Download as pdf or txt
You might also like
- 1 s2.0 S0140673622014854 MainDocument12 pages1 s2.0 S0140673622014854 Mainsilvia100% (1)
- Review: Alexander P J Vlaar, Nicole P Juff ErmansDocument11 pagesReview: Alexander P J Vlaar, Nicole P Juff ErmanssinarNo ratings yet
- Transfusion-Related Acute Lung Injury: Review ArticleDocument9 pagesTransfusion-Related Acute Lung Injury: Review ArticleAinunNadzirohNo ratings yet
- Committeereport: A Consensus Rede Finition of Transfusion-Related Acute Lung InjuryDocument12 pagesCommitteereport: A Consensus Rede Finition of Transfusion-Related Acute Lung InjuryAdrian ArnasaputraNo ratings yet
- Transfusion-Related Acute Lung Injury Risk Mitigation: An UpdateDocument10 pagesTransfusion-Related Acute Lung Injury Risk Mitigation: An UpdateAlfa FebriandaNo ratings yet
- Dilemma in PEDocument7 pagesDilemma in PEGosia JasiewiczNo ratings yet
- Transfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung InjuryDocument14 pagesTransfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung InjuryKaemacCrackercherryzebraNo ratings yet
- (TRALI) Cudilo2015Document4 pages(TRALI) Cudilo2015abu abdirrahmanNo ratings yet
- Transfusion-Related Acute Lung Injury and TransfusDocument4 pagesTransfusion-Related Acute Lung Injury and TransfusShanaz NovriandinaNo ratings yet
- Seminar: Nuala J Meyer, Luciano Gattinoni, Carolyn S CalfeeDocument16 pagesSeminar: Nuala J Meyer, Luciano Gattinoni, Carolyn S CalfeeDiana AngelesNo ratings yet
- Trali Uptodate PDFDocument36 pagesTrali Uptodate PDFTety M. DorisNo ratings yet
- Transfusion-Related Acute Lung Injury (Trali) : Description and IncidenceDocument9 pagesTransfusion-Related Acute Lung Injury (Trali) : Description and IncidenceNanda SilvaNo ratings yet
- TraliDocument10 pagesTraliMatilde Silva GonçalvesNo ratings yet
- Transfusion-Related Acute Lung Injury: HistoryDocument20 pagesTransfusion-Related Acute Lung Injury: HistoryBladimir CentenoNo ratings yet
- Distinguishing TRALI and TACODocument6 pagesDistinguishing TRALI and TACOl1o2stNo ratings yet
- Transfusion-Related Acute Lung Injury: A Literature Review: ReviewarticleDocument9 pagesTransfusion-Related Acute Lung Injury: A Literature Review: ReviewarticlekereklovagNo ratings yet
- Subphenotyping ARDS in COVID-19 Patients: Consequences For Ventilator ManagementDocument10 pagesSubphenotyping ARDS in COVID-19 Patients: Consequences For Ventilator ManagementPaola Andrade ValenciaNo ratings yet
- Juffermans Et Al-2020-Intensive Care MedicineDocument8 pagesJuffermans Et Al-2020-Intensive Care MedicineHalonzo RománNo ratings yet
- Chen 2015Document6 pagesChen 2015nurminsyahNo ratings yet
- 4Document16 pages4Ihsanul Ma'arifNo ratings yet
- Transfusion-Related Acute Lung Injury - StatPearls - NCBI BookshelfDocument5 pagesTransfusion-Related Acute Lung Injury - StatPearls - NCBI Bookshelfindahmsafitri3No ratings yet
- Alveolar HaemorragicDocument12 pagesAlveolar Haemorragicmedicina146No ratings yet
- Z. Citasi Piis014067362030917xDocument3 pagesZ. Citasi Piis014067362030917xMastifa HanasitaNo ratings yet
- © Simtipro SRLDocument11 pages© Simtipro SRLMoncef PechaNo ratings yet
- Transfusion-Related Acute Lung Injury: Pearl Toy,, and Ognjen GajicDocument2 pagesTransfusion-Related Acute Lung Injury: Pearl Toy,, and Ognjen GajicMaulana Akbar LubisNo ratings yet
- TRALI Review 2009 PDFDocument11 pagesTRALI Review 2009 PDFTitin AliyaturNo ratings yet
- Risk Factors For Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewDocument11 pagesRisk Factors For Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewKorwin TitlaNo ratings yet
- Sdra Reconocimiento Actual 2021Document16 pagesSdra Reconocimiento Actual 2021NATHALY JOVANA CONTRERAS HERRERANo ratings yet
- Articulo Trombocitipenia Por Vacuna CovidDocument10 pagesArticulo Trombocitipenia Por Vacuna CovidAlex de la RNo ratings yet
- From Gold 0 To Pre-CopdDocument10 pagesFrom Gold 0 To Pre-CopdLorena ZirondiNo ratings yet
- Acute Respiratory Distress Syndrome 2021 LancetDocument16 pagesAcute Respiratory Distress Syndrome 2021 LancetCláudia SilvaNo ratings yet
- Connective Tissue Disease-Associated Interstitial Lung Diseases: Unresolved IssuesDocument9 pagesConnective Tissue Disease-Associated Interstitial Lung Diseases: Unresolved IssuesNuntana ChampaNo ratings yet
- Int Care Med 2007Document5 pagesInt Care Med 2007sccNo ratings yet
- Chronic Airspace DiseasesDocument31 pagesChronic Airspace DiseasesAnkita ShahNo ratings yet
- Wu 2021Document8 pagesWu 2021Pulmonologi Dan Kedokteran Respirasi FK UNRINo ratings yet
- Review: Paolo Spagnolo, Giulio Rossi, Rocco Trisolini, Nicola Sverzellati, Robert P Baughman, Athol U WellsDocument14 pagesReview: Paolo Spagnolo, Giulio Rossi, Rocco Trisolini, Nicola Sverzellati, Robert P Baughman, Athol U Wellsandra mNo ratings yet
- 11 Acute Respiratory Distress Syndrome NEJM Thompson2017Document11 pages11 Acute Respiratory Distress Syndrome NEJM Thompson2017Camila Andrea PeñaNo ratings yet
- Anticoagulation in COVID-19: A Systematic Review, Meta-Analysis, and Rapid Guidance From Mayo ClinicDocument20 pagesAnticoagulation in COVID-19: A Systematic Review, Meta-Analysis, and Rapid Guidance From Mayo ClinicAndi Tiara S. AdamNo ratings yet
- Interstitial Pneumonia With Autoimmune Features Challenges and ControversieDocument19 pagesInterstitial Pneumonia With Autoimmune Features Challenges and ControversieVitória WasserNo ratings yet
- Analisis Comparativo Ipaf Vs EasDocument9 pagesAnalisis Comparativo Ipaf Vs Easpkh5qpp8j5No ratings yet
- Algoritma ARDSDocument7 pagesAlgoritma ARDSSri AgustinaNo ratings yet
- Accepted Manuscript: 10.1016/j.chest.2016.02.635Document21 pagesAccepted Manuscript: 10.1016/j.chest.2016.02.635Vic HNNo ratings yet
- Chronic Interstitial Lung Diseases in Children: Diagnosis ApproachesDocument30 pagesChronic Interstitial Lung Diseases in Children: Diagnosis Approachesgustavo adolfo rodriguez alzateNo ratings yet
- Copd 1Document8 pagesCopd 1Meinita M.DNo ratings yet
- PIIS1076633220302464Document1 pagePIIS1076633220302464India SunshineNo ratings yet
- Transfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung InjuryDocument14 pagesTransfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung InjuryGloria ThomasNo ratings yet
- Interpretación de Patrones Radiológicos Sugerentes de Covid-19 en PediatríaDocument9 pagesInterpretación de Patrones Radiológicos Sugerentes de Covid-19 en PediatríaJuan M SagnirbNo ratings yet
- Correspondence: Smell and Taste Dysfunction in Patients With COVID-19Document1 pageCorrespondence: Smell and Taste Dysfunction in Patients With COVID-19Dhyo Asy-shidiq HasNo ratings yet
- ISTH Interim Guidance On Recognition and Management of Coagulopathy in COVID-19Document8 pagesISTH Interim Guidance On Recognition and Management of Coagulopathy in COVID-19hellonduttyNo ratings yet
- 1 s2.0 S0140673622014398 MainDocument14 pages1 s2.0 S0140673622014398 Maintaaaatan.04No ratings yet
- A Case Series Describing The Epidemiology and Clinical Characteristics of COVID-19 Infection in Jilin ProvinceDocument4 pagesA Case Series Describing The Epidemiology and Clinical Characteristics of COVID-19 Infection in Jilin Provinceabeer alrofaeyNo ratings yet
- HHS Public Access: SyphilisDocument49 pagesHHS Public Access: Syphilisfaty basalamahNo ratings yet
- JMV 25815Document2 pagesJMV 25815fadil ahmadiNo ratings yet
- Reaksi Transfusi, TRALI Vs TACODocument12 pagesReaksi Transfusi, TRALI Vs TACOifadhrohayatNo ratings yet
- Pulmonary Tuberculosis Presenting With Acute Respiratory Distress Syndrome (Ards) : A Case Report and Review of LiteratureDocument5 pagesPulmonary Tuberculosis Presenting With Acute Respiratory Distress Syndrome (Ards) : A Case Report and Review of Literatureamelya asryNo ratings yet
- Complicatii PneumonieDocument9 pagesComplicatii PneumonieTatiana JalbaNo ratings yet
- Pathological Evidence of Pulmonary Thrombotic Phenomena in Severe COVID 19Document5 pagesPathological Evidence of Pulmonary Thrombotic Phenomena in Severe COVID 19Victor AugustoNo ratings yet
- Acute Respiratory Distress Syndrome: Etiology, Pathogenesis, and Summary On ManagementDocument15 pagesAcute Respiratory Distress Syndrome: Etiology, Pathogenesis, and Summary On ManagementLiri AndiyaniNo ratings yet
- (PULMO) 2012 ARDS - The New Berlin DefinitionDocument4 pages(PULMO) 2012 ARDS - The New Berlin DefinitionerikaNo ratings yet
- J Jaad 2008 12 046Document3 pagesJ Jaad 2008 12 046Moncef PechaNo ratings yet
- Life History of Cutaneous Vascular Lesions in Sneddon's SyndromeDocument8 pagesLife History of Cutaneous Vascular Lesions in Sneddon's SyndromeMoncef PechaNo ratings yet
- J Ekir 2020 12 039Document8 pagesJ Ekir 2020 12 039Moncef PechaNo ratings yet
- Soares Et Al 2016 Prognosis of Critically Ill Patients With Cancer and Acute Renal DysfunctionDocument14 pagesSoares Et Al 2016 Prognosis of Critically Ill Patients With Cancer and Acute Renal DysfunctionMoncef PechaNo ratings yet
- © Simtipro SRLDocument8 pages© Simtipro SRLMoncef PechaNo ratings yet
- © Simtipro SRLDocument11 pages© Simtipro SRLMoncef PechaNo ratings yet
- © Simtipro SRLDocument8 pages© Simtipro SRLMoncef PechaNo ratings yet
- 150QCM EmbryologieDocument66 pages150QCM EmbryologieMoncef PechaNo ratings yet
- © Simtipro SRL: A New Blood Group System: Scientific Relevance and Media ResonanceDocument2 pages© Simtipro SRL: A New Blood Group System: Scientific Relevance and Media ResonanceMoncef PechaNo ratings yet
- General Transfusion Practice Quiz For Rotating Medical StaffDocument3 pagesGeneral Transfusion Practice Quiz For Rotating Medical StaffaymenNo ratings yet
- HematologyDocument8 pagesHematologySameera Al MerriNo ratings yet
- Medical Devices: Selection of Tests For Interactions With Blood 10993-4Document10 pagesMedical Devices: Selection of Tests For Interactions With Blood 10993-4Muhammad ImranNo ratings yet
- Anemia Defisiensi Besi Pada Pasien Dengan Ulkus Peptikum: Laporan KasusDocument4 pagesAnemia Defisiensi Besi Pada Pasien Dengan Ulkus Peptikum: Laporan KasusAzura SyahadatiNo ratings yet
- Aragon, Annie Lynn Silverio 2487019192Document5 pagesAragon, Annie Lynn Silverio 2487019192Samuel AragonNo ratings yet
- Blood Bank International Standard ISBT Science Series - 2008 - Hardwick - Blood ProcessingDocument29 pagesBlood Bank International Standard ISBT Science Series - 2008 - Hardwick - Blood ProcessingShan AhmadNo ratings yet
- Management TTPDocument14 pagesManagement TTPSutirtho MukherjiNo ratings yet
- HematDocument3 pagesHematMohit AbhyankarNo ratings yet
- The Study On The Anti - Anemic Effect of Banana Peel Extract Against Gentamicin - Induced Anemic Male Albino RATS (Rattus Norvegicus)Document32 pagesThe Study On The Anti - Anemic Effect of Banana Peel Extract Against Gentamicin - Induced Anemic Male Albino RATS (Rattus Norvegicus)Maraiah BautistaNo ratings yet
- An Introduction To Haematopoiesis Prof Vernon Louw Clinical Haematology University of Cape TownDocument35 pagesAn Introduction To Haematopoiesis Prof Vernon Louw Clinical Haematology University of Cape TownAmmaarah IsaacsNo ratings yet
- Isaac Typhoid NegativeDocument5 pagesIsaac Typhoid Negativeganesh khondeNo ratings yet
- Shalamar Hospital Laboratory: LLFFLLLLLLLLLLLLLLLLLLDocument1 pageShalamar Hospital Laboratory: LLFFLLLLLLLLLLLLLLLLLLAfaq MehmoodNo ratings yet
- Complete Blood Count (CBC) Normal Laboratory Study Values: DefinitionDocument6 pagesComplete Blood Count (CBC) Normal Laboratory Study Values: DefinitionGlare RhayneNo ratings yet
- The Child With Hematologic DisordersDocument149 pagesThe Child With Hematologic DisordersNics FranciscoNo ratings yet
- Blood Bank PracticalDocument24 pagesBlood Bank Practicalmoonfire2009No ratings yet
- Adobe Scan 09 Jan 2024Document2 pagesAdobe Scan 09 Jan 2024swapna vijayNo ratings yet
- Blood Donation Research Paper - LatestDocument10 pagesBlood Donation Research Paper - LatestEileen1113100% (2)
- Laboratory Report: Consultant PathologistDocument2 pagesLaboratory Report: Consultant Pathologisttafiki4253No ratings yet
- HPLC Vs HB ElectrophoresisDocument10 pagesHPLC Vs HB ElectrophoresisRajeev Rajeshuni100% (1)
- Heparin MedicationDocument1 pageHeparin Medicationtriagestation100% (2)
- (Blood Group) Department of Public Health Fall 2020, Lab Manual (PBH101L)Document2 pages(Blood Group) Department of Public Health Fall 2020, Lab Manual (PBH101L)MunniNo ratings yet
- Hemograma Buna 2023 BunaDocument71 pagesHemograma Buna 2023 BunaMirelDabuleanuNo ratings yet
- Hemoglobinopathy - WikipediaDocument9 pagesHemoglobinopathy - WikipediaEslam NassarNo ratings yet
- Case Study ON: Blood DyscrasiaDocument40 pagesCase Study ON: Blood DyscrasiaJM RomiasNo ratings yet
- COMPLETE BLOOD COUNT Lecture GuideDocument9 pagesCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaNo ratings yet
- Differential Diagnosis of Microcytic Anemia PDFDocument5 pagesDifferential Diagnosis of Microcytic Anemia PDFayms99No ratings yet
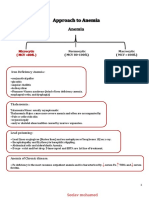
- Approach To AnemiaDocument4 pagesApproach To AnemiapNo ratings yet
- Presentation On AnaemiaDocument19 pagesPresentation On AnaemiaAnkit MalikNo ratings yet
- Sysmex SEED The Importance of Reticulocyte Detection PDFDocument8 pagesSysmex SEED The Importance of Reticulocyte Detection PDFRaluca BadeaNo ratings yet
- Vitamin B12 Deficiency and Anemia in 140 Taiwanese Female Lacto-VegetariansDocument13 pagesVitamin B12 Deficiency and Anemia in 140 Taiwanese Female Lacto-VegetariansLunaNo ratings yet