Download as pdf or txt
You might also like
- Solution Manual For Nutrition Exercise and Behavior An Integrated Approach To Weight Management 3rd Edition Summerfield 1305258770 9781305258778Document36 pagesSolution Manual For Nutrition Exercise and Behavior An Integrated Approach To Weight Management 3rd Edition Summerfield 1305258770 9781305258778julierileyjmaqypbftz100% (30)
- Pathophysiology of Metabolic SyndromeDocument5 pagesPathophysiology of Metabolic SyndromeAgeng BudianantiNo ratings yet
- Advanced Pharmaceutical analysisFrom EverandAdvanced Pharmaceutical analysisRating: 4.5 out of 5 stars4.5/5 (2)
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Acid Base BalanceDocument44 pagesAcid Base BalanceKenny JapNo ratings yet
- Acid Base Balance 2B - 3.05.2021Document56 pagesAcid Base Balance 2B - 3.05.2021Kavya FouzdarNo ratings yet
- Acid Base BalaneceDocument11 pagesAcid Base BalaneceHAMMYER ALROKHAMINo ratings yet
- Acid/Base Am Didactic Teaching Guide: Learning ObjectivesDocument3 pagesAcid/Base Am Didactic Teaching Guide: Learning ObjectivesAdrian CamposNo ratings yet
- ABG Algorithm PDFDocument2 pagesABG Algorithm PDFamin2014No ratings yet
- Acid - Base BalanceDocument41 pagesAcid - Base BalanceEgun Nuel DNo ratings yet
- Acid Base PhysiologyDocument4 pagesAcid Base PhysiologyGhadeer EbraheemNo ratings yet
- ABGDocument45 pagesABGHasan SudirgoNo ratings yet
- Acid-Base DisordersDocument46 pagesAcid-Base DisordersqazNo ratings yet
- Acid-Base Disorder 27 July 2017Document48 pagesAcid-Base Disorder 27 July 2017Pauline ChanNo ratings yet
- Acid-Base Disorder 27 July 2017 PDFDocument48 pagesAcid-Base Disorder 27 July 2017 PDFPauline ChanNo ratings yet
- ABG - Manuel Antonio Ko, MD 2008Document58 pagesABG - Manuel Antonio Ko, MD 2008Nguyen Minh DucNo ratings yet
- Acid Base Phsyiology AnswersDocument30 pagesAcid Base Phsyiology AnswersSharif ImamNo ratings yet
- ABG AnalysisDocument46 pagesABG Analysisregole100% (1)
- Blood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical CareDocument48 pagesBlood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical Carehagir alhajNo ratings yet
- 2016 Acid Base DisordersDocument48 pages2016 Acid Base DisordersbellabelbonNo ratings yet
- Acid BaseDocument6 pagesAcid BaseCarol Solanyi Gacha QuinteroNo ratings yet
- The Patient With Acid-Base Disorder: Students Approach To The ProblemDocument42 pagesThe Patient With Acid-Base Disorder: Students Approach To The ProblemOliviaLaneNo ratings yet
- Blood Gas AnalysisDocument52 pagesBlood Gas AnalysisKresna Dharma SuryanaNo ratings yet
- Acid-Base and Electrolyte DisordersDocument41 pagesAcid-Base and Electrolyte Disordersaantoxx84No ratings yet
- ABG MMHG InterpretationDocument92 pagesABG MMHG InterpretationManmeet SNo ratings yet
- Arterial Blood Gas.Document4 pagesArterial Blood Gas.Sathish KumarNo ratings yet
- Acid-Base Balance and Anion GapDocument37 pagesAcid-Base Balance and Anion GapMsa AhhfaaNo ratings yet
- ABGs InterpretationDocument33 pagesABGs InterpretationHamza DossaNo ratings yet
- ABG InterpertationDocument14 pagesABG Interpertationapi-3757039100% (1)
- Arterial Blood Gas: AnalysisDocument51 pagesArterial Blood Gas: Analysisnaven100% (2)
- Marc D. Berg, MD - Devos Children'S Hospital Rita R. Ongjoco, Do - Sinai Hospital of BaltimoreDocument41 pagesMarc D. Berg, MD - Devos Children'S Hospital Rita R. Ongjoco, Do - Sinai Hospital of BaltimoreAhmed KamalNo ratings yet
- Acid-Base Interpretation: APRIL 4, 2017Document9 pagesAcid-Base Interpretation: APRIL 4, 2017mohamedsmnNo ratings yet
- ABGAnalysis Resident LectureDocument71 pagesABGAnalysis Resident LecturePutu AdhekNo ratings yet
- © Dept. of Medical and Clinical Biochemistry Upjš in Košice, Medical Faculty Eva Ďurovcová, MD, PHDDocument51 pages© Dept. of Medical and Clinical Biochemistry Upjš in Košice, Medical Faculty Eva Ďurovcová, MD, PHDPaulina PaskeviciuteNo ratings yet
- Arterial Blood GAS InterpretationDocument25 pagesArterial Blood GAS Interpretationliyahanna02No ratings yet
- Structured Approach To Acid Base InterpretationDocument14 pagesStructured Approach To Acid Base InterpretationAnna MNo ratings yet
- Stepwise Approach To Acid-Base AnalysisDocument16 pagesStepwise Approach To Acid-Base AnalysisTryanto Amrisal MohammadNo ratings yet
- Acid Base Disorders: Mr. Ahmed Alnaji Mbchb. Mrcs 1+2 Palestinian Board G. Surgery European Gaza HospitalDocument60 pagesAcid Base Disorders: Mr. Ahmed Alnaji Mbchb. Mrcs 1+2 Palestinian Board G. Surgery European Gaza Hospitalpt.mahmoudNo ratings yet
- Approach Acid Base ProblemsDocument40 pagesApproach Acid Base Problemsnanang anacardia SubagyoNo ratings yet
- Abg InterpretationDocument52 pagesAbg InterpretationCirugia Cardiovascular NeivaNo ratings yet
- Acid Base BalanceDocument18 pagesAcid Base BalanceRichard PoonNo ratings yet
- Approach To Acid BaseDocument4 pagesApproach To Acid BaseJose Carlos Guerrero AcostaNo ratings yet
- ABG AnalysisDocument26 pagesABG Analysisf5psw2zk6fNo ratings yet
- Acid BaseDocument33 pagesAcid BaseParvathy R NairNo ratings yet
- Protocol - ABG Analysis by DR FazalDocument2 pagesProtocol - ABG Analysis by DR FazalSalmanNo ratings yet
- American Thoracic Society - Interpretation of Arterial Blood Gases (ABGs)Document8 pagesAmerican Thoracic Society - Interpretation of Arterial Blood Gases (ABGs)muhammadridhwanNo ratings yet
- Blood Gas AnalysisDocument5 pagesBlood Gas Analysissraji64No ratings yet
- Interpretasi ABGDocument5 pagesInterpretasi ABGNella Rosyalina DamayantiNo ratings yet
- Abg PPT NewDocument69 pagesAbg PPT NewMalaka Atapattu100% (3)
- Acid Base StatusDocument28 pagesAcid Base Statustoto loloNo ratings yet
- Y5 RN - Abgs 27oct2010Document5 pagesY5 RN - Abgs 27oct2010Canh VanNo ratings yet
- Michael Chansky Acid Base Made Easy HandoutDocument18 pagesMichael Chansky Acid Base Made Easy HandoutTeguh RamadhanNo ratings yet
- Acid Base BalanceDocument46 pagesAcid Base Balanceleesteph78No ratings yet
- Moderator: Dr. R. K. Yadav (MD) Presented By: Ashish JaisawalDocument47 pagesModerator: Dr. R. K. Yadav (MD) Presented By: Ashish Jaisawalimranqazi11No ratings yet
- Pneumonia - Kyphoscoliosis - Morbid Obesity - Drug OverdoseDocument3 pagesPneumonia - Kyphoscoliosis - Morbid Obesity - Drug OverdoseJessica nonyeNo ratings yet
- Basic Acid Base Balance - Practical Approach - MRNDocument9 pagesBasic Acid Base Balance - Practical Approach - MRNmuhammad rahmatsyah nasutionNo ratings yet
- Acidosis Alkalosis BiochemistryDocument31 pagesAcidosis Alkalosis BiochemistryliyaNo ratings yet
- Dec PH Opp Inc PH Opp: Rule 1: Rule 2Document3 pagesDec PH Opp Inc PH Opp: Rule 1: Rule 2Solomon Seth SallforsNo ratings yet
- Grami Renal Learning Issue ABG Use and Interpretation Version 2Document10 pagesGrami Renal Learning Issue ABG Use and Interpretation Version 2RomilPatelNo ratings yet
- Arterial Blood Gas Analysis-1Document74 pagesArterial Blood Gas Analysis-1ArunNo ratings yet
- Asidosis Metabolik PDFDocument6 pagesAsidosis Metabolik PDFafifurrahman_rizalNo ratings yet
- The Role of USG in ED (Ali Haedar)Document27 pagesThe Role of USG in ED (Ali Haedar)Bayu AkbarNo ratings yet
- Resuscitation Drugs (Ali Haedar)Document41 pagesResuscitation Drugs (Ali Haedar)Bayu AkbarNo ratings yet
- Electrolytes Emergencies (Ali Haedar)Document36 pagesElectrolytes Emergencies (Ali Haedar)Bayu AkbarNo ratings yet
- Hematology & Coagulation Study (Ali Haedar)Document16 pagesHematology & Coagulation Study (Ali Haedar)Bayu AkbarNo ratings yet
- Integrated Emergency Medical Services SystemDocument67 pagesIntegrated Emergency Medical Services SystemBayu AkbarNo ratings yet
- ECG & ArrhytmiaDocument46 pagesECG & ArrhytmiaBayu AkbarNo ratings yet
- WJAHR 282 Jurnal Bayu Akbar TesisDocument5 pagesWJAHR 282 Jurnal Bayu Akbar TesisBayu AkbarNo ratings yet
- Diabetic RetinopathyDocument13 pagesDiabetic RetinopathyMuhammad Rhema0% (1)
- Obesity PresentationDocument21 pagesObesity Presentationapi-433262794No ratings yet
- Graphic Organizer ExampleDocument1 pageGraphic Organizer Exampleapi-398530613No ratings yet
- Names: Manuel I Santos Memorial National High SchoolDocument4 pagesNames: Manuel I Santos Memorial National High SchoolWella Alyana CelestinoNo ratings yet
- Pathfi Module 1: Movement: C. Manipulative SkillsDocument4 pagesPathfi Module 1: Movement: C. Manipulative SkillsAndrea Gail UlitinNo ratings yet
- Gambaran Asupan Cairan Dan Status Gizi Pada Mahasiswa Kedokteran Universitas JambiDocument8 pagesGambaran Asupan Cairan Dan Status Gizi Pada Mahasiswa Kedokteran Universitas Jambiilham yuriNo ratings yet
- Stroke Risk Scorecard 2018Document2 pagesStroke Risk Scorecard 2018wahyu satriaNo ratings yet
- مصطفى مهدى صالح-81692Document5 pagesمصطفى مهدى صالح-81692Muntadher KareemNo ratings yet
- Ketogenic DietDocument60 pagesKetogenic DietKanchi Mitra BhargavNo ratings yet
- Oxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaDocument9 pagesOxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaidiNo ratings yet
- Metabolic Syndrome and StrokeDocument5 pagesMetabolic Syndrome and StrokeEmir SaricNo ratings yet
- Read The Passage of Obesity and Health'. Answer The Questions That FollowDocument3 pagesRead The Passage of Obesity and Health'. Answer The Questions That FollowLokman HakimNo ratings yet
- Foods That Promote Liver Health - Pritikin Weight Loss Resort PDFDocument6 pagesFoods That Promote Liver Health - Pritikin Weight Loss Resort PDFPallabi RoyNo ratings yet
- The Complete Weight Loss Guide: Brought To You byDocument6 pagesThe Complete Weight Loss Guide: Brought To You bySam YoussefNo ratings yet
- The Blueprint To Fasting For Fat Loss - V1.3 - 03-1-2023Document20 pagesThe Blueprint To Fasting For Fat Loss - V1.3 - 03-1-2023Riaan CoetzeeNo ratings yet
- Anjana Et AlDocument1 pageAnjana Et AlmegasyifaNo ratings yet
- 457 126619 3 10 20191010Document6 pages457 126619 3 10 20191010maarifah ifahNo ratings yet
- Physical Fitness Unit TwoDocument37 pagesPhysical Fitness Unit TwoMullisaa Sabaa HimuureeNo ratings yet
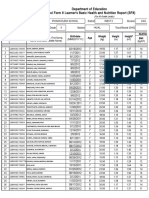
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Document4 pagesDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Roxan DosdosNo ratings yet
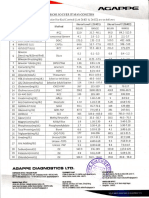
- Biorad InsertDocument1 pageBiorad InsertJohnmar AquinoNo ratings yet
- Obesity PPT 1416heDocument11 pagesObesity PPT 1416heMeity ElvinaNo ratings yet
- Kunjungan Lab PKM Pomalaa BLN Feb 2022Document1 pageKunjungan Lab PKM Pomalaa BLN Feb 2022RifaldiNo ratings yet
- Adaptaciones Spinreact BS240 ProDocument1 pageAdaptaciones Spinreact BS240 ProClaudia Gonzalez CuisaNo ratings yet
- Full Document For HealthDocument3 pagesFull Document For HealthDotto MakinaNo ratings yet
- Alert !!! 10-12 Hours Fasting Is Mandatory For Lipid Parameters. If Not, Values Might FluctuateDocument2 pagesAlert !!! 10-12 Hours Fasting Is Mandatory For Lipid Parameters. If Not, Values Might FluctuateArka Prava PaulNo ratings yet
- Trends in Epidemiology of Dyslipidemias in India 2024 Indian Heart JournalDocument9 pagesTrends in Epidemiology of Dyslipidemias in India 2024 Indian Heart Journallakshminivas PingaliNo ratings yet
- Obesity As Chronic DiseaseDocument37 pagesObesity As Chronic DiseaseMariana OlgaNo ratings yet
- School Form 8 (SF 8)Document1 pageSchool Form 8 (SF 8)Aquino ButsNo ratings yet