Download as pdf or txt
You might also like
- Hospital DischargeDocument15 pagesHospital DischargePrernaBhasinNo ratings yet
- Comprehensive Geriatric AssessmentDocument25 pagesComprehensive Geriatric Assessmentsantosestrella100% (6)
- PAPER (ENG) - (Shanahan T., Logemann J., Et Al., 1992 USA) Chin-Down Posture Effect On Aspiration in Dysphagic PatientsDocument5 pagesPAPER (ENG) - (Shanahan T., Logemann J., Et Al., 1992 USA) Chin-Down Posture Effect On Aspiration in Dysphagic PatientsAldo Hip NaranjoNo ratings yet
- Assessment of Oropharyngeal Dysphagia in Patients With Parkinson Disease: Use of UltrasonographyDocument7 pagesAssessment of Oropharyngeal Dysphagia in Patients With Parkinson Disease: Use of UltrasonographyTri Eka JuliantoNo ratings yet
- Incidence of Developing Contralateral M Enie're's Disease in Patients Undergoing Transmastoid Labyrinthectomy For Unilateral M Enie're's DiseaseDocument4 pagesIncidence of Developing Contralateral M Enie're's Disease in Patients Undergoing Transmastoid Labyrinthectomy For Unilateral M Enie're's DiseaseNoviTrianaNo ratings yet
- Pharyngeal Area Changes in Parkinson's Disease and Its Effect On Swallowing Safety, Efficiency, and KinematicsDocument10 pagesPharyngeal Area Changes in Parkinson's Disease and Its Effect On Swallowing Safety, Efficiency, and Kinematicskhadidja BOUTOUILNo ratings yet
- Análise Ultrassonográfica Da Elevação Laríngea Durante A Deglutição PDFDocument5 pagesAnálise Ultrassonográfica Da Elevação Laríngea Durante A Deglutição PDFGiovanna MartinsNo ratings yet
- FulltextDocument7 pagesFulltextNicolas CruzNo ratings yet
- Avaliação Ultrassonográfica Quantitativa Do Deslocamento Do Osso Hioide Durante A Deglutição Após Tireoidectomia PDFDocument11 pagesAvaliação Ultrassonográfica Quantitativa Do Deslocamento Do Osso Hioide Durante A Deglutição Após Tireoidectomia PDFGiovanna MartinsNo ratings yet
- HHS Public Access: Effects of Chin-Up Posture On The Sequence of Swallowing EventsDocument30 pagesHHS Public Access: Effects of Chin-Up Posture On The Sequence of Swallowing EventsMarcia SantanaNo ratings yet
- Relationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Young Chinese ChildrenDocument7 pagesRelationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Young Chinese ChildrenTanya HernandezNo ratings yet
- Aboudara2009 PDFDocument12 pagesAboudara2009 PDFYsl OrtodonciaNo ratings yet
- Otolaryngol - Head Neck Surg - 2010 - Aynehchi - Systematic Review of Laryngeal Reinnervation TechniquesDocument11 pagesOtolaryngol - Head Neck Surg - 2010 - Aynehchi - Systematic Review of Laryngeal Reinnervation TechniquesAlejandra BenavidezNo ratings yet
- Aijcr 2011 04 021Document6 pagesAijcr 2011 04 021ishu sNo ratings yet
- Effect of HeadDocument6 pagesEffect of HeadSwathi GeethaNo ratings yet
- Stewart 2004Document8 pagesStewart 2004César VidezNo ratings yet
- The Utility of Pitch Elevation in The Evaluation of Oropharyngeal Dysphagia - Preliminary FindingsDocument8 pagesThe Utility of Pitch Elevation in The Evaluation of Oropharyngeal Dysphagia - Preliminary FindingsESTEFANIA GEOVANNA MEJIA MACASNo ratings yet
- 10 Intl J Lang Comm Disor - 2019 - Park - Effect of Effortful Swallowing Training On Tongue Strength and OropharyngealDocument6 pages10 Intl J Lang Comm Disor - 2019 - Park - Effect of Effortful Swallowing Training On Tongue Strength and OropharyngealAndressa AraújoNo ratings yet
- Expansion OrtodoncicaDocument5 pagesExpansion OrtodoncicaRosa Natalia Muente RojasNo ratings yet
- 1 IiomainDocument6 pages1 IiomainyandaputriNo ratings yet
- Effectiveness of Brandt Daroff, Semont and Epley ManeuversDocument8 pagesEffectiveness of Brandt Daroff, Semont and Epley ManeuversNestri PrabandaniNo ratings yet
- Oropharyngeal Dysphagia HNCDocument15 pagesOropharyngeal Dysphagia HNCKhumaira SantaNo ratings yet
- PARS Reader's Digest - Feb 2013Document12 pagesPARS Reader's Digest - Feb 2013info8673No ratings yet
- Otolaryngology Head and Neck Surgery 2014 Namin P76 7Document3 pagesOtolaryngology Head and Neck Surgery 2014 Namin P76 76mqpjqh2vqNo ratings yet
- Relationships of Vertical Facial Pattern, Natural Head Position and Craniocervical Posture in Young Chinese ChildrenDocument8 pagesRelationships of Vertical Facial Pattern, Natural Head Position and Craniocervical Posture in Young Chinese ChildrenambersNo ratings yet
- Journal of Clinical Anesthesia: Original ContributionDocument6 pagesJournal of Clinical Anesthesia: Original ContributionzaimmuhtarNo ratings yet
- Tto Crup NatureDocument7 pagesTto Crup NatureCarolina Mora RuedaNo ratings yet
- 2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDocument7 pages2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDimitris RodriguezNo ratings yet
- Parapharyngeal Abscess in Children - Five Year Retrospective StudyDocument5 pagesParapharyngeal Abscess in Children - Five Year Retrospective StudyciciNo ratings yet
- Otolaryngol Head Neck Surg 2019 160 6 955-964Document10 pagesOtolaryngol Head Neck Surg 2019 160 6 955-964baltazarottonelloNo ratings yet
- Neck Abcess in ChildrenDocument6 pagesNeck Abcess in ChildrenNandaNo ratings yet
- Prevalence of Malocclusion in Children With Sleep Disordered BreathingDocument4 pagesPrevalence of Malocclusion in Children With Sleep Disordered BreathingMu'taz ArmanNo ratings yet
- Original Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialDocument9 pagesOriginal Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialAnonymous iM2totBrNo ratings yet
- Effects of Tracheostomy Tube On SwallowingDocument21 pagesEffects of Tracheostomy Tube On SwallowingPaola A. MartinezNo ratings yet
- Oclusion 1Document10 pagesOclusion 1Itzel MarquezNo ratings yet
- Cephalometric Assessment in OSADocument10 pagesCephalometric Assessment in OSAAkanksha SrivastavaNo ratings yet
- Prevention of Dislocation of The Hip in Children With Cerebral PalsyDocument7 pagesPrevention of Dislocation of The Hip in Children With Cerebral PalsymiguelpaillalefgutierrezNo ratings yet
- An Evaluation of Two Different Mandibular Advancement Devices On Craniofacial Characteristics and Upper Airway Dimensions of Chinese Adult Obstructive Sleep Apnea PatientsDocument7 pagesAn Evaluation of Two Different Mandibular Advancement Devices On Craniofacial Characteristics and Upper Airway Dimensions of Chinese Adult Obstructive Sleep Apnea PatientscemNo ratings yet
- BFA FullDocument9 pagesBFA Fullhistory APNo ratings yet
- Predictor de Residuos Faringeos en ParkinsonDocument11 pagesPredictor de Residuos Faringeos en Parkinsoncami gonzalezNo ratings yet
- Kim 2015Document4 pagesKim 2015ruthameliapNo ratings yet
- Correlation Between Laryngeal Sensitivity and Penetration/ Aspiration After StrokeDocument6 pagesCorrelation Between Laryngeal Sensitivity and Penetration/ Aspiration After StrokeRodrigo Felipe Toro MellaNo ratings yet
- Evaluación de TosDocument8 pagesEvaluación de TosCarolina CelisNo ratings yet
- Martin Harris Et Al 2021 The Modified Barium Swallow Study For Oropharyngeal Dysphagia Recommendations From AnDocument10 pagesMartin Harris Et Al 2021 The Modified Barium Swallow Study For Oropharyngeal Dysphagia Recommendations From AnCARLA ARACELI GÓMEZNo ratings yet
- Respiratory Swallow Pattern Following Total LaryngectomyDocument7 pagesRespiratory Swallow Pattern Following Total Laryngectomykhadidja BOUTOUILNo ratings yet
- Xu 2014Document8 pagesXu 2014Nadya Novia SariNo ratings yet
- Cephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionDocument6 pagesCephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionGabriela MuñozNo ratings yet
- Ijcm 2014071513394601 PDFDocument9 pagesIjcm 2014071513394601 PDFnurulrezqiaNo ratings yet
- Validity and Reliability of The Eating Assessment Tool (EAT-10) 2003Document6 pagesValidity and Reliability of The Eating Assessment Tool (EAT-10) 2003draanalordonezv1991No ratings yet
- Rapid Maxillary Expansion Before and After Adenotonsillectomy in Children With Obstructive Sleep ApneaDocument8 pagesRapid Maxillary Expansion Before and After Adenotonsillectomy in Children With Obstructive Sleep ApneaDiana Lozano OlveraNo ratings yet
- Puccinelli 2019Document8 pagesPuccinelli 2019RathavishwarajNo ratings yet
- 455 2014 Article 9580Document10 pages455 2014 Article 9580Ailin Vejar GaticaNo ratings yet
- Gag Reflex and Dysphagia: Steven Leder, PHDDocument4 pagesGag Reflex and Dysphagia: Steven Leder, PHDshraddhaNo ratings yet
- A Clinical Study of Intussusception in ChildrenDocument18 pagesA Clinical Study of Intussusception in ChildrenIJAR JOURNALNo ratings yet
- Otorhinolaryngology: Dysphagia in Patients With Moderate and Severe Obstructive Sleep ApneaDocument6 pagesOtorhinolaryngology: Dysphagia in Patients With Moderate and Severe Obstructive Sleep Apneadr Rizaldi AbesyNo ratings yet
- 3 2022 Phagia in Solid Tumors Outside The Head, Neck or Upper GI Tract - Clinical CharacteristicsDocument9 pages3 2022 Phagia in Solid Tumors Outside The Head, Neck or Upper GI Tract - Clinical CharacteristicsmeeNo ratings yet
- Protocol Anwar 3Document6 pagesProtocol Anwar 3abofares4ever88No ratings yet
- Journal Pone 0193913Document10 pagesJournal Pone 0193913tiara nadya putriandaNo ratings yet
- Tinnitus JournalDocument4 pagesTinnitus JournalSathvika BNo ratings yet
- Jamaotolaryngology Lee 2020 Oi 190100Document7 pagesJamaotolaryngology Lee 2020 Oi 190100LeonNo ratings yet
- Coordes 2017Document21 pagesCoordes 2017nunisulastri1998No ratings yet
- NCP Nutrition1Document4 pagesNCP Nutrition1java_biscocho1229100% (1)
- Eosinophilic Granulomatosis With Polyangiitis Complete ArticleDocument7 pagesEosinophilic Granulomatosis With Polyangiitis Complete ArticleVeronicaNo ratings yet
- Aminoleban Drug StudyDocument1 pageAminoleban Drug StudyNajmah Saaban100% (1)
- Answer Key Intraboard BDocument14 pagesAnswer Key Intraboard BJonas Marvin Anaque100% (3)
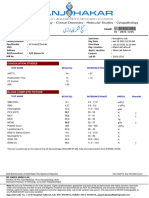
- REport BlooodDocument3 pagesREport Bloooddivid joneNo ratings yet
- 1 SMDocument6 pages1 SMedi_wsNo ratings yet
- Dental EssayDocument3 pagesDental Essayvaleriana calaniNo ratings yet
- NMC LICENSURE - Care PlanDocument2 pagesNMC LICENSURE - Care PlanAlukuba AwalNo ratings yet
- Patient'S Record: University of Northern PhilippinesDocument21 pagesPatient'S Record: University of Northern PhilippinesCezanne CruzNo ratings yet
- Basic Implant SurgeryDocument7 pagesBasic Implant SurgeryDr.Ankur Gupta100% (1)
- Technical Notes Community Health NursingDocument8 pagesTechnical Notes Community Health NursingMary JoyNo ratings yet
- Mitral Valve ProlapseDocument7 pagesMitral Valve ProlapsehracakNo ratings yet
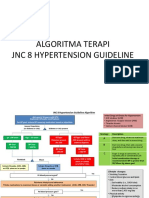
- 2 Algoritma HT JNC 8Document3 pages2 Algoritma HT JNC 8Nais Maghfiroh100% (1)
- PRISMA 2009 ChecklistDocument7 pagesPRISMA 2009 ChecklistRezky PutriNo ratings yet
- CSBP Post Stroke Checklist ENDocument2 pagesCSBP Post Stroke Checklist ENEduardo BessoloNo ratings yet
- DEFIBRILLATORDocument12 pagesDEFIBRILLATORRajath N Gowda 1SG18EE062No ratings yet
- 5 6212862165817229365Document116 pages5 6212862165817229365badhra100% (1)
- Clinical Pathway ACSDocument7 pagesClinical Pathway ACSherrerachaimNo ratings yet
- Ebook: Bioactive Dental Materials: The Future Is NowDocument7 pagesEbook: Bioactive Dental Materials: The Future Is NowAli FaridiNo ratings yet
- Pathophysiologic, Translational and Clinical Aspects of Postoperative Ileus - A ReviewDocument15 pagesPathophysiologic, Translational and Clinical Aspects of Postoperative Ileus - A ReviewRebecca BlackburnNo ratings yet
- Rule 11DDDocument3 pagesRule 11DDIonut ColcearNo ratings yet
- Intake FormDocument4 pagesIntake Formapi-217218803No ratings yet
- Nursing History and Assessment: A. IntroductionDocument18 pagesNursing History and Assessment: A. IntroductionAmanda ScarletNo ratings yet
- A Rare Case of Acute Abdomen: DR - Rajeev Thilak C, DR - Ramadoss.P, DR - Ameesh Izath, DR - Christianne SandhyaDocument3 pagesA Rare Case of Acute Abdomen: DR - Rajeev Thilak C, DR - Ramadoss.P, DR - Ameesh Izath, DR - Christianne SandhyaRajeev ThilakNo ratings yet
- 782Document20 pages782Aarathi raoNo ratings yet
- Cerebellopontine Angle Tumors: Guide:Dr Suchitra Dashjohn Speaker: DR Madhusmita BeheraDocument20 pagesCerebellopontine Angle Tumors: Guide:Dr Suchitra Dashjohn Speaker: DR Madhusmita Beheraasish753905No ratings yet
- ALCOHOL Pharmacology: Samuel Murano. Dept. of PharmacologyDocument23 pagesALCOHOL Pharmacology: Samuel Murano. Dept. of PharmacologyGideon K. MutaiNo ratings yet
- Z Code (Z00 Z99) Coding and GuidelinesDocument9 pagesZ Code (Z00 Z99) Coding and GuidelinesMutiara UtamiNo ratings yet