
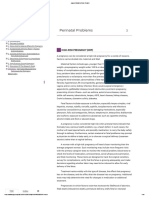
Prenatal Postpartum Care
Prenatal Postpartum Care
You might also like
- History Taking of The NewbornDocument9 pagesHistory Taking of The NewbornRAPHAEL ALFREDO LUIS BUENAFENo ratings yet
- Antenatal Care Lesson PlanDocument17 pagesAntenatal Care Lesson PlanAnuradha Maurya81% (16)
- Antenatal Care: By: Dr. Addis GDocument40 pagesAntenatal Care: By: Dr. Addis GtareNo ratings yet
- Edited Book 1Document501 pagesEdited Book 1mkm050923No ratings yet
- Prenatal CareDocument43 pagesPrenatal CareClare Espiritu DucutNo ratings yet
- Antenatal Assessment of Foetal Wellbeing.Document30 pagesAntenatal Assessment of Foetal Wellbeing.Kavya S MohanNo ratings yet
- Intrauterinegrowth RestrictionDocument48 pagesIntrauterinegrowth Restrictionshyam792No ratings yet
- Maternal Health ServicesDocument42 pagesMaternal Health ServicesAbo AmgadNo ratings yet
- Antenatal Case - Jonathan Matthews - November 2013Document25 pagesAntenatal Case - Jonathan Matthews - November 2013Anusree AnusreervNo ratings yet
- Assessment of Fetal Well BeingDocument90 pagesAssessment of Fetal Well BeingSherlinNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- IUGRDocument35 pagesIUGROlesea Morari CusnirNo ratings yet
- Big For Date Uterus - SeminarDocument56 pagesBig For Date Uterus - Seminarahmed mohammedNo ratings yet
- Induction of LaborDocument8 pagesInduction of LaborwiwimbakNo ratings yet
- Dispropositionate Fetal Growth 2020Document52 pagesDispropositionate Fetal Growth 2020Austine OdhiamboNo ratings yet
- D. High Risk PregnanciesDocument78 pagesD. High Risk PregnanciesKeziah TampusNo ratings yet
- NCM 109 ReviewerDocument6 pagesNCM 109 ReviewerDiane IlaoNo ratings yet
- NCM 109 SL Lesson 1Document3 pagesNCM 109 SL Lesson 1Martina Medrano100% (1)
- Tumaob, Lealyn A. Group HDocument4 pagesTumaob, Lealyn A. Group H002No ratings yet
- CH 19 Fetal Assessment NotesDocument7 pagesCH 19 Fetal Assessment NotesMary LowryNo ratings yet
- Intrahepatic Cholestasis of PregnancyDocument19 pagesIntrahepatic Cholestasis of Pregnancyjeribob1823No ratings yet
- Intrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSDocument72 pagesIntrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSapi-3703352No ratings yet
- Case Stud1.editedDocument12 pagesCase Stud1.editedNahshon UnsimilarNo ratings yet
- AbortoDocument26 pagesAbortoLeyda AvilésNo ratings yet
- Protocol Book For OBGYNDocument41 pagesProtocol Book For OBGYNShabir BadakhshNo ratings yet
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthEula ReyesNo ratings yet
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthClouiseNo ratings yet
- The High Risk Prenatal ClientDocument46 pagesThe High Risk Prenatal ClientPaul Albert Agunod100% (2)
- Antenatal CareDocument29 pagesAntenatal Careعبدالكريم الاسدNo ratings yet
- Jurnal OSP OkDocument26 pagesJurnal OSP OkOctaria SaputraNo ratings yet
- Resumenes GPCDocument41 pagesResumenes GPCmp 27No ratings yet
- Lecture IV IIIDocument32 pagesLecture IV IIIMohamad Alsayed AlasaasNo ratings yet
- Antenatal AssessmentDocument40 pagesAntenatal AssessmentKailash NagarNo ratings yet
- Drug Use During Pregnancy and LactationDocument50 pagesDrug Use During Pregnancy and LactationchintyamontangNo ratings yet
- Antenatal Care &assessment ofDocument39 pagesAntenatal Care &assessment ofxj74fr4ddxNo ratings yet
- Prenatal Care - Module A: NUR 106 Spring, 2005Document100 pagesPrenatal Care - Module A: NUR 106 Spring, 2005herwin sulemanNo ratings yet
- Assessment & Screening of High Risk PregnancyDocument18 pagesAssessment & Screening of High Risk Pregnancypiub15420No ratings yet
- Antenatal Care and High Risk PregnancyDocument12 pagesAntenatal Care and High Risk PregnancyMadhu Sudhan PandeyaNo ratings yet
- Preterm LabourDocument3 pagesPreterm Labourcgao30No ratings yet
- Prenatal Genetic Screening DBiagnosis Hamamy 2010Document27 pagesPrenatal Genetic Screening DBiagnosis Hamamy 2010Georgie StephenNo ratings yet
- Highrisk AssessmentDocument23 pagesHighrisk AssessmentHaripriya RadhikaNo ratings yet
- Topic 1 Maternal and Fetal Patient AssessmentDocument14 pagesTopic 1 Maternal and Fetal Patient AssessmentLenard SakiliNo ratings yet
- Perinatal Problems: High-Risk Pregnancy (HRP)Document16 pagesPerinatal Problems: High-Risk Pregnancy (HRP)anuNo ratings yet
- Psychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryDocument6 pagesPsychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryKimberly Sharah Mae Fortuno100% (1)
- Assessment of Fetal WellbeingDocument47 pagesAssessment of Fetal WellbeingsukiyamakotoNo ratings yet
- ANC SreelakshmiDocument22 pagesANC SreelakshmiEmyNo ratings yet
- Periconceptional and Antenatal CareDocument2 pagesPericonceptional and Antenatal CareYavani KulasinghamNo ratings yet
- Guideline For Routine Prenatal and Perinatal CareDocument6 pagesGuideline For Routine Prenatal and Perinatal CareAnnisa RahmawatiNo ratings yet
- Diagnostic TestDocument5 pagesDiagnostic TestCielo Alyssa IglianeNo ratings yet
- Antenatal AssessmentDocument40 pagesAntenatal Assessmentmanjuvm91% (11)
- Abortion, Ectopic PregnancyDocument139 pagesAbortion, Ectopic PregnancyINFORMASI MENARIKNo ratings yet
- 3rd TrimesterDocument37 pages3rd TrimesterAparna MohanNo ratings yet
- Antenatal AssessmentDocument46 pagesAntenatal AssessmentmariaNo ratings yet
- Genetic Screening and Prenatal DiagnosisDocument36 pagesGenetic Screening and Prenatal DiagnosisSarafina ChingaNo ratings yet
- Fetal-Growth DisorderS Fetal DisordersDocument29 pagesFetal-Growth DisorderS Fetal DisordersLakshay GulatiNo ratings yet
- Premature Rupture of MembranesDocument33 pagesPremature Rupture of MembranesSarang Lee100% (1)
- Premature Rupture of The MembraneDocument27 pagesPremature Rupture of The MembranezizsatriaNo ratings yet
- Multiple PregnancyDocument16 pagesMultiple Pregnancyjane7arian7berzabalNo ratings yet
- Anatomy & Conception: Ns - Wulan Novika Ambarsari.,MANDocument100 pagesAnatomy & Conception: Ns - Wulan Novika Ambarsari.,MANdikaNo ratings yet
- FibroidsFrom EverandFibroidsJames H. SegarsNo ratings yet
- Left-Broken-17 BruisedDocument6 pagesLeft-Broken-17 BruisedJamie PalmeriNo ratings yet
- Nutrition and Supplementation PDF FreeDocument35 pagesNutrition and Supplementation PDF FreeJamie PalmeriNo ratings yet
- (Intubate!) : Stag e Description GFR (Ml/min/1.73Document7 pages(Intubate!) : Stag e Description GFR (Ml/min/1.73Jamie PalmeriNo ratings yet
- Anticoagulant Oral GuidelinesforprescribingmonitoringandmanagementDocument29 pagesAnticoagulant Oral GuidelinesforprescribingmonitoringandmanagementJamie PalmeriNo ratings yet
- MeningiomaDocument31 pagesMeningiomaJamie PalmeriNo ratings yet
- Antenatal Care Unit Two Lesson 192Document192 pagesAntenatal Care Unit Two Lesson 192RidiculouslySweetNo ratings yet
- WHO. Fatherhood and Health Outcomes in EuropeDocument40 pagesWHO. Fatherhood and Health Outcomes in EuropeMaria Carmela DomocmatNo ratings yet
- Nepal PosterDocument1 pageNepal Posterapi-282838160No ratings yet
- Cavite State University: Cvsu Vision Cvsu MissionDocument31 pagesCavite State University: Cvsu Vision Cvsu MissionToyour EternityNo ratings yet
- Anaemia in Pregnancy Study PDFDocument189 pagesAnaemia in Pregnancy Study PDFMurugesan100% (4)
- First Prenatal VisitDocument7 pagesFirst Prenatal VisitAnonymous lSLAlEBjVCNo ratings yet
- Antenatal CareDocument3 pagesAntenatal CareAnnapurna DangetiNo ratings yet
- Kujdesi Antenatal - Anglisht (Per Web) 02Document53 pagesKujdesi Antenatal - Anglisht (Per Web) 02UNICEF KosovoNo ratings yet
- Guideline Book 2017Document204 pagesGuideline Book 2017tonirian99No ratings yet
- Models of Maternal HealthDocument12 pagesModels of Maternal HealthLindsey Brock MoralesNo ratings yet
- Preventive Obstetrics (By Mohan.s)Document52 pagesPreventive Obstetrics (By Mohan.s)mOHAN.S98% (55)
- Drugs Used in PregnancyDocument11 pagesDrugs Used in PregnancyTasmia RhamanNo ratings yet
- Antenatal Care During The First, SecondDocument85 pagesAntenatal Care During The First, Secondasmina sihotang100% (1)
- EMBU UNIVERSITY Rules and RegulationsDocument16 pagesEMBU UNIVERSITY Rules and Regulationsjeff liwaliNo ratings yet
- Prenatal Care: James E. Eullaran Katrina Ysabelle Garcia Kathleen Mae R. Flores April 16, 2019Document99 pagesPrenatal Care: James E. Eullaran Katrina Ysabelle Garcia Kathleen Mae R. Flores April 16, 2019James eullaranNo ratings yet
- An Essay About MotherDocument6 pagesAn Essay About Motherzzcpllaeg100% (2)
- Literature ReviewDocument4 pagesLiterature ReviewSonam ChodenNo ratings yet
- Project On Analysis of Attitude of Pregnant Mother Towards Antenatal Care ServiceDocument50 pagesProject On Analysis of Attitude of Pregnant Mother Towards Antenatal Care ServiceYUSUF AMINUNo ratings yet
- Lupus Case PresentationDocument48 pagesLupus Case PresentationRoscelie KhoNo ratings yet
- Project Documentation Thesis BookDocument66 pagesProject Documentation Thesis BookMAHER MOHAMEDNo ratings yet
- Antenatal CareDocument3 pagesAntenatal CareSimranNo ratings yet
- 5 - Care of The Mother and The FetusDocument36 pages5 - Care of The Mother and The FetusMa Nelia P MagsinoNo ratings yet
- Kalusugan ReflectionDocument3 pagesKalusugan ReflectionRizza Mae CallejaNo ratings yet
- Antenatal CareDocument19 pagesAntenatal CareIshika RoyNo ratings yet
- Prenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncDocument33 pagesPrenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncISFAHAN MASULOTNo ratings yet
- Teenage PregnancyDocument4 pagesTeenage PregnancyjoannesalagubangNo ratings yet
- N E E D S C O G N I T I V E P E R P E T U A L RationaleDocument14 pagesN E E D S C O G N I T I V E P E R P E T U A L RationaleArianna Jasmine MabungaNo ratings yet
- Innovative Approaches For Improving Maternal and Newborn Health - A Landscape AnalysisDocument19 pagesInnovative Approaches For Improving Maternal and Newborn Health - A Landscape AnalysisAli Abubakar AuduNo ratings yet
- Alignment of Performance Based Financing in Health With The Government Budget A Principle Based ApproachDocument42 pagesAlignment of Performance Based Financing in Health With The Government Budget A Principle Based ApproachCandra, MPHNo ratings yet





























































































Download as pdf or txt
You might also like
- History Taking of The NewbornDocument9 pagesHistory Taking of The NewbornRAPHAEL ALFREDO LUIS BUENAFENo ratings yet
- Antenatal Care Lesson PlanDocument17 pagesAntenatal Care Lesson PlanAnuradha Maurya81% (16)
- Antenatal Care: By: Dr. Addis GDocument40 pagesAntenatal Care: By: Dr. Addis GtareNo ratings yet
- Edited Book 1Document501 pagesEdited Book 1mkm050923No ratings yet
- Prenatal CareDocument43 pagesPrenatal CareClare Espiritu DucutNo ratings yet
- Antenatal Assessment of Foetal Wellbeing.Document30 pagesAntenatal Assessment of Foetal Wellbeing.Kavya S MohanNo ratings yet
- Intrauterinegrowth RestrictionDocument48 pagesIntrauterinegrowth Restrictionshyam792No ratings yet
- Maternal Health ServicesDocument42 pagesMaternal Health ServicesAbo AmgadNo ratings yet
- Antenatal Case - Jonathan Matthews - November 2013Document25 pagesAntenatal Case - Jonathan Matthews - November 2013Anusree AnusreervNo ratings yet
- Assessment of Fetal Well BeingDocument90 pagesAssessment of Fetal Well BeingSherlinNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- IUGRDocument35 pagesIUGROlesea Morari CusnirNo ratings yet
- Big For Date Uterus - SeminarDocument56 pagesBig For Date Uterus - Seminarahmed mohammedNo ratings yet
- Induction of LaborDocument8 pagesInduction of LaborwiwimbakNo ratings yet
- Dispropositionate Fetal Growth 2020Document52 pagesDispropositionate Fetal Growth 2020Austine OdhiamboNo ratings yet
- D. High Risk PregnanciesDocument78 pagesD. High Risk PregnanciesKeziah TampusNo ratings yet
- NCM 109 ReviewerDocument6 pagesNCM 109 ReviewerDiane IlaoNo ratings yet
- NCM 109 SL Lesson 1Document3 pagesNCM 109 SL Lesson 1Martina Medrano100% (1)
- Tumaob, Lealyn A. Group HDocument4 pagesTumaob, Lealyn A. Group H002No ratings yet
- CH 19 Fetal Assessment NotesDocument7 pagesCH 19 Fetal Assessment NotesMary LowryNo ratings yet
- Intrahepatic Cholestasis of PregnancyDocument19 pagesIntrahepatic Cholestasis of Pregnancyjeribob1823No ratings yet
- Intrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSDocument72 pagesIntrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSapi-3703352No ratings yet
- Case Stud1.editedDocument12 pagesCase Stud1.editedNahshon UnsimilarNo ratings yet
- AbortoDocument26 pagesAbortoLeyda AvilésNo ratings yet
- Protocol Book For OBGYNDocument41 pagesProtocol Book For OBGYNShabir BadakhshNo ratings yet
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthEula ReyesNo ratings yet
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthClouiseNo ratings yet
- The High Risk Prenatal ClientDocument46 pagesThe High Risk Prenatal ClientPaul Albert Agunod100% (2)
- Antenatal CareDocument29 pagesAntenatal Careعبدالكريم الاسدNo ratings yet
- Jurnal OSP OkDocument26 pagesJurnal OSP OkOctaria SaputraNo ratings yet
- Resumenes GPCDocument41 pagesResumenes GPCmp 27No ratings yet
- Lecture IV IIIDocument32 pagesLecture IV IIIMohamad Alsayed AlasaasNo ratings yet
- Antenatal AssessmentDocument40 pagesAntenatal AssessmentKailash NagarNo ratings yet
- Drug Use During Pregnancy and LactationDocument50 pagesDrug Use During Pregnancy and LactationchintyamontangNo ratings yet
- Antenatal Care &assessment ofDocument39 pagesAntenatal Care &assessment ofxj74fr4ddxNo ratings yet
- Prenatal Care - Module A: NUR 106 Spring, 2005Document100 pagesPrenatal Care - Module A: NUR 106 Spring, 2005herwin sulemanNo ratings yet
- Assessment & Screening of High Risk PregnancyDocument18 pagesAssessment & Screening of High Risk Pregnancypiub15420No ratings yet
- Antenatal Care and High Risk PregnancyDocument12 pagesAntenatal Care and High Risk PregnancyMadhu Sudhan PandeyaNo ratings yet
- Preterm LabourDocument3 pagesPreterm Labourcgao30No ratings yet
- Prenatal Genetic Screening DBiagnosis Hamamy 2010Document27 pagesPrenatal Genetic Screening DBiagnosis Hamamy 2010Georgie StephenNo ratings yet
- Highrisk AssessmentDocument23 pagesHighrisk AssessmentHaripriya RadhikaNo ratings yet
- Topic 1 Maternal and Fetal Patient AssessmentDocument14 pagesTopic 1 Maternal and Fetal Patient AssessmentLenard SakiliNo ratings yet
- Perinatal Problems: High-Risk Pregnancy (HRP)Document16 pagesPerinatal Problems: High-Risk Pregnancy (HRP)anuNo ratings yet
- Psychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryDocument6 pagesPsychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryKimberly Sharah Mae Fortuno100% (1)
- Assessment of Fetal WellbeingDocument47 pagesAssessment of Fetal WellbeingsukiyamakotoNo ratings yet
- ANC SreelakshmiDocument22 pagesANC SreelakshmiEmyNo ratings yet
- Periconceptional and Antenatal CareDocument2 pagesPericonceptional and Antenatal CareYavani KulasinghamNo ratings yet
- Guideline For Routine Prenatal and Perinatal CareDocument6 pagesGuideline For Routine Prenatal and Perinatal CareAnnisa RahmawatiNo ratings yet
- Diagnostic TestDocument5 pagesDiagnostic TestCielo Alyssa IglianeNo ratings yet
- Antenatal AssessmentDocument40 pagesAntenatal Assessmentmanjuvm91% (11)
- Abortion, Ectopic PregnancyDocument139 pagesAbortion, Ectopic PregnancyINFORMASI MENARIKNo ratings yet
- 3rd TrimesterDocument37 pages3rd TrimesterAparna MohanNo ratings yet
- Antenatal AssessmentDocument46 pagesAntenatal AssessmentmariaNo ratings yet
- Genetic Screening and Prenatal DiagnosisDocument36 pagesGenetic Screening and Prenatal DiagnosisSarafina ChingaNo ratings yet
- Fetal-Growth DisorderS Fetal DisordersDocument29 pagesFetal-Growth DisorderS Fetal DisordersLakshay GulatiNo ratings yet
- Premature Rupture of MembranesDocument33 pagesPremature Rupture of MembranesSarang Lee100% (1)
- Premature Rupture of The MembraneDocument27 pagesPremature Rupture of The MembranezizsatriaNo ratings yet
- Multiple PregnancyDocument16 pagesMultiple Pregnancyjane7arian7berzabalNo ratings yet
- Anatomy & Conception: Ns - Wulan Novika Ambarsari.,MANDocument100 pagesAnatomy & Conception: Ns - Wulan Novika Ambarsari.,MANdikaNo ratings yet
- FibroidsFrom EverandFibroidsJames H. SegarsNo ratings yet
- Left-Broken-17 BruisedDocument6 pagesLeft-Broken-17 BruisedJamie PalmeriNo ratings yet
- Nutrition and Supplementation PDF FreeDocument35 pagesNutrition and Supplementation PDF FreeJamie PalmeriNo ratings yet
- (Intubate!) : Stag e Description GFR (Ml/min/1.73Document7 pages(Intubate!) : Stag e Description GFR (Ml/min/1.73Jamie PalmeriNo ratings yet
- Anticoagulant Oral GuidelinesforprescribingmonitoringandmanagementDocument29 pagesAnticoagulant Oral GuidelinesforprescribingmonitoringandmanagementJamie PalmeriNo ratings yet
- MeningiomaDocument31 pagesMeningiomaJamie PalmeriNo ratings yet
- Antenatal Care Unit Two Lesson 192Document192 pagesAntenatal Care Unit Two Lesson 192RidiculouslySweetNo ratings yet
- WHO. Fatherhood and Health Outcomes in EuropeDocument40 pagesWHO. Fatherhood and Health Outcomes in EuropeMaria Carmela DomocmatNo ratings yet
- Nepal PosterDocument1 pageNepal Posterapi-282838160No ratings yet
- Cavite State University: Cvsu Vision Cvsu MissionDocument31 pagesCavite State University: Cvsu Vision Cvsu MissionToyour EternityNo ratings yet
- Anaemia in Pregnancy Study PDFDocument189 pagesAnaemia in Pregnancy Study PDFMurugesan100% (4)
- First Prenatal VisitDocument7 pagesFirst Prenatal VisitAnonymous lSLAlEBjVCNo ratings yet
- Antenatal CareDocument3 pagesAntenatal CareAnnapurna DangetiNo ratings yet
- Kujdesi Antenatal - Anglisht (Per Web) 02Document53 pagesKujdesi Antenatal - Anglisht (Per Web) 02UNICEF KosovoNo ratings yet
- Guideline Book 2017Document204 pagesGuideline Book 2017tonirian99No ratings yet
- Models of Maternal HealthDocument12 pagesModels of Maternal HealthLindsey Brock MoralesNo ratings yet
- Preventive Obstetrics (By Mohan.s)Document52 pagesPreventive Obstetrics (By Mohan.s)mOHAN.S98% (55)
- Drugs Used in PregnancyDocument11 pagesDrugs Used in PregnancyTasmia RhamanNo ratings yet
- Antenatal Care During The First, SecondDocument85 pagesAntenatal Care During The First, Secondasmina sihotang100% (1)
- EMBU UNIVERSITY Rules and RegulationsDocument16 pagesEMBU UNIVERSITY Rules and Regulationsjeff liwaliNo ratings yet
- Prenatal Care: James E. Eullaran Katrina Ysabelle Garcia Kathleen Mae R. Flores April 16, 2019Document99 pagesPrenatal Care: James E. Eullaran Katrina Ysabelle Garcia Kathleen Mae R. Flores April 16, 2019James eullaranNo ratings yet
- An Essay About MotherDocument6 pagesAn Essay About Motherzzcpllaeg100% (2)
- Literature ReviewDocument4 pagesLiterature ReviewSonam ChodenNo ratings yet
- Project On Analysis of Attitude of Pregnant Mother Towards Antenatal Care ServiceDocument50 pagesProject On Analysis of Attitude of Pregnant Mother Towards Antenatal Care ServiceYUSUF AMINUNo ratings yet
- Lupus Case PresentationDocument48 pagesLupus Case PresentationRoscelie KhoNo ratings yet
- Project Documentation Thesis BookDocument66 pagesProject Documentation Thesis BookMAHER MOHAMEDNo ratings yet
- Antenatal CareDocument3 pagesAntenatal CareSimranNo ratings yet
- 5 - Care of The Mother and The FetusDocument36 pages5 - Care of The Mother and The FetusMa Nelia P MagsinoNo ratings yet
- Kalusugan ReflectionDocument3 pagesKalusugan ReflectionRizza Mae CallejaNo ratings yet
- Antenatal CareDocument19 pagesAntenatal CareIshika RoyNo ratings yet
- Prenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncDocument33 pagesPrenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncISFAHAN MASULOTNo ratings yet
- Teenage PregnancyDocument4 pagesTeenage PregnancyjoannesalagubangNo ratings yet
- N E E D S C O G N I T I V E P E R P E T U A L RationaleDocument14 pagesN E E D S C O G N I T I V E P E R P E T U A L RationaleArianna Jasmine MabungaNo ratings yet
- Innovative Approaches For Improving Maternal and Newborn Health - A Landscape AnalysisDocument19 pagesInnovative Approaches For Improving Maternal and Newborn Health - A Landscape AnalysisAli Abubakar AuduNo ratings yet
- Alignment of Performance Based Financing in Health With The Government Budget A Principle Based ApproachDocument42 pagesAlignment of Performance Based Financing in Health With The Government Budget A Principle Based ApproachCandra, MPHNo ratings yet