Download as pdf or txt
You might also like
- SIBODocument146 pagesSIBOMundhir Al-Khusaibi82% (11)
- Case Study Liver CirrhosisDocument30 pagesCase Study Liver CirrhosisMarielle Soriano100% (3)
- Regulation of Gastric SecretionDocument18 pagesRegulation of Gastric SecretionSanchit Rao50% (2)
- Successful Surgical Management of An Extrahepatic Biliary CystadenocarcinomaDocument4 pagesSuccessful Surgical Management of An Extrahepatic Biliary CystadenocarcinomaVlad IchimNo ratings yet
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinNo ratings yet
- Ninomiya 等 - 2020 - Clip on Staple Method to Prevent Bile Leakage in ADocument4 pagesNinomiya 等 - 2020 - Clip on Staple Method to Prevent Bile Leakage in A蔡一鹏No ratings yet
- Dynamic CT Findings of A Polypoid Gastric - ChrisnaDocument4 pagesDynamic CT Findings of A Polypoid Gastric - ChrisnaferonicaNo ratings yet
- Acute Median Arcuate Ligament Syndrome After PancreaticoduodenectomyDocument5 pagesAcute Median Arcuate Ligament Syndrome After PancreaticoduodenectomyAna Karen RNo ratings yet
- Z - 2001-01 - Nonfunctioning Islet Cell Carcinoma of The Pancreas Associated With Massive Intra-Abdominal HemorrhageDocument5 pagesZ - 2001-01 - Nonfunctioning Islet Cell Carcinoma of The Pancreas Associated With Massive Intra-Abdominal HemorrhageNawzad SulayvaniNo ratings yet
- ccr3 2368Document6 pagesccr3 2368Avicenna Shafhan ArfiNo ratings yet
- J Gastrointest Cancer 2019 50 3 578-82Document5 pagesJ Gastrointest Cancer 2019 50 3 578-82Fernando SousaNo ratings yet
- FA - Adrenal Mets Artice - PJMS-32-1044Document3 pagesFA - Adrenal Mets Artice - PJMS-32-1044Farhat AbbasNo ratings yet
- 8593 29933 3 PBDocument4 pages8593 29933 3 PBDiogo SantosNo ratings yet
- Obstructive Jaundice A Clinical StudyDocument7 pagesObstructive Jaundice A Clinical StudyAnisah Maryam DianahNo ratings yet
- Gastroduodenal Artery Pseudoaneurysm and Aberrant Right Hepatic ArteryDocument3 pagesGastroduodenal Artery Pseudoaneurysm and Aberrant Right Hepatic ArteryGordana PuzovicNo ratings yet
- Laparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaDocument4 pagesLaparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaRonald QuezadaNo ratings yet
- Urology Case Reports: OncologyDocument3 pagesUrology Case Reports: OncologyDavids MarinNo ratings yet
- Multiple Hepatic Sclerosing HemangiomaDocument4 pagesMultiple Hepatic Sclerosing Hemangiomahussein_faourNo ratings yet
- Kumar 2013Document4 pagesKumar 2013Cirugía General Hospital de San JoséNo ratings yet
- Klatskin TumorDocument9 pagesKlatskin TumorFlorian JeffNo ratings yet
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Medi 98 E14234Document5 pagesMedi 98 E14234فرجني موغNo ratings yet
- Totally Laparoscipic Right Colectomy: Technique Description: Hepato-Gastroenterology April 2015Document5 pagesTotally Laparoscipic Right Colectomy: Technique Description: Hepato-Gastroenterology April 2015anatomNo ratings yet
- International Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. AwasthiDocument3 pagesInternational Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. Awasthijohanna monsalveNo ratings yet
- Choledochal Cyst: SymposiumDocument3 pagesCholedochal Cyst: SymposiumRegi Anastasya MangiriNo ratings yet
- Materi DR Budi WidodoDocument44 pagesMateri DR Budi WidodoAnna Maria UlfaNo ratings yet
- COLONDocument24 pagesCOLONYS NateNo ratings yet
- HPB 2016, 18 (S1), E1 Ee384Document2 pagesHPB 2016, 18 (S1), E1 Ee384Yacine Tarik AizelNo ratings yet
- Surgtest GI Surgery NEET SS 2022 RecallDocument58 pagesSurgtest GI Surgery NEET SS 2022 RecallRajhan 410No ratings yet
- Classi Fication of Biliary Tract Cancers Established by The Japanese Society of Hepato-Biliary-Pancreatic Surgery: 3 English EditionDocument16 pagesClassi Fication of Biliary Tract Cancers Established by The Japanese Society of Hepato-Biliary-Pancreatic Surgery: 3 English EditionMoez SahnounNo ratings yet
- Jurnal 7Document3 pagesJurnal 7rahayuNo ratings yet
- Spontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewDocument5 pagesSpontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewHitomi-No ratings yet
- Anatomical Laparoscopic Right Posterior SectionectomyDocument7 pagesAnatomical Laparoscopic Right Posterior SectionectomyhoangducnamNo ratings yet
- Articulo 1 Quiste ColeDocument4 pagesArticulo 1 Quiste ColeMaria Elena VinuezaNo ratings yet
- Oesophagocoloplasty For Corrosive Oesophageal Stricture: AbstractDocument12 pagesOesophagocoloplasty For Corrosive Oesophageal Stricture: AbstractSpandan KadamNo ratings yet
- Presentation of Unruptured Right Gastric Aneurysm Du 2024 International JourDocument4 pagesPresentation of Unruptured Right Gastric Aneurysm Du 2024 International JourRonald QuezadaNo ratings yet
- RJX 102Document3 pagesRJX 102FachryNo ratings yet
- Case ReportDocument5 pagesCase Report260778No ratings yet
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocument1 pageLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiNo ratings yet
- Hilar Cholangiocarcinoma Diagnosed and Treated Early, in Prejaundice PhaseDocument4 pagesHilar Cholangiocarcinoma Diagnosed and Treated Early, in Prejaundice PhasebbdddNo ratings yet
- Absite 21 Answers - StomachDocument2 pagesAbsite 21 Answers - Stomachsiriopa08No ratings yet
- Biliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentDocument3 pagesBiliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentMarcelo CalossoNo ratings yet
- Laparoscopic Right Radical Hemicolectomy: Howidoit?Document4 pagesLaparoscopic Right Radical Hemicolectomy: Howidoit?pingusNo ratings yet
- En Bloc Robot-Assisted Laparoscopic Partial Cystectomy, Urachal Resection, and Pelvic Lymphadenectomy For Urachal AdenocarcinomaDocument4 pagesEn Bloc Robot-Assisted Laparoscopic Partial Cystectomy, Urachal Resection, and Pelvic Lymphadenectomy For Urachal Adenocarcinomadr.tonichenNo ratings yet
- DIANDRA PARIKESIT Thrombus-Like - Tumor - of - Renal - Cell - Carcinoma - MimickDocument4 pagesDIANDRA PARIKESIT Thrombus-Like - Tumor - of - Renal - Cell - Carcinoma - MimickYulia DjatiwardaniNo ratings yet
- Journal of Medical Case Reports: Jejuno-Jejunal Invagination Caused by Epithelioid Sarcoma: A CaseDocument4 pagesJournal of Medical Case Reports: Jejuno-Jejunal Invagination Caused by Epithelioid Sarcoma: A CaseAde CandraNo ratings yet
- Art 4 - Haemorrhagic Rupture of Hepatocellular CarcinomaDocument3 pagesArt 4 - Haemorrhagic Rupture of Hepatocellular CarcinomaBertrand EssobiyouNo ratings yet
- Rcsann 2020 0149Document7 pagesRcsann 2020 0149NandaNo ratings yet
- Successful Cervical Esophageal Reconstruction Using Gastric Conduit Without Gastroepiploic ArteryDocument2 pagesSuccessful Cervical Esophageal Reconstruction Using Gastric Conduit Without Gastroepiploic ArteryRony RonyNo ratings yet
- Ameboma of Colon Simulating Colonic Adenocarcinoma: Case ReportDocument3 pagesAmeboma of Colon Simulating Colonic Adenocarcinoma: Case ReportJulio BarajasNo ratings yet
- A Rare Case of Spontaneous Hepatic Rupture in A Pregnant WomanDocument4 pagesA Rare Case of Spontaneous Hepatic Rupture in A Pregnant WomanFatmawati MahirNo ratings yet
- D2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologyDocument66 pagesD2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologySuneel Kaushik KNo ratings yet
- Biloma After Cholecystectomy 2Document5 pagesBiloma After Cholecystectomy 2Rashid LatifNo ratings yet
- Liver DiseasesDocument12 pagesLiver Diseasesissam_1994No ratings yet
- Jurnal IkterusDocument3 pagesJurnal IkterusTututWidyaNurAnggrainiNo ratings yet
- It Is Not Always A Cholangiocarcinoma: Unusual Peritoneal Carcinomatosis Revealing Gastric AdenocarcinomaDocument5 pagesIt Is Not Always A Cholangiocarcinoma: Unusual Peritoneal Carcinomatosis Revealing Gastric AdenocarcinomaIJAR JOURNALNo ratings yet
- A Case Report of Liver Infiltration From A Large - 2024 - International JournalDocument4 pagesA Case Report of Liver Infiltration From A Large - 2024 - International JournalRonald QuezadaNo ratings yet
- Hydatic Cyst of The Liver or Hepatic Mucinous CystadenomaDocument5 pagesHydatic Cyst of The Liver or Hepatic Mucinous CystadenomaIJAR JOURNALNo ratings yet
- Mrcs HepatobiliaryDocument40 pagesMrcs HepatobiliaryAdebisiNo ratings yet
- Surgical Management Ca Colon 1Document81 pagesSurgical Management Ca Colon 1Shweta Achuthan KuttyNo ratings yet
- 4206 CR 1Document3 pages4206 CR 1Ardianto SucintaNo ratings yet
- Rupture of A Hydatid Cyst Into The Bile DuctDocument3 pagesRupture of A Hydatid Cyst Into The Bile DuctasclepiuspdfsNo ratings yet
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesFrom EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo ratings yet
- Comparison of Trans Anal Endoscopic Operation and TR - 2017 - Annals of MedicineDocument7 pagesComparison of Trans Anal Endoscopic Operation and TR - 2017 - Annals of MedicineViorel AvramescuNo ratings yet
- Škoda Superb An 2017 #2.0TDI DSG #Tva Deductibila #GARANTIE #COLUMBUS Bucuresti Sectorul 1 - OLXDocument7 pagesŠkoda Superb An 2017 #2.0TDI DSG #Tva Deductibila #GARANTIE #COLUMBUS Bucuresti Sectorul 1 - OLXViorel AvramescuNo ratings yet
- Lexical Combinations Via FormulaDocument6 pagesLexical Combinations Via FormulaViorel AvramescuNo ratings yet
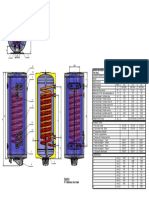
- 56 100-150 T21 Vertikalni Za Stena ENDocument1 page56 100-150 T21 Vertikalni Za Stena ENViorel AvramescuNo ratings yet
- MS P2 CompilationDocument451 pagesMS P2 CompilationJe KirsteneNo ratings yet
- Definiciones en El Marco de Trabajo Del IDDSI de Líquidos y SólidosDocument20 pagesDefiniciones en El Marco de Trabajo Del IDDSI de Líquidos y SólidosLaura IzquierdoNo ratings yet
- Inflammatory Bowel DiseaseDocument412 pagesInflammatory Bowel DiseaseSabbra CadabraNo ratings yet
- Powerpoint: Colorectal Surgical DiseasesDocument74 pagesPowerpoint: Colorectal Surgical Diseasesj.doe.hex_87100% (1)
- Medical Surgical NursingDocument6 pagesMedical Surgical NursingMariel Febreo MerlanNo ratings yet
- Intussusception 161007042729 PDFDocument44 pagesIntussusception 161007042729 PDFDina MarselinaNo ratings yet
- Ch. Danis:3 Month:Invaginasi:Dr. Tedjo Arianto, SP.B-KBDDocument11 pagesCh. Danis:3 Month:Invaginasi:Dr. Tedjo Arianto, SP.B-KBDNhoeExanisahNo ratings yet
- IntussusceptionDocument8 pagesIntussusceptionMohamed Na3eemNo ratings yet
- Clasificacion de Hannover PDFDocument11 pagesClasificacion de Hannover PDFMelaine ChirinosNo ratings yet
- Esophageal and Gastric Disorders in Infancy and ChildhoodDocument1,461 pagesEsophageal and Gastric Disorders in Infancy and ChildhoodVu HoangNo ratings yet
- Colcistectomia FenestradaDocument8 pagesColcistectomia FenestradaLuis David AguileraNo ratings yet
- Amoebiasis - and GiardiasisDocument59 pagesAmoebiasis - and GiardiasisSaurabh AgarwalNo ratings yet
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- Refractory Gastroesophageal Reflux Disease Diagnosis and ManagementDocument12 pagesRefractory Gastroesophageal Reflux Disease Diagnosis and Managementg-46005995No ratings yet
- Cleanse & Restore Kit and ProtocolDocument2 pagesCleanse & Restore Kit and ProtocolEmese MagdásNo ratings yet
- Tabel SubstanţeDocument2 pagesTabel SubstanţeDosa DanielNo ratings yet
- Barium StudiesDocument16 pagesBarium StudiesRuby Dela RamaNo ratings yet
- Allen: Pre-Medical: BiologyDocument1 pageAllen: Pre-Medical: BiologyDevdatta PatilNo ratings yet
- BETTY M - Pharmacology 1. Ass 2Document3 pagesBETTY M - Pharmacology 1. Ass 2Tapiwa KugodaNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: © 2017 John Wiley & Sons LTDDocument6 pagesIntestinal Tuberculosis: A Diagnostic Challenge: © 2017 John Wiley & Sons LTDLily SmithNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- Physiology: Stomach by DR Anam IsrarDocument20 pagesPhysiology: Stomach by DR Anam IsrarSaher Yasin100% (1)
- Physio Cont.Document22 pagesPhysio Cont.Ayman HajeerNo ratings yet
- Acute AbdomenDocument72 pagesAcute AbdomenIgnasNo ratings yet
- Salmonella LectureDocument21 pagesSalmonella Lectureghosson01006228961No ratings yet
- Chapter 39 - Lower Digestive Tract DisordersDocument5 pagesChapter 39 - Lower Digestive Tract DisordersStacey100% (1)
- Git 5 PDFDocument27 pagesGit 5 PDFafaq alismailiNo ratings yet