Download as pdf or txt
You might also like
- Brain Mapping An Encyclopedic Reference (-PUNISHER-)Document2,668 pagesBrain Mapping An Encyclopedic Reference (-PUNISHER-)Robin Smith100% (7)
- Anz Gog Rad Hyst HistoryDocument109 pagesAnz Gog Rad Hyst Historyinfo7615No ratings yet
- Icru 89 (229-260)Document32 pagesIcru 89 (229-260)Christian Ordoñez100% (1)
- Mini-IPX v5.0Document2 pagesMini-IPX v5.0Safia RehmanNo ratings yet
- Indeterminate Renal Mass ACR Appropriateness CriteriaDocument10 pagesIndeterminate Renal Mass ACR Appropriateness CriteriaAndrew TaliaferroNo ratings yet
- ACR Appropriateness Criteria For HematuriaDocument8 pagesACR Appropriateness Criteria For HematuriaAndrew TaliaferroNo ratings yet
- Onset Flank PainDocument11 pagesOnset Flank PainPipitNo ratings yet
- Major Blunt TraumaDocument18 pagesMajor Blunt TraumaghassanNo ratings yet
- Adrenal Mass EvaluationDocument19 pagesAdrenal Mass Evaluationpj rakNo ratings yet
- Acute Nonlocalized Abdominal PainDocument17 pagesAcute Nonlocalized Abdominal PainghassanNo ratings yet
- Acute PancreatitisDocument16 pagesAcute PancreatitisLoredana BoghezNo ratings yet
- Hematuria PDFDocument11 pagesHematuria PDFPipitNo ratings yet
- Acute Onset Flank Pain-Suspicion of Stone DiseaseDocument9 pagesAcute Onset Flank Pain-Suspicion of Stone DiseasecubirojasNo ratings yet
- Occupational Lung DiseasesDocument13 pagesOccupational Lung DiseasesVianney OlveraNo ratings yet
- American College of Radiology ACR Appropriateness CriteriaDocument7 pagesAmerican College of Radiology ACR Appropriateness CriteriaMeutia PutriNo ratings yet
- Abdominal Aortic Aneurysm-Interventional Planning and Follow-UpDocument13 pagesAbdominal Aortic Aneurysm-Interventional Planning and Follow-Upvictor contrerasNo ratings yet
- Low Back PainDocument22 pagesLow Back PainSF TifarinNo ratings yet
- Chylothorax Treatment PlanningDocument10 pagesChylothorax Treatment PlanningVianney OlveraNo ratings yet
- Abdominal Aortic Aneurysm Follow-Up (Without Repair)Document7 pagesAbdominal Aortic Aneurysm Follow-Up (Without Repair)victor contrerasNo ratings yet
- Acute Respiratory Illness in Immunocompetent PatientsDocument14 pagesAcute Respiratory Illness in Immunocompetent PatientsVianney OlveraNo ratings yet
- Infective EndocarditisDocument13 pagesInfective Endocarditispaquidermo85No ratings yet
- Acute Nonspecific Chest Pain-Low Probability of Coronary Artery DiseaseDocument10 pagesAcute Nonspecific Chest Pain-Low Probability of Coronary Artery Diseasevictor contrerasNo ratings yet
- Postmenopausal Subacute or Chronic Pelvic PainDocument9 pagesPostmenopausal Subacute or Chronic Pelvic PainM SNo ratings yet
- Radiologic Management of Upper Gastrointestinal BleedingDocument13 pagesRadiologic Management of Upper Gastrointestinal BleedingshadowlightfoxNo ratings yet
- ACR Appropriateness Criteria® Acute Chest Pain - Suspected Pulmonary Embolism.Document16 pagesACR Appropriateness Criteria® Acute Chest Pain - Suspected Pulmonary Embolism.Madalina TalpauNo ratings yet
- Acute Hip Pain-Suspected FractureDocument9 pagesAcute Hip Pain-Suspected FractureMario UmañaNo ratings yet
- Dyspnea-Suspected Cardiac Origin (Ischemia Already Excluded)Document20 pagesDyspnea-Suspected Cardiac Origin (Ischemia Already Excluded)Parth PatilNo ratings yet
- Abnormal Uterine BleedingDocument12 pagesAbnormal Uterine Bleedingvictor contrerasNo ratings yet
- Low Back PainDocument10 pagesLow Back Paindigimon666No ratings yet
- ACR Appropriateness Criteria Pancreatic CystDocument9 pagesACR Appropriateness Criteria Pancreatic CystSole GonzalezNo ratings yet
- Breast Implant Evaluation - NarrativeDocument25 pagesBreast Implant Evaluation - Narrativeopenlab.doisNo ratings yet
- Breast PainDocument9 pagesBreast PainmarysrbNo ratings yet
- American College of Radiology End User License AgreementDocument9 pagesAmerican College of Radiology End User License AgreementYori PrimandaNo ratings yet
- Abdominal Truama (Handout)Document6 pagesAbdominal Truama (Handout)Ayuub AbdirizakNo ratings yet
- Aaa RepairDocument5 pagesAaa RepairLakshmi Mounica GrandhiNo ratings yet
- Abdomen X RayDocument4 pagesAbdomen X RaytimvrghsNo ratings yet
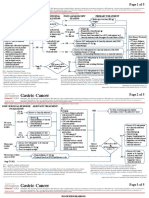
- Ca Treatment Gastric Web AlgorithmDocument5 pagesCa Treatment Gastric Web AlgorithmEVELYN EZEKWENo ratings yet
- Surgery E: MD Najmus Sakir K-75Document14 pagesSurgery E: MD Najmus Sakir K-75Kitty GraceNo ratings yet
- CA Treatment Osteosarcoma Pedi Web AlgorithmDocument6 pagesCA Treatment Osteosarcoma Pedi Web AlgorithmyaseenNo ratings yet
- Ca - Treatment-Breast-Inflammatory-Web-AlgorithmDocument19 pagesCa - Treatment-Breast-Inflammatory-Web-AlgorithmAgustin SierraNo ratings yet
- Diagnostic Imaging of Breast: Radiology DepartementDocument35 pagesDiagnostic Imaging of Breast: Radiology DepartementAnonymous 9NC74wAL1No ratings yet
- Blunt Abdominal TraumaDocument11 pagesBlunt Abdominal TraumaRahmat SyahiliNo ratings yet
- BUAP QAQ - Patient Outcome DataDocument2 pagesBUAP QAQ - Patient Outcome DataYousra ManaaNo ratings yet
- Cap-2 27 2015Document73 pagesCap-2 27 2015martyn odekeNo ratings yet
- Masa Palpable en MamaDocument22 pagesMasa Palpable en MamaarcaNo ratings yet
- D105 APBI Future - My Point of ViewDocument70 pagesD105 APBI Future - My Point of ViewSoc. Portuguesa de Radioterapia OncologiaNo ratings yet
- SBRT Upper AbdomenDocument25 pagesSBRT Upper AbdomenIPQ PioneerNo ratings yet
- ACR Criteria PDFDocument18 pagesACR Criteria PDFquickdannyNo ratings yet
- GEN SURG Module 4 Quiz 2 Samplexes 2011-2018: (Trauma)Document30 pagesGEN SURG Module 4 Quiz 2 Samplexes 2011-2018: (Trauma)Kaila AbeledaNo ratings yet
- Essentials of Ultrasound Course AssessmentDocument8 pagesEssentials of Ultrasound Course Assessmentaassmmaass13No ratings yet
- APBI Journal Club PowerPointDocument20 pagesAPBI Journal Club PowerPointRegan Ward HimeNo ratings yet
- History History History: CounsellingDocument2 pagesHistory History History: CounsellingMahad IbrahemNo ratings yet
- The Use of A Pediatric Abdominal Trauma Protocol Improves Resource UtilizationDocument26 pagesThe Use of A Pediatric Abdominal Trauma Protocol Improves Resource UtilizationArchanaNo ratings yet
- CT vs. Mri Compendium 2011 1 PDFDocument4 pagesCT vs. Mri Compendium 2011 1 PDFWaqas HaleemNo ratings yet
- Rationale Diagnostic ProceduresDocument22 pagesRationale Diagnostic ProceduresShaktisila FatrahadyNo ratings yet
- Algoritma Buat Bedah-1Document2 pagesAlgoritma Buat Bedah-1nilacindyNo ratings yet
- Curso - Volúmenes - ESTRO - Octubre - 2015 - Dra - ArenasDocument105 pagesCurso - Volúmenes - ESTRO - Octubre - 2015 - Dra - ArenasTriniNo ratings yet
- 04 Non Muscle Invasive BC - LR1Document17 pages04 Non Muscle Invasive BC - LR1alaaNo ratings yet
- PDFsam ObGynDocument4 pagesPDFsam ObGynAlessandro ZadraNo ratings yet
- Abdomen Blunt Trauma 2 - 3 - 2020Document6 pagesAbdomen Blunt Trauma 2 - 3 - 2020Iqra NazNo ratings yet
- Dr. Manoj GuptaDocument36 pagesDr. Manoj GuptaafshanNo ratings yet
- CT Scan in Abdominal Emergency SurgeryFrom EverandCT Scan in Abdominal Emergency SurgeryFausto CatenaNo ratings yet
- Siemens Setup ManualsDocument858 pagesSiemens Setup Manualsapi-2689284867% (9)
- Bone-RADS v2023 Assessment Categories Table - FinalDocument1 pageBone-RADS v2023 Assessment Categories Table - FinalBruna AngeloNo ratings yet
- Konica Minolta, Inc. Medium Term Business Plan: - Announced On May 9th, 2014Document27 pagesKonica Minolta, Inc. Medium Term Business Plan: - Announced On May 9th, 2014sidNo ratings yet
- CT of The Heart PDFDocument391 pagesCT of The Heart PDFZornić AlemNo ratings yet
- Heat Load Gupta Consultants & Associates: Lower BasementDocument2 pagesHeat Load Gupta Consultants & Associates: Lower BasementSameer UddinNo ratings yet
- Diagnostic Imaging Services Regulation 2012Document65 pagesDiagnostic Imaging Services Regulation 2012Aya MahmoudNo ratings yet
- DHR System User ManualDocument218 pagesDHR System User Manualselvamejia100% (1)
- PSC VACANT POSITIONS IN THE PUBLIC SERVICE 6th APRIL 2020Document9 pagesPSC VACANT POSITIONS IN THE PUBLIC SERVICE 6th APRIL 2020sharif sayyid al mahdalyNo ratings yet
- A Study On Employee Welfare Measures and Its Influence On Performance of Hindustan Latex LTD (HLL)Document76 pagesA Study On Employee Welfare Measures and Its Influence On Performance of Hindustan Latex LTD (HLL)suriyanarayanan707No ratings yet
- Evaluation and Management of Renal Injuries: Consensus Statement of The Renal Trauma SubcommitteeDocument18 pagesEvaluation and Management of Renal Injuries: Consensus Statement of The Renal Trauma SubcommitteeTakis StefanopoulosNo ratings yet
- A Compact Modified Antipodal Vivaldi Antenna For Imaging ApplicationDocument5 pagesA Compact Modified Antipodal Vivaldi Antenna For Imaging ApplicationHumza SamiNo ratings yet
- Atlas of Small Animal Diagnostic Imaging Nathan C Nelson Full ChapterDocument51 pagesAtlas of Small Animal Diagnostic Imaging Nathan C Nelson Full Chapterpatty.shawgo340100% (7)
- Al-Okshi Et Al 2016Document11 pagesAl-Okshi Et Al 2016Ayman AlOkshiNo ratings yet
- Synopsis For Breast CancerDocument50 pagesSynopsis For Breast Cancershuja behnaNo ratings yet
- Diagnostics 11 01219Document14 pagesDiagnostics 11 01219Jose Antonio Chavez MNo ratings yet
- Catalogo Catálogo Geral Quart 2903095428Document40 pagesCatalogo Catálogo Geral Quart 2903095428Tuankiet TruongNo ratings yet
- Medical Physis CareersDocument93 pagesMedical Physis CareersShakeel Ahmad KasuriNo ratings yet
- Presentations On Educational Bio-Medical Engineering Project For Trios CollegeDocument16 pagesPresentations On Educational Bio-Medical Engineering Project For Trios CollegeGUIDE ON BIO-MEDICAL ENGINEERING UNDERGRADUATE PROGRAM:50% (2)
- Maxim in IndiaDocument19 pagesMaxim in IndiaSuryansh SinghNo ratings yet
- Best Diagnostic Center in Gurgaon Tests Cost HODDocument1 pageBest Diagnostic Center in Gurgaon Tests Cost HODyashpalwalNo ratings yet
- CT Image Quality: Outsource, Inc. (All Rights Reserved)Document44 pagesCT Image Quality: Outsource, Inc. (All Rights Reserved)bbkanilNo ratings yet
- 2020 Selected Occupational Therapy CPT CodesDocument5 pages2020 Selected Occupational Therapy CPT CodesJane DNo ratings yet
- Imaging of Normal SpineDocument32 pagesImaging of Normal SpineDestia AnandaNo ratings yet
- 主流几大SPECT-CT 制造商系统参数比较Document6 pages主流几大SPECT-CT 制造商系统参数比较AnguschowNo ratings yet
- Medical SpecialistsDocument2 pagesMedical SpecialistsArvin Dela CrÜzNo ratings yet
- Introdution To Biomedical EngineeringDocument28 pagesIntrodution To Biomedical Engineeringsidkhan1100% (1)
- Adams and Stashaks Lameness in Horses Seventh Edition Edition Gary M Baxter Full ChapterDocument67 pagesAdams and Stashaks Lameness in Horses Seventh Edition Edition Gary M Baxter Full Chapterhobert.gardner896100% (4)
- Breast Imaging Survey FormDocument6 pagesBreast Imaging Survey Formmaryam cookNo ratings yet