoroNo ratings yet
- Digestive Tract Detoxification GI Health Depends PDFDocument20 pagesDigestive Tract Detoxification GI Health Depends PDFPablo CrespoNo ratings yet
- Inflammation: Cardinal Signs of InflammationDocument9 pagesInflammation: Cardinal Signs of InflammationGeoffreyNo ratings yet
- 6 Seeds To Heaven PDFDocument37 pages6 Seeds To Heaven PDFSarbu Stacy100% (1)
- 7.1 Petermann PCLACDocument11 pages7.1 Petermann PCLACbob marley100% (1)
- Respiration and Transportation WorksheetDocument4 pagesRespiration and Transportation WorksheetAarjav JainNo ratings yet
- NCA - CVA InfarctDocument126 pagesNCA - CVA InfarctRosaree Mae PantojaNo ratings yet
- Fish OilsDocument36 pagesFish OilsGabiNo ratings yet
- Chapter 6. The Circulatory System: Short QuestionsDocument31 pagesChapter 6. The Circulatory System: Short QuestionsParardha DharNo ratings yet
- Arterial UlcersDocument8 pagesArterial Ulcerspka25No ratings yet
- Aging Changes in The Heart and Blood VesselsDocument4 pagesAging Changes in The Heart and Blood VesselsTotalenesya Reforrent SutiknoNo ratings yet