Download as pdf or txt
You might also like
- Final Myocardial Infarction Pathophysiology PDFDocument3 pagesFinal Myocardial Infarction Pathophysiology PDFDave JoshuaNo ratings yet
- Pathophysiology of Diabetes Mellitus Type 2Document4 pagesPathophysiology of Diabetes Mellitus Type 2jo_annamae4413100% (3)
- Onion Root Tip MitosisDocument5 pagesOnion Root Tip MitosisNor Ashikin IsmailNo ratings yet
- Coro 120 Operators ManualDocument256 pagesCoro 120 Operators ManualRaul PerezNo ratings yet
- Cardiovascular Disorders Concept MapDocument4 pagesCardiovascular Disorders Concept MapZairaNo ratings yet
- SW9.1x Instruction of Use PDFDocument302 pagesSW9.1x Instruction of Use PDFAl ImranNo ratings yet
- Neuro-Transmitter Questionnaire: Determining Your Dominant NatureDocument6 pagesNeuro-Transmitter Questionnaire: Determining Your Dominant NatureBrad100% (1)
- Yuri Verkhoshansky - (02) OrganizationOfTheTrainingProcessDocument19 pagesYuri Verkhoshansky - (02) OrganizationOfTheTrainingProcessOdraudeIttereip100% (4)
- Muscle Intelligence 30-Day Primer - Hams & GlutesDocument29 pagesMuscle Intelligence 30-Day Primer - Hams & GlutesPK100% (2)
- Pathophysiology of Acute Renal FailureDocument1 pagePathophysiology of Acute Renal FailureAina HaravataNo ratings yet
- Chronic Nephropathy Diabetic Glomerulonephritis Chronic PyelonephritisDocument1 pageChronic Nephropathy Diabetic Glomerulonephritis Chronic Pyelonephritisssiton886No ratings yet
- Clinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesDocument27 pagesClinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesradhiinathahirNo ratings yet
- Pathophysiology of cholangiocarcinomaJAYCERDocument3 pagesPathophysiology of cholangiocarcinomaJAYCERirish_estrellaNo ratings yet
- PATHOPHYDocument3 pagesPATHOPHYArlly Faena AbadNo ratings yet
- Patho5 8 - Renal Tubular Interstitial Dr. MesinaDocument10 pagesPatho5 8 - Renal Tubular Interstitial Dr. MesinaMonique BorresNo ratings yet
- Pathway HDDocument2 pagesPathway HDketut dana.No ratings yet
- 12 Years 15 Years: HypertensionDocument4 pages12 Years 15 Years: HypertensionKathleenNo ratings yet
- Pa Tho Physiology of Sepsis Secondary To Typhoid IleusDocument6 pagesPa Tho Physiology of Sepsis Secondary To Typhoid IleusPhatsee PangilinanNo ratings yet
- Journal Reading - Haemostatic ResuscitationDocument47 pagesJournal Reading - Haemostatic ResuscitationNeva ArunikaNo ratings yet
- O High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleDocument4 pagesO High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleJoherNo ratings yet
- Acute Kidney Injury: Lantin/Reyes/Sanchez/SevillaDocument32 pagesAcute Kidney Injury: Lantin/Reyes/Sanchez/SevillaKen Edward ZataNo ratings yet
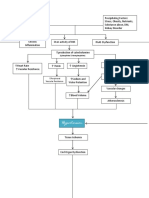
- Spider Web Acute Renal FailureDocument3 pagesSpider Web Acute Renal FailureTien KartiniNo ratings yet
- Chapter 11. Chemotherapy and Kidney InjuryDocument10 pagesChapter 11. Chemotherapy and Kidney InjuryIs KahnNo ratings yet
- CeVD, MI, HCVD & Atrial Fibrillation PathophysiologyDocument3 pagesCeVD, MI, HCVD & Atrial Fibrillation PathophysiologyJjessmar Bolivar FamaNo ratings yet
- Hypertension Obstruction: Chronic Renal FailureDocument3 pagesHypertension Obstruction: Chronic Renal FailureDiane-Richie PezLo100% (1)
- Transient Ischemic Attack Precipitating Factors Predisposing FactorsDocument6 pagesTransient Ischemic Attack Precipitating Factors Predisposing FactorsYosef OxinioNo ratings yet
- Mechanism Involved in Remote Injury To The Gut Mucosa Leading To Gut Barrier Failure After Liver Ischemia/ Reperfusion InjuryDocument3 pagesMechanism Involved in Remote Injury To The Gut Mucosa Leading To Gut Barrier Failure After Liver Ischemia/ Reperfusion InjuryvanW92No ratings yet
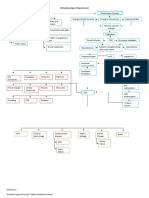
- ARF PathoDocument3 pagesARF PathoNikki RodrigoNo ratings yet
- Stimulate Renin Release: Decreased Blood Flow To O2 KidneyDocument2 pagesStimulate Renin Release: Decreased Blood Flow To O2 KidneyMiguelito Galagar GultianoNo ratings yet
- PathophysiologyDocument34 pagesPathophysiologyeunams_1195% (20)
- Pre Eclampsia of Severe FeaturesDocument3 pagesPre Eclampsia of Severe FeaturesPrincess Diane S. VillegasNo ratings yet
- Ascites: Saag Albumin AlbuminDocument7 pagesAscites: Saag Albumin AlbuminMike GNo ratings yet
- Allopurinol (Drug Study)Document2 pagesAllopurinol (Drug Study)Daisy PalisocNo ratings yet
- 6 Med Ward (WK - 1) PathophysiologyDocument3 pages6 Med Ward (WK - 1) PathophysiologyZaijean Kate Dianne LigutomNo ratings yet
- Heart Failure: Peter A. Mccullough, MD, MPH, Facc, Facp, Faha, FCCPDocument54 pagesHeart Failure: Peter A. Mccullough, MD, MPH, Facc, Facp, Faha, FCCPDenisse Tinajero SánchezNo ratings yet
- Pathophysiology of ESRDDocument3 pagesPathophysiology of ESRDjake90210100% (1)
- Sirosis HepatisDocument65 pagesSirosis HepatisIntania Fadilla100% (1)
- Anemia Ugib PathoDocument2 pagesAnemia Ugib PathoAj GoNo ratings yet
- Pathophysio of Type 2 Diabetes With Secondary Hypertension PDFDocument6 pagesPathophysio of Type 2 Diabetes With Secondary Hypertension PDFDingsNo ratings yet
- Aki EditedDocument8 pagesAki EditedLarabelle Avila CoralesNo ratings yet
- Modifiable Risk Factors: Non-Modifiable Risk Factors:: IV. Pathophysiology of Chronic Kidney DiseaseDocument5 pagesModifiable Risk Factors: Non-Modifiable Risk Factors:: IV. Pathophysiology of Chronic Kidney DiseaseSteffi MurielNo ratings yet
- DM Tipe II Rasa: GDS 203 MG/DL Hba1c 7,3% APTT 22,8 DetikDocument1 pageDM Tipe II Rasa: GDS 203 MG/DL Hba1c 7,3% APTT 22,8 DetikAndrianus AtuNo ratings yet
- Acute Kidney Injury (AKI)Document50 pagesAcute Kidney Injury (AKI)Omar AbdillahiNo ratings yet
- Acute Kidney Injury (AKI) : Volume Depletion VascularDocument7 pagesAcute Kidney Injury (AKI) : Volume Depletion VascularJennyu YuNo ratings yet
- Kidney GM Eng 2020Document31 pagesKidney GM Eng 2020snowrose2609No ratings yet
- 2 - Concept Map 4Document4 pages2 - Concept Map 4keshav singhNo ratings yet
- Renal Failure: SMF Urologi FK-Unpar / RSUD Dr. Doris SylvanusDocument53 pagesRenal Failure: SMF Urologi FK-Unpar / RSUD Dr. Doris SylvanusClarissa SuheryNo ratings yet
- Tatalaksana Hiperosmolar Hiperglicemic State (SHH)Document16 pagesTatalaksana Hiperosmolar Hiperglicemic State (SHH)Vidya VidyutNo ratings yet
- 4 Kidney Diseases TogleMDDocument1 page4 Kidney Diseases TogleMDMarianneNo ratings yet
- MHD Exam 5 MaterialDocument122 pagesMHD Exam 5 Materialnaexuis5467100% (1)
- Menigitis & EncephalitisDocument38 pagesMenigitis & EncephalitisKim GonzalesNo ratings yet
- 2.3 Patofisiologi Penyakit HipertensiDocument5 pages2.3 Patofisiologi Penyakit HipertensiNicky Putri CapindoNo ratings yet
- Tatalaksana Hiperosmolar Hiperglicemic State (SHH)Document13 pagesTatalaksana Hiperosmolar Hiperglicemic State (SHH)Vidya VidyutNo ratings yet
- Renal Failure DefinisiDocument4 pagesRenal Failure DefinisiLentinaNo ratings yet
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- Hemodynamic Disorders, Thromboembolic Disease and ShockDocument3 pagesHemodynamic Disorders, Thromboembolic Disease and ShockRuel MateoNo ratings yet
- Pathophysiology of Acute Kidney Injury (Aki) Caused by ShockDocument26 pagesPathophysiology of Acute Kidney Injury (Aki) Caused by ShockbokobokobokanNo ratings yet
- Referat AKI DionDocument39 pagesReferat AKI DionRyanNo ratings yet
- Pathophysiology HypertensionDocument4 pagesPathophysiology HypertensionKimberly BautistaNo ratings yet
- Renin Angiotensin Aldosterone Systems Nitrates Oct14Document10 pagesRenin Angiotensin Aldosterone Systems Nitrates Oct14Mohammad Hazamyn Hazrul HamzahNo ratings yet
- RHF and CRSDocument15 pagesRHF and CRSnataliawara92No ratings yet
- Traumatic Brain Injury Related To Blunt Face and Questionable FallDocument2 pagesTraumatic Brain Injury Related To Blunt Face and Questionable FallGenette Sy SolisNo ratings yet
- 1035 Pathway CKDDocument1 page1035 Pathway CKDeka pandeNo ratings yet
- Hypertension PathoDocument2 pagesHypertension Pathojake90210100% (1)
- HYPERTENSIONSSSSDocument1 pageHYPERTENSIONSSSSJulianne Jeamer FabroaNo ratings yet
- BursDocument3 pagesBursminangsung minangnengNo ratings yet
- Island (Isla) Plateau (Talampas) : Mountain (Bundok)Document3 pagesIsland (Isla) Plateau (Talampas) : Mountain (Bundok)minangsung minangnengNo ratings yet
- Consent Form Google DocsDocument2 pagesConsent Form Google Docsminangsung minangnengNo ratings yet
- KYPHOSISDocument18 pagesKYPHOSISminangsung minangnengNo ratings yet
- Babs AstigmatismDocument1 pageBabs Astigmatismminangsung minangnengNo ratings yet
- OSCE ReviewerDocument17 pagesOSCE Reviewerminangsung minangnengNo ratings yet
- AutismDocument26 pagesAutismminangsung minangnengNo ratings yet
- Case Presentation Acute GlomerulonephritisDocument10 pagesCase Presentation Acute Glomerulonephritisminangsung minangnengNo ratings yet
- Last PartDocument5 pagesLast Partminangsung minangnengNo ratings yet
- Acute Glomerulonephritis PathophysioDocument4 pagesAcute Glomerulonephritis Pathophysiominangsung minangnengNo ratings yet
- Bonapace PDFDocument9 pagesBonapace PDFIztho LiufetoNo ratings yet
- Summative Skeletal SystemDocument3 pagesSummative Skeletal SystemVarun MangotraNo ratings yet
- N5 Biology All 2018Document48 pagesN5 Biology All 2018Sajida CheemaNo ratings yet
- Multiple Myeloma With PathophysiologyDocument32 pagesMultiple Myeloma With Pathophysiologymabec pagaduan90% (10)
- Astm ErsDocument9 pagesAstm ErsAdrian RomanNo ratings yet
- KN 4@enzl 8 Ha 4 B 6 CC 9 eDocument26 pagesKN 4@enzl 8 Ha 4 B 6 CC 9 eRamzen Raphael DomingoNo ratings yet
- Activity 6-Module 1Document1 pageActivity 6-Module 1Kristine Ibarreta-JazulNo ratings yet
- Cell DivisionDocument10 pagesCell DivisionMEDRANO, Hana Jhiemyka O.No ratings yet
- Liver CirrhosisDocument83 pagesLiver CirrhosisRusiana NasilahNo ratings yet
- ImplantationDocument18 pagesImplantationNurulAqilahZulkifliNo ratings yet
- Spirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Document60 pagesSpirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Alkaustariyah LubisNo ratings yet
- Amino Acids in Animal NutritionDocument515 pagesAmino Acids in Animal NutritionLuciana EmanuelleNo ratings yet
- Effect of Yoga On Subclinical Hypothyroidism: A Case ReportDocument8 pagesEffect of Yoga On Subclinical Hypothyroidism: A Case ReportpronitNo ratings yet
- Msds CaffeineDocument6 pagesMsds CaffeineNovia RegitaNo ratings yet
- Mictonorm Product InsertDocument6 pagesMictonorm Product InsertChung Wen WeiNo ratings yet
- EthisomeDocument147 pagesEthisomeMurali KrishnaNo ratings yet
- Maxillary ArteryDocument30 pagesMaxillary ArteryMeriam AntonyNo ratings yet
- Fish Anatomy For Fish BreedingDocument2 pagesFish Anatomy For Fish BreedinghumanupgradeNo ratings yet
- The Life of A Flowering PlantDocument19 pagesThe Life of A Flowering PlantMedinaNo ratings yet
- Chest Physiotherapy Using Trendelenberg: (Age 2 and Older)Document5 pagesChest Physiotherapy Using Trendelenberg: (Age 2 and Older)riena456No ratings yet
- Ecg Made EasyDocument45 pagesEcg Made EasyVinoth Kumar RaviNo ratings yet
- Lane 2004Document9 pagesLane 2004Mia KobašNo ratings yet
- Schools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasDocument2 pagesSchools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasSharna Flynn SolonNo ratings yet
- Care of Low Birth Weight BabiesDocument102 pagesCare of Low Birth Weight Babiesvarshasharma050% (2)