Download as pdf or txt
You might also like
- Vascular Access Principles and Practice by Samuel Eric WilsonDocument328 pagesVascular Access Principles and Practice by Samuel Eric WilsonBruno ZanuttiniNo ratings yet
- The Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomyDocument4 pagesThe Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomywachito ricoNo ratings yet
- The Many Varieties of Catatonia: Max Fink Michael A. TaylorDocument7 pagesThe Many Varieties of Catatonia: Max Fink Michael A. TaylorRoy FloresNo ratings yet
- 1943 - Further Experiments On Thiamine Deficiency in ManDocument16 pages1943 - Further Experiments On Thiamine Deficiency in ManSimon SaundersNo ratings yet
- Poison TableDocument12 pagesPoison TableKirk NeneriaNo ratings yet
- The AmebaDocument7 pagesThe AmebaSandra Mhay RodilloNo ratings yet
- Trypanocidal Effect of Diminazene Aceturate byDocument6 pagesTrypanocidal Effect of Diminazene Aceturate byCristina SorairesNo ratings yet
- CE Forceris Art N3 LRDocument7 pagesCE Forceris Art N3 LRLài LêNo ratings yet
- Final RheaDocument5 pagesFinal RheaRhealyn LegaspiNo ratings yet
- A Case Report of Echinostoma Species For The First Time in NepalDocument2 pagesA Case Report of Echinostoma Species For The First Time in NepalniniNo ratings yet
- Sulfasalazine Toxic Reactions. Hepatitis, Fever, and Skin Rash With Hypocomplementemia and Immune ComplexesDocument2 pagesSulfasalazine Toxic Reactions. Hepatitis, Fever, and Skin Rash With Hypocomplementemia and Immune ComplexesChistian LassoNo ratings yet
- High-Dose Thiamine Improves The Symptoms of FibromyalgiaDocument4 pagesHigh-Dose Thiamine Improves The Symptoms of FibromyalgiaVivekNo ratings yet
- A Rare Case of Acute Abdomen Secondary To Omental.283Document1 pageA Rare Case of Acute Abdomen Secondary To Omental.283prabowoaji12No ratings yet
- NCP PEDIA TonsillitisDocument2 pagesNCP PEDIA Tonsillitisdeliejoyce100% (1)
- Pengaruh Pemberian Antibiotika Amoksisilin Dan Tetrasiklin Terhadap Gambaran Urine Pada KUCING LOKAL (Felis Catus)Document9 pagesPengaruh Pemberian Antibiotika Amoksisilin Dan Tetrasiklin Terhadap Gambaran Urine Pada KUCING LOKAL (Felis Catus)ansariNo ratings yet
- Sic 2Document4 pagesSic 2Ezra Miguel DarundayNo ratings yet
- Giant Gastric Trichobezoar in A Female TeenagerDocument6 pagesGiant Gastric Trichobezoar in A Female TeenagerSajag GuptaNo ratings yet
- Histamine, Histamine Receptors, and Their Role in Immunomodulation: An Updated Systematic ReviewDocument33 pagesHistamine, Histamine Receptors, and Their Role in Immunomodulation: An Updated Systematic ReviewRizka Dwi AuliaNo ratings yet
- Pharmacokinetics of High-Dose Oral Thiamine Hydrochloride in Healthy SubjectsDocument10 pagesPharmacokinetics of High-Dose Oral Thiamine Hydrochloride in Healthy SubjectsHerawati YustikasariNo ratings yet
- 10 Myth About Tannin in SorghumDocument3 pages10 Myth About Tannin in SorghumWilly YanuwarNo ratings yet
- Clinical Parasitology Lecture: The FlagellatesDocument18 pagesClinical Parasitology Lecture: The FlagellatesGyu KimNo ratings yet
- Microbiology and Parasitology Given Parasites Identify The Following A. Common Name B. Geographical Distribution in The PhilippinesDocument29 pagesMicrobiology and Parasitology Given Parasites Identify The Following A. Common Name B. Geographical Distribution in The PhilippinesTea-yuhNo ratings yet
- Surgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Document7 pagesSurgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Ayu DinaNo ratings yet
- Histamina Metabolismo Ing.Document2 pagesHistamina Metabolismo Ing.Sócrates De AtenasNo ratings yet
- From Son 1973Document4 pagesFrom Son 1973Abhishek JunghareNo ratings yet
- Bioavaibility Melatonin 00912700022009422Document4 pagesBioavaibility Melatonin 00912700022009422sd221wsNo ratings yet
- Thiamine - Vitamins (Vit b1) - IV FLUIDS Fabros, JennyDocument2 pagesThiamine - Vitamins (Vit b1) - IV FLUIDS Fabros, JennyJenny Agustin FabrosNo ratings yet
- Cefixime Case Pre RhuDocument1 pageCefixime Case Pre RhuJohn Karl Garcia RazalanNo ratings yet
- Activity No. 9: Name: Lacastesantos, Bryan E. Course and Section: BSN 1-1EDocument4 pagesActivity No. 9: Name: Lacastesantos, Bryan E. Course and Section: BSN 1-1EKeen Jude CaminosNo ratings yet
- CE Forceris Art N4 LRDocument7 pagesCE Forceris Art N4 LRLài LêNo ratings yet
- Beisel1995Herman Award Lecture, 1995 Infection-Induced Malnutrition-From Cholera To Cytokines.Document7 pagesBeisel1995Herman Award Lecture, 1995 Infection-Induced Malnutrition-From Cholera To Cytokines.PWaaaaNo ratings yet
- AMOEBIASISDocument1 pageAMOEBIASISjeromedcNo ratings yet
- Health Teaching Plan DRDocument1 pageHealth Teaching Plan DREYANAH DELOS REYESNo ratings yet
- محاضرة سادسة رابع نظريDocument7 pagesمحاضرة سادسة رابع نظريaust austNo ratings yet
- The Gastro-Intestinal SystemDocument12 pagesThe Gastro-Intestinal SystemRenelyn ComiaNo ratings yet
- HIRSCHSPRUNGDocument1 pageHIRSCHSPRUNGAezyreal Anne MirallesNo ratings yet
- Concept Map Day 5 (Constipation)Document4 pagesConcept Map Day 5 (Constipation)Matt McKinleyNo ratings yet
- Intended Learning OutcomeDocument1 pageIntended Learning OutcomeJade CentinoNo ratings yet
- Treatment of Postpartum Endometritis: Hospital PracticeDocument8 pagesTreatment of Postpartum Endometritis: Hospital Practicefalon papalangiNo ratings yet
- It Is Caused By:: Definition of TyphusDocument2 pagesIt Is Caused By:: Definition of TyphusAshima Viie BassamahNo ratings yet
- Beriberi (Thiamine Deficiency) and High Infant Mortality in Northern LaosDocument16 pagesBeriberi (Thiamine Deficiency) and High Infant Mortality in Northern LaosNurfadhilah YusufNo ratings yet
- Health Teaching PlanDocument6 pagesHealth Teaching PlanLody Lean CruzNo ratings yet
- Jurnal 5Document5 pagesJurnal 5Asniar RNo ratings yet
- Appendisitis TBDocument41 pagesAppendisitis TBrachmi mirnaNo ratings yet
- Materi AnemiaDocument9 pagesMateri AnemiaMeyrha Hi BayanNo ratings yet
- Bertrand10 MelatoninDocument12 pagesBertrand10 MelatoninmjpozoNo ratings yet
- Pediatrics: Abdominal Epilepsy in ChildhoodDocument6 pagesPediatrics: Abdominal Epilepsy in ChildhoodGanjar SulaksmonoNo ratings yet
- El Efecto de La Etionina en La Transmetilación de La Meionina A Colina y Creatina in Vivo "Document6 pagesEl Efecto de La Etionina en La Transmetilación de La Meionina A Colina y Creatina in Vivo "Carlos VargasNo ratings yet
- Parasitology HandoutsDocument12 pagesParasitology HandoutsJed Imperial100% (1)
- Thiamine Tetrahydrofurfuryl Disulfi De: A Little Known Therapeutic AgentDocument6 pagesThiamine Tetrahydrofurfuryl Disulfi De: A Little Known Therapeutic AgentPrima DimalouwNo ratings yet
- Thiamine and Selected Thiamine Antivitamins - Biological Activity and Methods of SynthesisDocument24 pagesThiamine and Selected Thiamine Antivitamins - Biological Activity and Methods of SynthesisAnomSuryaNo ratings yet
- VILLAMIN - Drug StudyDocument4 pagesVILLAMIN - Drug StudyAzizah VillaminNo ratings yet
- Review Article: Gastric Pathological FindingsDocument8 pagesReview Article: Gastric Pathological FindingsYosi Puput MaharaniNo ratings yet
- Effectofberberineon GiardiasisDocument5 pagesEffectofberberineon GiardiasisSummiNo ratings yet
- Common Parasites: Nematodes (Roundworm) Common Name MOT Mode of Transmission IS Symptoms Cause DiseaseDocument2 pagesCommon Parasites: Nematodes (Roundworm) Common Name MOT Mode of Transmission IS Symptoms Cause DiseaseYAM ABOUHATABNo ratings yet
- Cinnamon As Wound HealingDocument4 pagesCinnamon As Wound HealingfadalNo ratings yet
- 49 Articolo D'Angelo R. 7.2Document7 pages49 Articolo D'Angelo R. 7.2Abhishek KubalNo ratings yet
- Flora Intestina LavandaDocument5 pagesFlora Intestina LavandajuanNo ratings yet
- College of Nursing: Cebu Normal UniversityDocument3 pagesCollege of Nursing: Cebu Normal UniversityShiva TorinsNo ratings yet
- Experience With IV Metronidazole To Treat Moderate To Severe Amebiasis in JapanDocument5 pagesExperience With IV Metronidazole To Treat Moderate To Severe Amebiasis in JapanRobin ScherbatskyNo ratings yet
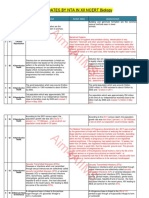
- Aim4AIIMS: Updates by Nta in Xii Ncert BiologyDocument12 pagesAim4AIIMS: Updates by Nta in Xii Ncert BiologyYashesh ChoukseyNo ratings yet
- Surgical Management of An Abdominal Abscess in A Malayan TapirDocument3 pagesSurgical Management of An Abdominal Abscess in A Malayan TapirPaulo MorgadoNo ratings yet
- 1 s2.0 S0021925818760493 MainDocument7 pages1 s2.0 S0021925818760493 MainMarko Sanja StikovicNo ratings yet
- Sulfur IntoleranceDocument1 pageSulfur IntoleranceMarko Sanja StikovicNo ratings yet
- 1 s2.0 S0021925818698229 MainDocument3 pages1 s2.0 S0021925818698229 MainMarko Sanja StikovicNo ratings yet
- 01 Oglas 20221116Document2 pages01 Oglas 20221116Marko Sanja StikovicNo ratings yet
- Dietary Fat and Risk of Renal Cell Carcinoma in The Usa A Casecontrol StudyDocument11 pagesDietary Fat and Risk of Renal Cell Carcinoma in The Usa A Casecontrol StudyMarko Sanja StikovicNo ratings yet
- ENDOCRINE PRACTICE Rapid Electronic Article in Press: AACE/ACE Consensus StatementDocument66 pagesENDOCRINE PRACTICE Rapid Electronic Article in Press: AACE/ACE Consensus StatementMUHAMMAD09No ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- CardiotocographyDocument51 pagesCardiotocographyticticNo ratings yet
- IMS Biosimilar 2017 - V9 PDFDocument33 pagesIMS Biosimilar 2017 - V9 PDFPamela Ruiz RuizNo ratings yet
- DOH Pre Spanish EraDocument6 pagesDOH Pre Spanish EraKyle MendozaNo ratings yet
- Pseudomonas Aeruginosa : Most CommonDocument2 pagesPseudomonas Aeruginosa : Most CommonSoojung Nam100% (1)
- MrsDocument2 pagesMrsHelen SabuquelNo ratings yet
- Journal Multivariate Mita2016Document36 pagesJournal Multivariate Mita2016Mange Sumange GffrNo ratings yet
- Arch Dis Child Fetal Neonatal Ed-2013-Boland-F201-4 PDFDocument5 pagesArch Dis Child Fetal Neonatal Ed-2013-Boland-F201-4 PDFMarce FloresNo ratings yet
- Laporan Pemakaian Dan Lembar Permintaan Obat (Lplpo) : Box at 50 TabletDocument29 pagesLaporan Pemakaian Dan Lembar Permintaan Obat (Lplpo) : Box at 50 TabletIndrawan AnwarNo ratings yet
- Daftar Pustaka: Aurum Wanda Dewana, Ibu Ida Fitriana, S.Farm., Apt., M.SCDocument6 pagesDaftar Pustaka: Aurum Wanda Dewana, Ibu Ida Fitriana, S.Farm., Apt., M.SCFebriyono AnggelaNo ratings yet
- Patient Specific Dental Hygiene Care PlanDocument8 pagesPatient Specific Dental Hygiene Care Planapi-354959885No ratings yet
- Re Ca VADocument9 pagesRe Ca VAmanudanuNo ratings yet
- BaOH2 PDFDocument5 pagesBaOH2 PDFGhana Cintai DiaNo ratings yet
- Horizontal Gene Transfer Among Bacteria and Its Role in Biological EvolutionDocument8 pagesHorizontal Gene Transfer Among Bacteria and Its Role in Biological EvolutionHarold Earl Cabungcal VenalNo ratings yet
- THE SOCIAL TERRORIST, The Day AIDS Became A Global Threat! A Novel by Joseph P. ChaddockDocument112 pagesTHE SOCIAL TERRORIST, The Day AIDS Became A Global Threat! A Novel by Joseph P. ChaddockJoseph Caratti100% (1)
- DIAGNOSTICS (Student Copy)Document59 pagesDIAGNOSTICS (Student Copy)Abigail Mayled LausNo ratings yet
- Browne 2011Document11 pagesBrowne 2011Gisele Elise MeninNo ratings yet
- Plants Used in Mexican Traditional Medicine July 04Document180 pagesPlants Used in Mexican Traditional Medicine July 04Biol. Miguel Angel Gutiérrez DomínguezNo ratings yet
- The 28 All-Time Best Healing FoodsDocument64 pagesThe 28 All-Time Best Healing FoodsMardz100% (2)
- MNCHN RNHealsDocument58 pagesMNCHN RNHealstinea nigraNo ratings yet
- English (Respiratory System)Document16 pagesEnglish (Respiratory System)ChitraNo ratings yet
- Dr. R. W. Bernard - Science Discovers The Psychological Value of ContinenceDocument31 pagesDr. R. W. Bernard - Science Discovers The Psychological Value of ContinenceOliveros2012No ratings yet
- Animal Husbandry Department Asked To Shut Down Dog Breeding Unit But PETA India Failed To Book Animal Abusers, Rescue of Animals, Why?Document2 pagesAnimal Husbandry Department Asked To Shut Down Dog Breeding Unit But PETA India Failed To Book Animal Abusers, Rescue of Animals, Why?Abhishek KadyanNo ratings yet
- Homework Assignment 1: Creative Hopelessness: InstructionsDocument2 pagesHomework Assignment 1: Creative Hopelessness: Instructionsswandal1No ratings yet
- List of Product For CE ExcelDocument92 pagesList of Product For CE Excelsaledepartment.adqNo ratings yet
- In This Issue Getting To Zero: Updates and Activities of The Gfatm RCC Ii PPTCT ProgramDocument6 pagesIn This Issue Getting To Zero: Updates and Activities of The Gfatm RCC Ii PPTCT ProgramIets PcgNo ratings yet