Download as pdf or txt
You might also like
- Infertility Concept MapDocument1 pageInfertility Concept Mapnursing concept maps50% (2)
- Art 3A10.1007 2Fs12672 015 0224 3Document8 pagesArt 3A10.1007 2Fs12672 015 0224 3Ariph BudiboyNo ratings yet
- Atm 07 05 100Document10 pagesAtm 07 05 100Farhan IrhamsyahNo ratings yet
- Clinicopathological Analysis of Nonfunctioning Pituitary Adenomas in Patients Younger Than 25 Years of AgeDocument6 pagesClinicopathological Analysis of Nonfunctioning Pituitary Adenomas in Patients Younger Than 25 Years of AgenaimNo ratings yet
- Horm 2002 1677Document8 pagesHorm 2002 1677MariaLyNguyễnNo ratings yet
- Interstitial Laser Photocoagulation For Treatment of Benign Prostatic Hypertrophy: Outcomes and Cost EffectivenessDocument8 pagesInterstitial Laser Photocoagulation For Treatment of Benign Prostatic Hypertrophy: Outcomes and Cost Effectivenessmutya yulindaNo ratings yet
- Do Not Copy: Dementia Is Associated With Chronic Rhinosinusitis: A Population-Based Case-Controlled StudyDocument5 pagesDo Not Copy: Dementia Is Associated With Chronic Rhinosinusitis: A Population-Based Case-Controlled StudyDominique MendozaNo ratings yet
- Boelaert2006 PDFDocument7 pagesBoelaert2006 PDFgustianto hutama pNo ratings yet
- Predictors of Positive Chest Radiography in Non-Traumatic Chest Pain in The Emergency DepartmentDocument5 pagesPredictors of Positive Chest Radiography in Non-Traumatic Chest Pain in The Emergency DepartmentHario Tri HendrokoNo ratings yet
- ThyroidDocument12 pagesThyroidHendra HermawanNo ratings yet
- Non-Suppressed Thyrotropin and Elevated Thyroglobulin Are Independent Predictors of Recurrence in Differentiated Thyroid CarcinomaDocument8 pagesNon-Suppressed Thyrotropin and Elevated Thyroglobulin Are Independent Predictors of Recurrence in Differentiated Thyroid CarcinomaPressureserveNo ratings yet
- Concurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung CancerDocument7 pagesConcurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung Cancerdurgesh kumarNo ratings yet
- Aldrich2021 Article ComparisonOfHypothyroidismGrowDocument8 pagesAldrich2021 Article ComparisonOfHypothyroidismGrowMona ElsaudiNo ratings yet
- Strokeaha 118 021301Document6 pagesStrokeaha 118 021301Rahma Nur AmeliaNo ratings yet
- Clinical Characteristics of Epithelioid Hemangioendothelioma: A Single-Center Retrospective StudyDocument8 pagesClinical Characteristics of Epithelioid Hemangioendothelioma: A Single-Center Retrospective StudyJose Huaman CamposNo ratings yet
- The Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyDocument6 pagesThe Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyagusNo ratings yet
- BPJ Vol 14 No 2 P 921-938Document18 pagesBPJ Vol 14 No 2 P 921-938Satish SinghNo ratings yet
- Advpub EJ18-0358Document7 pagesAdvpub EJ18-0358Arfiian Iffan BuddiarsoNo ratings yet
- Incidentally Diagnosed Adenocarcinoma Prostate After Surgery For Clinically Benign Prostatomegaly A 2 Years Retrospective StudyDocument6 pagesIncidentally Diagnosed Adenocarcinoma Prostate After Surgery For Clinically Benign Prostatomegaly A 2 Years Retrospective StudyIJAR JOURNALNo ratings yet
- Troponin ADocument18 pagesTroponin AMariangelRodriguezCNo ratings yet
- The First Affiliated Hospital of Zhengzhou University, Nöroloji, Zhengzhou, ÇinDocument12 pagesThe First Affiliated Hospital of Zhengzhou University, Nöroloji, Zhengzhou, ÇinwithoutlifeNo ratings yet
- J Ahj 2019 12 007Document29 pagesJ Ahj 2019 12 007Adriana MartinsNo ratings yet
- Epidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Document2 pagesEpidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Mirza RisqaNo ratings yet
- Ajh 10377Document6 pagesAjh 10377Dwika AudiyanandaNo ratings yet
- Tca 9 1453Document8 pagesTca 9 1453Pedro Gómez RNo ratings yet
- Development and Validation of A Prognostic NomogramDocument8 pagesDevelopment and Validation of A Prognostic Nomogramchao wangNo ratings yet
- Ikeda 2018Document7 pagesIkeda 2018Fatih KızılyelNo ratings yet
- Early Change in Platelet Count and MPV Levels of Patients Who Received Hemodialysis For The First Time Mogadishu Somalia ExperienceDocument5 pagesEarly Change in Platelet Count and MPV Levels of Patients Who Received Hemodialysis For The First Time Mogadishu Somalia ExperienceDea Fiesta JatikusumaNo ratings yet
- Risk HFDocument21 pagesRisk HFTeguh JayaNo ratings yet
- Jkns 2018 0153Document7 pagesJkns 2018 0153ioNo ratings yet
- The Impact of Cigarette Smoking On 24-Hour Blood Pressure, Inflammatory and Hemostatic Activity, and Cardiovascular Risk in Japanese Hypertensive PatientsDocument8 pagesThe Impact of Cigarette Smoking On 24-Hour Blood Pressure, Inflammatory and Hemostatic Activity, and Cardiovascular Risk in Japanese Hypertensive PatientsPutraChamplenxNo ratings yet
- 2 +Hardi+and+Soeroharjo +analysis+of+hematologicalDocument6 pages2 +Hardi+and+Soeroharjo +analysis+of+hematologicalInnayah KhnisaNo ratings yet
- Print 2 PDFDocument6 pagesPrint 2 PDFfk unswagatiNo ratings yet
- Starker 2016Document58 pagesStarker 2016brandon macarioNo ratings yet
- Chest 147 1 132Document8 pagesChest 147 1 132Timothy Eduard A. SupitNo ratings yet
- Avaliacao Doses FarmacoindutoresDocument7 pagesAvaliacao Doses FarmacoindutoresEnzoNo ratings yet
- Glycemic Control and Radiographic Manifestations of Tuberculosis in Diabetic PatientsDocument17 pagesGlycemic Control and Radiographic Manifestations of Tuberculosis in Diabetic PatientsGlenda B AjilaNo ratings yet
- Performance Evaluation of Five Different Disseminated Intravascular Coagulation (DIC) Diagnostic Criteria For Predicting Mortality in Patients With Complicated SepsisDocument8 pagesPerformance Evaluation of Five Different Disseminated Intravascular Coagulation (DIC) Diagnostic Criteria For Predicting Mortality in Patients With Complicated SepsisDwika AudiyanandaNo ratings yet
- Shock CorticioidesDocument5 pagesShock CorticioidesSebastián RinaldiNo ratings yet
- 2010-High-Sensitivoty of C-Reactive Protein and CancerDocument8 pages2010-High-Sensitivoty of C-Reactive Protein and CancerThalia KarampasiNo ratings yet
- Ijss Jan Oa08Document7 pagesIjss Jan Oa08IvanDwiKurniawanNo ratings yet
- Treatment For Benign Thyroid Nodules With A CombinDocument7 pagesTreatment For Benign Thyroid Nodules With A CombindarthjesussithNo ratings yet
- 1-s2.0-S1525505013004186 TUGAS INDAH-mainDocument5 pages1-s2.0-S1525505013004186 TUGAS INDAH-mainRendi Er PratamaNo ratings yet
- Diagnostic Approach To and Treatment of Thyroid Nodules - UpToDate PDFDocument36 pagesDiagnostic Approach To and Treatment of Thyroid Nodules - UpToDate PDFDANIEL SANTAMARIANo ratings yet
- Diagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDocument11 pagesDiagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDini NanamiNo ratings yet
- Clinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyDocument8 pagesClinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyPriya JainNo ratings yet
- Idiopathic First Seizure in Adult Life: Who Be Treated?: ShouldDocument4 pagesIdiopathic First Seizure in Adult Life: Who Be Treated?: ShouldJessica HueichiNo ratings yet
- Predicting 30-Day Case Fatality of Primary Inoperable Intracerebral Hemorrhage Based On Findings at The Emergency DepartmentDocument6 pagesPredicting 30-Day Case Fatality of Primary Inoperable Intracerebral Hemorrhage Based On Findings at The Emergency DepartmentNouchan NoupNo ratings yet
- One Stop Centre Staging by ContrastEnhanced FDG PETCT in Preoperative Assessment of Ovarian CancerDocument10 pagesOne Stop Centre Staging by ContrastEnhanced FDG PETCT in Preoperative Assessment of Ovarian CancerHana SalemNo ratings yet
- Metabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismDocument7 pagesMetabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismMaria Alice BourneufNo ratings yet
- Art Cancer Gastrico PDFDocument8 pagesArt Cancer Gastrico PDFvane_vane_tatyNo ratings yet
- Hyper Tiro IdDocument5 pagesHyper Tiro Idkonstantin balabalaNo ratings yet
- Diagnostic Value of Ischemia-Modified Albumin in Acute Coronary Syndrome and Acute Ischemic StrokeDocument5 pagesDiagnostic Value of Ischemia-Modified Albumin in Acute Coronary Syndrome and Acute Ischemic StrokeSarah KemalasariNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- The Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsDocument11 pagesThe Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsThinh VinhNo ratings yet
- RamachandranDocument9 pagesRamachandranjojobaggins100% (1)
- Preoperative Platelet-Lymphocyte Ratio Is A Superior Prognostic FactorDocument7 pagesPreoperative Platelet-Lymphocyte Ratio Is A Superior Prognostic Factordominguezmariela465No ratings yet
- 360 713 1 SMDocument8 pages360 713 1 SMadityachupezNo ratings yet
- Thyroid Nodules Diagnostic Evaluation Based OnDocument20 pagesThyroid Nodules Diagnostic Evaluation Based Ondiaspalma.medNo ratings yet
- Prognostic Significance of Neutrophil-to-Lymphocyte Ratio and PLRDocument9 pagesPrognostic Significance of Neutrophil-to-Lymphocyte Ratio and PLRdominguezmariela465No ratings yet
- (2009) Radiographic Improvement and Its Predictors in Patients With Pulmonary TuberculosisDocument6 pages(2009) Radiographic Improvement and Its Predictors in Patients With Pulmonary TuberculosisMohd RahimiNo ratings yet
- Enm 29 96Document5 pagesEnm 29 96Claudia IrimieNo ratings yet
- Italy StudyDocument8 pagesItaly StudyClaudia IrimieNo ratings yet
- Art 4Document5 pagesArt 4Claudia IrimieNo ratings yet
- Cushing IncidDocument10 pagesCushing IncidClaudia IrimieNo ratings yet
- Tumor Adrenale ItaliaDocument8 pagesTumor Adrenale ItaliaClaudia IrimieNo ratings yet
- OI2011 FRAXin Clinical PracticeDocument18 pagesOI2011 FRAXin Clinical PracticeClaudia IrimieNo ratings yet
- NutritionDocument4 pagesNutritionClaudia IrimieNo ratings yet
- Art 3Document6 pagesArt 3Claudia IrimieNo ratings yet
- Non Functional Parathyroid Cyst Masquerading As A Thyroid Cyst Report of Two Cases and Review of The LiteratureDocument6 pagesNon Functional Parathyroid Cyst Masquerading As A Thyroid Cyst Report of Two Cases and Review of The LiteratureClaudia IrimieNo ratings yet
- Artb 2Document11 pagesArtb 2Claudia IrimieNo ratings yet
- Subclinical Cushing's Syndrome: AACE 26th Annual Scientific & Clinical CongressDocument39 pagesSubclinical Cushing's Syndrome: AACE 26th Annual Scientific & Clinical CongressClaudia IrimieNo ratings yet
- Osteoporosis Men 10Document7 pagesOsteoporosis Men 10Claudia IrimieNo ratings yet
- Art 1Document4 pagesArt 1Claudia IrimieNo ratings yet
- Elevated Adrenocorticotropic Hormone, Hypercortisolism, and Marked HypernatremiaDocument8 pagesElevated Adrenocorticotropic Hormone, Hypercortisolism, and Marked HypernatremiaClaudia IrimieNo ratings yet
- Vitamindmetabolismin Bariatricsurgery: Marlene Chakhtoura,, Maya Rahme,, Ghada El-Hajj FuleihanDocument36 pagesVitamindmetabolismin Bariatricsurgery: Marlene Chakhtoura,, Maya Rahme,, Ghada El-Hajj FuleihanClaudia IrimieNo ratings yet
- Childhood and Puberty Close Monitoring (CPCM) Growth ChartDocument2 pagesChildhood and Puberty Close Monitoring (CPCM) Growth ChartClaudia IrimieNo ratings yet
- CT and MRI of Adrenal Gland PathologiesDocument23 pagesCT and MRI of Adrenal Gland PathologiesClaudia IrimieNo ratings yet
- CateterixareDocument4 pagesCateterixareClaudia IrimieNo ratings yet
- Cushing SubDocument7 pagesCushing SubClaudia IrimieNo ratings yet
- Glucoortixcoizii SarcinaDocument25 pagesGlucoortixcoizii SarcinaClaudia IrimieNo ratings yet
- 3.19.10 Sunderlin Pituitary AdenomaDocument10 pages3.19.10 Sunderlin Pituitary AdenomaClaudia IrimieNo ratings yet
- Abnormalities of Growth Hormone Lecture NO 02 MBBSDocument19 pagesAbnormalities of Growth Hormone Lecture NO 02 MBBSClaudia IrimieNo ratings yet
- 50 Year-Old Man Presents With Gynaecomastia: Case # 1Document63 pages50 Year-Old Man Presents With Gynaecomastia: Case # 1Claudia IrimieNo ratings yet
- Acromegaly: Jalisa BonillaDocument8 pagesAcromegaly: Jalisa BonillaClaudia Irimie100% (1)
- 05.31.1 Pathology of The BreastDocument107 pages05.31.1 Pathology of The BreastClaudia IrimieNo ratings yet
- Hiperlazie Adrenala CongenitalaDocument11 pagesHiperlazie Adrenala CongenitalaClaudia IrimieNo ratings yet
- BAETS Guidelines 2003Document28 pagesBAETS Guidelines 2003Claudia IrimieNo ratings yet
- Basics of Endocrinology: Kathleen Colleran MD Associate Professor of MedicineDocument48 pagesBasics of Endocrinology: Kathleen Colleran MD Associate Professor of MedicineClaudia IrimieNo ratings yet
- Hypophysis CerebriDocument21 pagesHypophysis CerebriAli Akand AsifNo ratings yet
- Pathophysilogy of Cushing Dse by OsmosisDocument4 pagesPathophysilogy of Cushing Dse by OsmosisEdrea MendezNo ratings yet
- TSH LiaisonDocument6 pagesTSH Liaisonsorayafathi90No ratings yet
- ENDOCRINOLOGY ReportDocument16 pagesENDOCRINOLOGY ReportConlene PontejoNo ratings yet
- Case Study Cushing Syndrome 1Document5 pagesCase Study Cushing Syndrome 1Selena Marie100% (1)
- Randomized Control Trial To Real World Evidence of Ultra Long Acting Insulin Basal Glargine-300: What Big Clinical Data Teaching Us ?Document27 pagesRandomized Control Trial To Real World Evidence of Ultra Long Acting Insulin Basal Glargine-300: What Big Clinical Data Teaching Us ?Yaumil FitriNo ratings yet
- Dry Lab Exercise 4 Aktivity 2Document4 pagesDry Lab Exercise 4 Aktivity 2ZULBIKAR SETYA DHARMANo ratings yet
- Amenorrhea: An Approach To Diagnosis and ManagementDocument8 pagesAmenorrhea: An Approach To Diagnosis and ManagementtapayanaNo ratings yet
- Management of Congenital HypogonadotropicDocument42 pagesManagement of Congenital HypogonadotropicAgung SentosaNo ratings yet
- Hyperthyroidism: Div. Endokrin-Metabolisme Dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM MedanDocument46 pagesHyperthyroidism: Div. Endokrin-Metabolisme Dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM MedanDaniel IvanNo ratings yet
- Endocrinology OSCEDocument17 pagesEndocrinology OSCEswamy rao100% (1)
- Final: A45 - Gyanpur Cc-Ajeet Pandey NILL, Tahsilroad, District Hospital, Tahsil Gyanpur GYANPUR 221304Document2 pagesFinal: A45 - Gyanpur Cc-Ajeet Pandey NILL, Tahsilroad, District Hospital, Tahsil Gyanpur GYANPUR 221304UughuuNo ratings yet
- Perbedaan Kadar Asam Urat Pada Wanita Perimenopause Dan MenopauseDocument4 pagesPerbedaan Kadar Asam Urat Pada Wanita Perimenopause Dan Menopauseria kartini panjaitanNo ratings yet
- Endocrine System 1: Overview of The Endocrine System and HormonesDocument5 pagesEndocrine System 1: Overview of The Endocrine System and HormonesDance RangersNo ratings yet
- Agappe I1000 Clia - CPT NewDocument2 pagesAgappe I1000 Clia - CPT Newsrikanth7210No ratings yet
- Addison's Disease (Primary Adrenal Insufficiency)Document5 pagesAddison's Disease (Primary Adrenal Insufficiency)sunnnydayNo ratings yet
- Guias Thyroid 2012Document43 pagesGuias Thyroid 2012JoseAbdalaNo ratings yet
- Diabetes MellitusDocument70 pagesDiabetes MellitusAizaz AhmadNo ratings yet
- Canine Diabetes MellitusDocument6 pagesCanine Diabetes MellitusLauura Cristina BarriosNo ratings yet
- Development in Childhood PDFDocument2 pagesDevelopment in Childhood PDFraz2000No ratings yet
- 注册信息汇总表 Ce 2023.04Document1 page注册信息汇总表 Ce 2023.04hzfrankshanNo ratings yet
- 3current Evaluation of Amenorrhea - A Committee OpinionDocument9 pages3current Evaluation of Amenorrhea - A Committee Opinionjorge nnNo ratings yet
- Study of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)Document2 pagesStudy of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)IJAR JOURNALNo ratings yet
- Hormone Replacement Therapy: A Study of Women's Knowledge and AttitudesDocument7 pagesHormone Replacement Therapy: A Study of Women's Knowledge and AttitudesArpita ArpitaNo ratings yet
- Royal Alexandra Hospital For Children: Policy & Procedures ManualDocument73 pagesRoyal Alexandra Hospital For Children: Policy & Procedures ManualDivya NarayanNo ratings yet
- Cushing SyndromDocument12 pagesCushing SyndromIka AnisaNo ratings yet
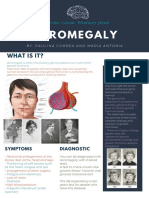
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- 22.chemical Coordination and IntegrationDocument32 pages22.chemical Coordination and Integrationg13070% (1)
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet