Download as pdf or txt
You might also like
- (The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive ADocument1,088 pages(The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive AEdu Martins100% (1)
- Internal Medicine NBME 3Document52 pagesInternal Medicine NBME 3Esteph Anie79% (24)
- Pals Study GuideDocument8 pagesPals Study Guidefredyromanreyes100% (2)
- Ventilasi MekanikDocument47 pagesVentilasi MekanikzahrahNo ratings yet
- ECMO Cannulae, Cannulation, Components, Pumps and Set-UP UKEDocument23 pagesECMO Cannulae, Cannulation, Components, Pumps and Set-UP UKEPERFUZIJANo ratings yet
- CAP AfinaDocument30 pagesCAP Afinaphyna27No ratings yet
- Afina Fitra Firdaus Ppds Ipd 50Document30 pagesAfina Fitra Firdaus Ppds Ipd 5050Afina Fitra FirdausNo ratings yet
- An Ecmo PrimerDocument109 pagesAn Ecmo Primernicky_lauw5885No ratings yet
- 4-6 MV For ARDS (Basic Level)Document49 pages4-6 MV For ARDS (Basic Level)salwafathiNo ratings yet
- My Own Critical Care NotesDocument4 pagesMy Own Critical Care NotesSamer GobreialNo ratings yet
- Extracorporeal Membrane Oxygenation (ECMO) System.: Atrial Septal DefectDocument10 pagesExtracorporeal Membrane Oxygenation (ECMO) System.: Atrial Septal DefectDhina KaranNo ratings yet
- Mechanical VentilatorsDocument11 pagesMechanical VentilatorsIra Katrina Bernales MendozaNo ratings yet
- ITU Handbook For Non-Anaesthetists 214Document23 pagesITU Handbook For Non-Anaesthetists 214AtikaNo ratings yet
- Contoh Kasus-Dr - TunjungDocument22 pagesContoh Kasus-Dr - TunjungYas EliasNo ratings yet
- Anaesthesia For Aortic Aneurysm: BhupeshDocument70 pagesAnaesthesia For Aortic Aneurysm: BhupeshParvathy R NairNo ratings yet
- Open Heart 1Document18 pagesOpen Heart 1mohamedNo ratings yet
- Concept Mapping - FullDocument24 pagesConcept Mapping - Fulliamlibertarian100% (3)
- Duty Report: Sunday, 27 May 2018Document17 pagesDuty Report: Sunday, 27 May 2018HarisNo ratings yet
- EcmoDocument39 pagesEcmoSiriporn Pongpattarapak100% (1)
- Anesthesia Monitoring Systems 1Document80 pagesAnesthesia Monitoring Systems 1gnapikaNo ratings yet
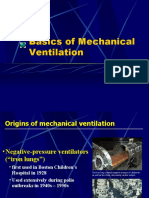
- Basics of Mechanical VentilationDocument38 pagesBasics of Mechanical VentilationbennyrolandnababanNo ratings yet
- ARDS Net AliDocument30 pagesARDS Net Aliamalia adeNo ratings yet
- Mortality conference: ߡⰊשʑⅶⷪず कẤⵒ Reporter: CR⨀ᆙ Supervisor: CVS ⫯⸉Document42 pagesMortality conference: ߡⰊשʑⅶⷪず कẤⵒ Reporter: CR⨀ᆙ Supervisor: CVS ⫯⸉劉彩屏No ratings yet
- Cardiopulmonary by PassDocument62 pagesCardiopulmonary by PassRezwanul Hoque Bulbul100% (1)
- ECMO BasicsDocument72 pagesECMO Basicszhelle2100% (2)
- Critical Care NursingDocument159 pagesCritical Care Nursinggretchen marie80% (5)
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- Setting VentilatorDocument10 pagesSetting VentilatorHafiz YusaryahyaNo ratings yet
- Critical Care NursingDocument159 pagesCritical Care NursingJoy Jarin50% (2)
- An Introduction To Surgical Icu.: Mohamed Emad Abdel-Ghaffar. Professor of Anesthesiology, Fom, King Faisal UniversityDocument38 pagesAn Introduction To Surgical Icu.: Mohamed Emad Abdel-Ghaffar. Professor of Anesthesiology, Fom, King Faisal UniversityHassan.shehriNo ratings yet
- ECMO Management Lecture 5Document39 pagesECMO Management Lecture 5dnafredyNo ratings yet
- Basics Mechanical VentilationDocument51 pagesBasics Mechanical VentilationademNo ratings yet
- ECHMODocument52 pagesECHMOanupama varghese100% (1)
- Weaning Ventilator Protocol For LiberationDocument3 pagesWeaning Ventilator Protocol For LiberationBonny ChristianNo ratings yet
- Admission To The ICU and Monitoring Technique Early Postoperative CareDocument7 pagesAdmission To The ICU and Monitoring Technique Early Postoperative CareWidiartha WahyudiNo ratings yet
- Pulmonary Artery CatheterizationDocument15 pagesPulmonary Artery Catheterizationأبو أويس شرف الدينNo ratings yet
- Day in The Life 2019Document30 pagesDay in The Life 2019Hoa Cỏ ĐậuNo ratings yet
- Basics of EcmoDocument7 pagesBasics of EcmolakongkorNo ratings yet
- HFOV High-Frequency-Oscillatory-VentilationDocument22 pagesHFOV High-Frequency-Oscillatory-VentilationJZNo ratings yet
- Adult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPDocument51 pagesAdult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPArsitoNo ratings yet
- Mechanical VentilationDocument62 pagesMechanical Ventilationdrphaninadella100% (1)
- Basics of ECMO Part 2Document6 pagesBasics of ECMO Part 2corinna.ongaigui.gsbmNo ratings yet
- Evidence Based Mechanical Ventilation Strategies ARS-Cortes-PuentesDocument23 pagesEvidence Based Mechanical Ventilation Strategies ARS-Cortes-PuentesAli AftabNo ratings yet
- Blalock Taussig Shunt PDFDocument4 pagesBlalock Taussig Shunt PDFzuraini_mdnoorNo ratings yet
- Mechanical Ventilation AulaDocument47 pagesMechanical Ventilation Aulaapi-3820606100% (1)
- Modes of Ventilation PDFDocument30 pagesModes of Ventilation PDFsgod34No ratings yet
- COVIDDocument23 pagesCOVID24 Narong ReedNo ratings yet
- An Introduction To Surgical Icu.: by DR Farrukh SaeedDocument33 pagesAn Introduction To Surgical Icu.: by DR Farrukh SaeedTARIQNo ratings yet
- Capnography in ICUDocument49 pagesCapnography in ICUherbertglennyNo ratings yet
- Percutaneous InterventionsDocument55 pagesPercutaneous InterventionsShannon Bellamy-FoggNo ratings yet
- Transposition of Great Arteries (TGA)Document6 pagesTransposition of Great Arteries (TGA)zuraini_mdnoorNo ratings yet
- IABP FINAL by Mr. Adnan (13-04-2020 To 04-05-2020Document33 pagesIABP FINAL by Mr. Adnan (13-04-2020 To 04-05-2020Atia KiranNo ratings yet
- ECMO (Extracorporeal Membrane Oxygenation)Document39 pagesECMO (Extracorporeal Membrane Oxygenation)Linto John100% (1)
- Guias ElsoDocument10 pagesGuias ElsoSebastián Caimanque CortésNo ratings yet
- Care of Patients With Acute Biologic CrisisDocument72 pagesCare of Patients With Acute Biologic CrisisJames QuilingNo ratings yet
- Use of One-Lung Ventilation For Thoracic SurgeryDocument26 pagesUse of One-Lung Ventilation For Thoracic SurgeryErinne DefrianiNo ratings yet
- Post Anesthesia Care Unit (Pacu) : Department of Anesthesiology & Reanimation School of Medicine, Malahayati UniversityDocument46 pagesPost Anesthesia Care Unit (Pacu) : Department of Anesthesiology & Reanimation School of Medicine, Malahayati UniversityIbnu DharmajatiNo ratings yet
- Archives of Renal Diseases and ManagementDocument3 pagesArchives of Renal Diseases and ManagementPeertechz Publications Inc.No ratings yet
- 0bbamechanical VentilationDocument85 pages0bbamechanical VentilationKamal MohamedNo ratings yet
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Difficult Cases Septic ShockDocument53 pagesDifficult Cases Septic ShockHoa Cỏ ĐậuNo ratings yet
- Day in The Life 2019Document30 pagesDay in The Life 2019Hoa Cỏ ĐậuNo ratings yet
- Cardiac ECMO Cases - TDDocument17 pagesCardiac ECMO Cases - TDHoa Cỏ ĐậuNo ratings yet
- Anticoagulation For Ecmo 2019Document40 pagesAnticoagulation For Ecmo 2019Hoa Cỏ ĐậuNo ratings yet
- Paige Wilso, Teresa Ferster Glazier - The Least You Should Know About English - Writing Skills-Cengage Learning (2018)Document353 pagesPaige Wilso, Teresa Ferster Glazier - The Least You Should Know About English - Writing Skills-Cengage Learning (2018)Hoa Cỏ ĐậuNo ratings yet
- Parkland Formula For Burns Calculated DecisionsDocument2 pagesParkland Formula For Burns Calculated DecisionsJulia Ines ObregonNo ratings yet
- Blank Clinical Log - Spring 2nd HalfDocument2 pagesBlank Clinical Log - Spring 2nd HalfEileenNo ratings yet
- Cover Dan AbstrakDocument3 pagesCover Dan AbstrakAndhika DipaNo ratings yet
- Biochemistry - Lipid ProfileDocument1 pageBiochemistry - Lipid ProfileHassan RazaNo ratings yet
- Hypertensive Cardiovascular DiseaseDocument16 pagesHypertensive Cardiovascular DiseaseTintin Ponciano100% (1)
- Template Power EKG Rev SOS Maret 14 PDFDocument42 pagesTemplate Power EKG Rev SOS Maret 14 PDFAwe NugrohoNo ratings yet
- Transposition of The Great Arteries (TGA)Document4 pagesTransposition of The Great Arteries (TGA)Tommy JohnsonNo ratings yet
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDocument4 pagesCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- Morning Report 3 Neil Patel 2020Document14 pagesMorning Report 3 Neil Patel 2020PL NLNo ratings yet
- Medical Translation 3Document16 pagesMedical Translation 3rawdaeid0No ratings yet
- Nursing Care Plan AGNDocument2 pagesNursing Care Plan AGNAlexis Coronado50% (2)
- Function of The HeartDocument27 pagesFunction of The HeartAb Ab100% (1)
- HCVD Cad Cva InfarctionDocument2 pagesHCVD Cad Cva InfarctionMiguel Carlos Tacderan100% (1)
- Heart Assessment: Physical ExaminationDocument6 pagesHeart Assessment: Physical Examinationshannon c. lewisNo ratings yet
- High Sensitivity Cardiac Troponin T Increases After STR - 2019 - Clinical BiocheDocument6 pagesHigh Sensitivity Cardiac Troponin T Increases After STR - 2019 - Clinical BiocheFrankenstein MelancholyNo ratings yet
- PART+B +Biopotential+AmplifiersDocument3 pagesPART+B +Biopotential+Amplifierselztly4694No ratings yet
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- 3rd Quarter Exam ENGLISH 8Document2 pages3rd Quarter Exam ENGLISH 8Neiman J. MontonNo ratings yet
- 10 1016@j CCL 2020 04 008Document12 pages10 1016@j CCL 2020 04 008Linda Silvana SariNo ratings yet
- Periprocedural Anticoagulation Guidelines - UKDocument14 pagesPeriprocedural Anticoagulation Guidelines - UKjoshNo ratings yet
- bsm2300td 050620Document10 pagesbsm2300td 050620Fadi ZarraaNo ratings yet
- 2023 ACC Atrial FibrillationDocument171 pages2023 ACC Atrial FibrillationHill kanjinNo ratings yet
- Module 1 Questions and AnswersDocument2 pagesModule 1 Questions and AnswersAmberNo ratings yet
- Basic Life Support BLS Acls AtlsDocument24 pagesBasic Life Support BLS Acls AtlsCaptain AmericaNo ratings yet
- Cardiovascular Drugs: Dr. Hazha S. Ameen MSCDocument25 pagesCardiovascular Drugs: Dr. Hazha S. Ameen MSCAhmed MohamadNo ratings yet
- The Human Circulatory System: Teacher: D.Bleau School: ST Anthony's Secondary SchoolDocument10 pagesThe Human Circulatory System: Teacher: D.Bleau School: ST Anthony's Secondary SchoolCaiden HenryNo ratings yet
- Cardiovascular System SheetDocument11 pagesCardiovascular System SheetBetsy Brown ByersmithNo ratings yet
- Shock: Principles of Management: Nathan W. Mick, MD Massachusetts General Hospital Brigham and Women's HospitalDocument21 pagesShock: Principles of Management: Nathan W. Mick, MD Massachusetts General Hospital Brigham and Women's Hospitalifan zulfantriNo ratings yet