Download as docx, pdf, or txt
You might also like
- Alberta Drivers HandbookDocument235 pagesAlberta Drivers HandbookHarsheen Kaur100% (1)
- IOSA ManualDocument702 pagesIOSA ManualManisha YuukiNo ratings yet
- KRA For HR ExecutiveDocument4 pagesKRA For HR ExecutiveChintan Shet100% (5)
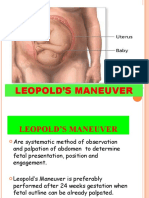
- Mechanism of Normal LabourDocument42 pagesMechanism of Normal Labourjayapreethiravi94% (18)
- DocumentsDocument22 pagesDocumentsDivina D Galvez-BeronioNo ratings yet
- Breech PresentationDocument122 pagesBreech Presentationlieynna4996100% (1)
- Breech Delivery TechniqueDocument39 pagesBreech Delivery Techniquevan016_bunny100% (1)
- Breech FinalDocument51 pagesBreech FinalSwati ThathiraNo ratings yet
- How To Perform LeopoldDocument5 pagesHow To Perform LeopoldChared Lumba100% (3)
- Breech Delivery: Department of Gynaecology and Obstetrics R.G.Kar Medical CollegeDocument16 pagesBreech Delivery: Department of Gynaecology and Obstetrics R.G.Kar Medical CollegeSourav ChowdhuryNo ratings yet
- Mal PresentationDocument5 pagesMal Presentationhomework8589No ratings yet
- Leopold's Maneuver and 7 Cardinal MovementsDocument5 pagesLeopold's Maneuver and 7 Cardinal MovementsMikaela Gabrielle GERALINo ratings yet
- Conduct of Normal Labor and DeliveryDocument141 pagesConduct of Normal Labor and DeliveryRea Dominique CabanillaNo ratings yet
- Leopold's Maneuvers - PPTMDocument26 pagesLeopold's Maneuvers - PPTMDencel BarramedaNo ratings yet
- Mechanism of Abnormal Labour Breech 500LDocument4 pagesMechanism of Abnormal Labour Breech 500Lm jNo ratings yet
- New Ballard ScoreDocument5 pagesNew Ballard ScoreNaviin Gopi Kumar100% (1)
- Clinics Breech Delivery - MVNDocument31 pagesClinics Breech Delivery - MVNDoc AchondoNo ratings yet
- Leopold's ManeuverDocument22 pagesLeopold's ManeuverArlene Cerdeña Salceda100% (1)
- MalpresentationDocument19 pagesMalpresentationHanelie B. AldeaNo ratings yet
- ACFrOgBEGtOKqayqBNgWl7cRDozoAC7IIFrbJTuLoEqpdwn0pt Y4EGdcsgvfe9-0aZjQwd7EmTj3i3ibCKP1RvPW p1mB7cX Ubs8y 3Y1pfDKGb7HyWcIAqo5tJB62FaTOkEsx8QBbZg7u3b-CDocument27 pagesACFrOgBEGtOKqayqBNgWl7cRDozoAC7IIFrbJTuLoEqpdwn0pt Y4EGdcsgvfe9-0aZjQwd7EmTj3i3ibCKP1RvPW p1mB7cX Ubs8y 3Y1pfDKGb7HyWcIAqo5tJB62FaTOkEsx8QBbZg7u3b-CDustin Dela CruzNo ratings yet
- Mechanism of LabourDocument18 pagesMechanism of LabournamithaNo ratings yet
- Breech 2Document67 pagesBreech 2Kiprotich Titus NgetichNo ratings yet
- Mechanism of Normal Labor and PartographDocument50 pagesMechanism of Normal Labor and PartographpatsilwalNo ratings yet
- Malposition & Malpresentation: Ahmad MakhloufDocument72 pagesMalposition & Malpresentation: Ahmad Makhloufjssamc prasootitantraNo ratings yet
- Breech 17Document27 pagesBreech 17Trevor Uratel100% (1)
- Malpresentation and Malposition - BreechDocument21 pagesMalpresentation and Malposition - BreechNishaThakuri100% (1)
- CPP Breech DeliveryDocument9 pagesCPP Breech Deliveryjay bristolNo ratings yet
- Breech Presentation: Nur Azwani Binti Mamat Nur Alya Inani Binti RosniDocument14 pagesBreech Presentation: Nur Azwani Binti Mamat Nur Alya Inani Binti RosniLiEya EyNani KAizenNo ratings yet
- Mechanisms of Normal LaborDocument5 pagesMechanisms of Normal LaborbasimahNo ratings yet
- Breech Presentation 1Document33 pagesBreech Presentation 1Cristina Stanlee100% (1)
- Fetal MalpresentationDocument33 pagesFetal MalpresentationMichael Angelo Seña100% (1)
- Dystocia: DR - Selvaraj, Chinnasamy M.DDocument54 pagesDystocia: DR - Selvaraj, Chinnasamy M.DSelvaraj ChinnasamyNo ratings yet
- Ballard ScoreDocument7 pagesBallard ScoreAndre OpaNo ratings yet
- Breech DeliveryDocument6 pagesBreech DeliveryNyoman TapayanaNo ratings yet
- Second Stage of Labour SubmissionDocument22 pagesSecond Stage of Labour SubmissionSavita HanamsagarNo ratings yet
- FAULTY FETAL DI-WPS OfficeDocument8 pagesFAULTY FETAL DI-WPS OfficeDr. Vinay VijayakumarNo ratings yet
- Breech PresentationDocument46 pagesBreech PresentationJOY SANDHYA JOSEPH (RA2123003011002)No ratings yet
- Braxton Hicks Contractions or False Labor: ST STDocument10 pagesBraxton Hicks Contractions or False Labor: ST STKristine Jade OdtujanNo ratings yet
- Nursing Care of The Client With High-Risk Labor & DeliveryDocument10 pagesNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanNo ratings yet
- Breech Presentation June 2023Document59 pagesBreech Presentation June 2023Imbodi TiliyeNo ratings yet
- Labor and DeliveryDocument4 pagesLabor and DeliveryJinky Teneza100% (1)
- Brow PresentationDocument38 pagesBrow PresentationAnnapurna DangetiNo ratings yet
- LEOPOLD's MANEUVER RATIONALEDocument3 pagesLEOPOLD's MANEUVER RATIONALEAngela AquisapNo ratings yet
- Breech Presentation-Pritiss Nair Group 2Document45 pagesBreech Presentation-Pritiss Nair Group 2asmeralda99No ratings yet
- Bien Powerpoint Demo PresentationDocument58 pagesBien Powerpoint Demo PresentationbienNo ratings yet
- Mal Presentations ObgDocument20 pagesMal Presentations ObgMonika shankarNo ratings yet
- Leopold's Maneuver.2Document23 pagesLeopold's Maneuver.2Ces Aria100% (1)
- 6.1 Notes On Handling and Assisting CareDocument7 pages6.1 Notes On Handling and Assisting CarePasay Trisha Faye Y.No ratings yet
- Malpresentations: Liji Raichel Kurian Dept of OBGDocument41 pagesMalpresentations: Liji Raichel Kurian Dept of OBGliji raichel kurian100% (1)
- Topic # 1 Leopold's ManueverDocument39 pagesTopic # 1 Leopold's ManueverJayrelle D. SafranNo ratings yet
- Breech-Presentation (2) - 1Document30 pagesBreech-Presentation (2) - 1ahmed shorshNo ratings yet
- Occipito PosteriorpositionDocument7 pagesOccipito PosteriorpositionNishaThakuriNo ratings yet
- Transverse LieDocument7 pagesTransverse LieKezia JessicaNo ratings yet
- Anatomy and Physiology of NSDDocument4 pagesAnatomy and Physiology of NSDkyle otedaNo ratings yet
- Mechanism of Normal LaborDocument12 pagesMechanism of Normal LaborImation Data100% (1)
- Obstetrics: The Fetus-in-Utero (Lie, Presentation & Position)Document28 pagesObstetrics: The Fetus-in-Utero (Lie, Presentation & Position)Sanjeet SahNo ratings yet
- Rle LeopoldsDocument34 pagesRle LeopoldsAngelica Fontanilla Bajo RNNo ratings yet
- Breech PresentationDocument62 pagesBreech Presentationmishka.dubtsovNo ratings yet
- 4 P's of Labor and Birth: Presented By: Ana Laurice R. Nastor & Nerissa N. Natata RLE II-7.2Document56 pages4 P's of Labor and Birth: Presented By: Ana Laurice R. Nastor & Nerissa N. Natata RLE II-7.2steffiNo ratings yet
- Fetal Malpresentation and Malposition - LecturioDocument17 pagesFetal Malpresentation and Malposition - LecturiomeddcrossNo ratings yet
- Interfacial PhenomenaDocument75 pagesInterfacial Phenomenanejaabera12No ratings yet
- Regional CQM Supervisor - Wuhan Fiberhome International Technologies Phils., Inc. - 10502036 - JobStreetDocument4 pagesRegional CQM Supervisor - Wuhan Fiberhome International Technologies Phils., Inc. - 10502036 - JobStreetJabNo ratings yet
- A2 - 2 - Health & Fitness (ES)Document23 pagesA2 - 2 - Health & Fitness (ES)tomasgomisNo ratings yet
- Bread Maker Recipe 1 PDFDocument16 pagesBread Maker Recipe 1 PDFSopheak ThapNo ratings yet
- Automated Coiled Tubing Integrity Monitoring (ACIM) : TechnologyDocument4 pagesAutomated Coiled Tubing Integrity Monitoring (ACIM) : TechnologyArgonauta_navegadorNo ratings yet
- Competitors Analysis 1Document2 pagesCompetitors Analysis 1rajaroma45No ratings yet
- AEG JSA 107 Angle GrinderDocument3 pagesAEG JSA 107 Angle GrinderSai PrasathNo ratings yet
- Effect of Mulch On Soil TemperatureDocument11 pagesEffect of Mulch On Soil TemperatureEzeugo NelsonNo ratings yet
- Phytochemical Screening and Antimicrobial Assay of Various SeedsDocument9 pagesPhytochemical Screening and Antimicrobial Assay of Various SeedsWendy FXNo ratings yet
- Business Ethics ANSWERSDocument3 pagesBusiness Ethics ANSWERSMỹ HàNo ratings yet
- STSDocument4 pagesSTSMGPagaduanNo ratings yet
- 9137-AN/898: Airport Services ManualDocument170 pages9137-AN/898: Airport Services ManualAndry NapitupuluNo ratings yet
- ISO 14001-Claus-4.4.1Document2 pagesISO 14001-Claus-4.4.1Navnath TamhaneNo ratings yet
- Discrimination (Different Type)Document2 pagesDiscrimination (Different Type)Jep DVNo ratings yet
- Macro Curriculum Changes 2023 Part 2Document6 pagesMacro Curriculum Changes 2023 Part 2Al VelNo ratings yet
- Sda Church History 1863-1888Document17 pagesSda Church History 1863-1888Tawonga RushambwaNo ratings yet
- MJMHS 0034Document3 pagesMJMHS 0034Alan MarshallNo ratings yet
- Experiment #02 To Verify The Theoretical Expression For The Force Exerted by Jet Striking Normally On The Flat Plate (Impact of Jet)Document2 pagesExperiment #02 To Verify The Theoretical Expression For The Force Exerted by Jet Striking Normally On The Flat Plate (Impact of Jet)Mir Masood ShahNo ratings yet
- Oral Squamous Cell Carcinoma (OSCC) : Homam Mansour Abo Orabi 201814250Document15 pagesOral Squamous Cell Carcinoma (OSCC) : Homam Mansour Abo Orabi 201814250Homam MANo ratings yet
- A9810029 enDocument3 pagesA9810029 enAnonymous nIcSGEwNo ratings yet
- Otec SeminarDocument21 pagesOtec SeminarAbhishekSuman80% (5)
- Weflo 3129 Cast Iron Gate Valve Flanged Table EDocument1 pageWeflo 3129 Cast Iron Gate Valve Flanged Table EMOHD HAIDARNo ratings yet
- 38 Fault Codes Tachograph MID 220Document34 pages38 Fault Codes Tachograph MID 220Lazuardhitya oktananda100% (1)
- Springfield Building Department Inspectional Services Notice of ViolationsDocument6 pagesSpringfield Building Department Inspectional Services Notice of ViolationsThe Republican/MassLive.comNo ratings yet
- Desain Pengembangan Karir FTDocument39 pagesDesain Pengembangan Karir FTasma hayatiNo ratings yet
- Bahasa Inggris Soal LatihanDocument38 pagesBahasa Inggris Soal LatihanIndah PramantiNo ratings yet