Download as pdf or txt
You might also like
- Autonomic Nervous System Drugs Simple Complement Type QuestionsDocument11 pagesAutonomic Nervous System Drugs Simple Complement Type QuestionsIrina Panciu Stefan100% (1)
- Cheat Sheet Integumentary SystemDocument4 pagesCheat Sheet Integumentary SystemLisa RetbergNo ratings yet
- Chapter 4. AnaphyDocument2 pagesChapter 4. AnaphyNathalia100% (1)
- Presby ManualDocument432 pagesPresby Manualpoddata100% (3)
- BATES CH 4 SkinDocument2 pagesBATES CH 4 SkinAngelica Mae Dela CruzNo ratings yet
- Yoga For Skin Diseases Anna MayerDocument22 pagesYoga For Skin Diseases Anna Mayerjaideep negi100% (1)
- Skin Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSkin Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- FNCP CommunityDocument4 pagesFNCP CommunityWendy EscalanteNo ratings yet
- 1 - Initial LesionsDocument73 pages1 - Initial LesionsAhmed RamzyNo ratings yet
- Ch. 10 Skin, Hair and Nails - Bickley and BatesDocument2 pagesCh. 10 Skin, Hair and Nails - Bickley and BatesfufuNo ratings yet
- 2016 DermTerms & Dx-1Document53 pages2016 DermTerms & Dx-1vivekNo ratings yet
- Presentation1 DermoDocument12 pagesPresentation1 DermotannuNo ratings yet
- Skin Examination 1Document17 pagesSkin Examination 1Daffa AmaliaNo ratings yet
- Chapter 4: Examination of The Skin, Coat and Associated StructuresDocument19 pagesChapter 4: Examination of The Skin, Coat and Associated StructuresZekarias GetachewNo ratings yet
- Dermatology NotesDocument59 pagesDermatology NotesAbdullah Matar Badran50% (2)
- Safari - 26 Mar 2023, 11:28 AMDocument1 pageSafari - 26 Mar 2023, 11:28 AMErza KabashiNo ratings yet
- EfloresensiDocument40 pagesEfloresensimariamunsriNo ratings yet
- Hers Hey Chapter 13 RevisedDocument10 pagesHers Hey Chapter 13 RevisedpoddataNo ratings yet
- Epidermis: Sebaceous/oil GlandsDocument3 pagesEpidermis: Sebaceous/oil GlandsDeepthi VallabhaneniNo ratings yet
- Dermatology+Review 2015 BATCH SOLVEDDocument7 pagesDermatology+Review 2015 BATCH SOLVEDMati ullah KhanNo ratings yet
- .Nursing in Dermatology. - 1700566942000Document53 pages.Nursing in Dermatology. - 1700566942000sagessenguegangNo ratings yet
- Nose Basal Cell CarcinomaDocument24 pagesNose Basal Cell CarcinomadianNo ratings yet
- Anatomy & Function of The SkinDocument9 pagesAnatomy & Function of The Skinعبدالعزيز احمد علي عتشNo ratings yet
- Derma 2023Document98 pagesDerma 2023mostafahabbeb2003No ratings yet
- Type of Skin Lesions: Dermatovenereology Departement / Division Dr. Moh. Hoesin Hospital / Medical Faculty UNSRI 2011Document35 pagesType of Skin Lesions: Dermatovenereology Departement / Division Dr. Moh. Hoesin Hospital / Medical Faculty UNSRI 2011Dipika Awinda0% (1)
- Act 12 (Zoolab 1C)Document5 pagesAct 12 (Zoolab 1C)莉安No ratings yet
- Tissue Integrity Outline Spring 2023Document25 pagesTissue Integrity Outline Spring 2023morganstorey0No ratings yet
- Dermatology TextbookDocument170 pagesDermatology TextbookHamo RefaatNo ratings yet
- PENDAHULUAN - EfloresensiDocument50 pagesPENDAHULUAN - EfloresensiSucitri NyomanNo ratings yet
- Integ. System Lesson 1Document7 pagesInteg. System Lesson 1Gabriela RamírezNo ratings yet
- Skin EXAM 2Document6 pagesSkin EXAM 2Madison100% (1)
- Assessment of Dermatological SkinPADAS FK UKDDocument24 pagesAssessment of Dermatological SkinPADAS FK UKDmichafuteNo ratings yet
- Integumentary Note 2 PDFDocument6 pagesIntegumentary Note 2 PDFMervi SarsonasNo ratings yet
- SKINDocument12 pagesSKINJaleah Gwyneth Fernandez EdullantesNo ratings yet
- Kulit-Perubahan Dasar Histologis PrintDocument38 pagesKulit-Perubahan Dasar Histologis PrintWirman RamadhanNo ratings yet
- Dermatology نظري PDFDocument46 pagesDermatology نظري PDFMedstudent 25No ratings yet
- Skin ShortDocument10 pagesSkin ShortKashar SaeedNo ratings yet
- CDI 22 Midterm Chapter 5 Injuries and WoundsDocument23 pagesCDI 22 Midterm Chapter 5 Injuries and WoundsFrank Davin BiraoNo ratings yet
- L1,2,3 - Intro, Anatomy, Language of Dermatologydr. Almontaser BellahDocument102 pagesL1,2,3 - Intro, Anatomy, Language of Dermatologydr. Almontaser BellahTOMMYNo ratings yet
- Biology 2: CH 5 - The Integumentary SystemDocument9 pagesBiology 2: CH 5 - The Integumentary SystemNicole Athena CruzNo ratings yet
- The Integumentary SystemDocument4 pagesThe Integumentary SystemKhan Hayudini SaliNo ratings yet
- The Integumentary System Activity No. 12Document4 pagesThe Integumentary System Activity No. 12Khan Hayudini SaliNo ratings yet
- Efflorescence of The Skin Lesions: Dr. M. Izazi HP, SP - KKDocument40 pagesEfflorescence of The Skin Lesions: Dr. M. Izazi HP, SP - KKSaputra Tri NopiantoNo ratings yet
- Scar & Keloids, Skin Grafting & Flaps: Dr. Kadhim Jawad Specialized General SurgeonDocument51 pagesScar & Keloids, Skin Grafting & Flaps: Dr. Kadhim Jawad Specialized General SurgeonNur Ain Che MudaNo ratings yet
- Skin Over View DermatologyDocument6 pagesSkin Over View DermatologyAlaa AhmedNo ratings yet
- Atopic Dermatitis Eczema NotesDocument12 pagesAtopic Dermatitis Eczema Notes돼끼빈No ratings yet
- CH 4take Home Test - Chapter 4 Integumentary SystemDocument5 pagesCH 4take Home Test - Chapter 4 Integumentary SystemKatieNo ratings yet
- WOUND CARE and BANDAGINGDocument9 pagesWOUND CARE and BANDAGINGJane BelvisNo ratings yet
- Chapter 6: Holes Anatomy and Physiology The Integumentary System (A Cutaneous Membrane)Document5 pagesChapter 6: Holes Anatomy and Physiology The Integumentary System (A Cutaneous Membrane)ccami709No ratings yet
- GMS511Document29 pagesGMS511Mahmoud NafeaNo ratings yet
- Sistem Integumentum 2Document19 pagesSistem Integumentum 2Andrianus SudarmonoNo ratings yet
- Derma OSCEDocument3 pagesDerma OSCEUsama El BazNo ratings yet
- Kuliah Sindrom Rabu 19112008.Document65 pagesKuliah Sindrom Rabu 19112008.Nurdiana RahmadaniNo ratings yet
- Derm 1Document19 pagesDerm 1tyleree3No ratings yet
- Integumentary System PhysioDocument53 pagesIntegumentary System PhysioMhykhaela CaparasNo ratings yet
- Dissertation LeucodermaDocument90 pagesDissertation LeucodermaRashmi Mishra100% (1)
- Pathology of The Integumentary System: References: Http://people - Upei.ca/hannaDocument22 pagesPathology of The Integumentary System: References: Http://people - Upei.ca/hannaLakshita Prajapati100% (1)
- National CollageDocument7 pagesNational CollageSolve App IssuesNo ratings yet
- Lect 4. Skin Hair and NailsDocument34 pagesLect 4. Skin Hair and Nailsdaniahisham05No ratings yet
- Dermatology 2010 2011Document28 pagesDermatology 2010 2011Qasim HaleimiNo ratings yet
- Skin cell, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSkin cell, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Patient Safety WHO CurriculumDocument46 pagesPatient Safety WHO CurriculumCalvin Chowder WittelsbachNo ratings yet
- 5 - HayashiItsuki 2012 TeenageSmokingWhatAre SmokingHealthEffectsPDocument38 pages5 - HayashiItsuki 2012 TeenageSmokingWhatAre SmokingHealthEffectsPlobont nataliaNo ratings yet
- Prediction of Fluid ResponsivenessDocument4 pagesPrediction of Fluid ResponsivenessSANTOSH KUMAR BHASKARNo ratings yet
- Jock ItchDocument16 pagesJock ItchMarcz Leogan BriagasNo ratings yet
- Chapter 11Document11 pagesChapter 11christian anchetaNo ratings yet
- Understanding Factual Reports (Human)Document4 pagesUnderstanding Factual Reports (Human)Rida Nadhira DNo ratings yet
- Application of Periodontal DressingDocument8 pagesApplication of Periodontal DressingSheena Mae OcampoNo ratings yet
- 1-Cpe-Black Book Simran Riya RitikDocument57 pages1-Cpe-Black Book Simran Riya RitikAnsh DabholkarNo ratings yet
- Systematic Reviews The Good, The Bad, and The Ugly - Yuan and Hunt (2009)Document7 pagesSystematic Reviews The Good, The Bad, and The Ugly - Yuan and Hunt (2009)felipeNo ratings yet
- Biliary Microlithiasis, Sludge, Crystals, MicrocrystallizationDocument6 pagesBiliary Microlithiasis, Sludge, Crystals, MicrocrystallizationniklukNo ratings yet
- UntitledDocument2 pagesUntitledPatricia DesireeNo ratings yet
- National Oral Health Policy VR 12 Revised Final PRINT VERSION 17 03 22 1Document44 pagesNational Oral Health Policy VR 12 Revised Final PRINT VERSION 17 03 22 1Adetayo AborisadeNo ratings yet
- Cesarean Delivery: Postoperative Issues - UpToDateDocument12 pagesCesarean Delivery: Postoperative Issues - UpToDateZurya UdayanaNo ratings yet
- Columbia Suicide Severity Rating Scale PDFDocument2 pagesColumbia Suicide Severity Rating Scale PDFAlejandroNo ratings yet
- Electrocardiogram ExaminationDocument13 pagesElectrocardiogram ExaminationayunisallehNo ratings yet
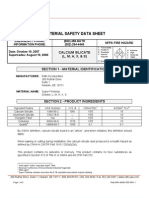
- Calcium Silicate MsdsDocument3 pagesCalcium Silicate MsdsHaniff RahimNo ratings yet
- Dealing With Listeria: A Guide For Food ManufacturersDocument8 pagesDealing With Listeria: A Guide For Food ManufacturersNicolas BenavidezNo ratings yet
- 39207618Document6 pages39207618api-301074100% (1)
- Q2 - A.Y. 21 22 - G2 - TOS and Periodical ExamDocument6 pagesQ2 - A.Y. 21 22 - G2 - TOS and Periodical ExamSher SherwinNo ratings yet
- Medical Nutrition Therapy A Case Study Approach 4Th Edition Nelms Solutions Manual Full Chapter PDFDocument29 pagesMedical Nutrition Therapy A Case Study Approach 4Th Edition Nelms Solutions Manual Full Chapter PDFStephanieMckayeqwr100% (13)
- American EskimosDocument21 pagesAmerican EskimosJorie RocoNo ratings yet
- Medical Form For XoDocument16 pagesMedical Form For XoKishan ChoudharyNo ratings yet
- Cocaine: What Does Cocaine Do?Document4 pagesCocaine: What Does Cocaine Do?pmmanickNo ratings yet
- Clinical-Trial AIIADocument6 pagesClinical-Trial AIIAkaushal ahirwarNo ratings yet
- Comparing The Calcium Content of Various Types of Milk: By: Rebecca AllenDocument26 pagesComparing The Calcium Content of Various Types of Milk: By: Rebecca AllenWan Ting ChiaNo ratings yet
- Lesson Plan For PortfolioDocument8 pagesLesson Plan For Portfolioapi-449507744No ratings yet
- Laghu Shankha Prakshalana - Final BnysDocument9 pagesLaghu Shankha Prakshalana - Final Bnyssureshbabubnys100% (1)
- Ass SciDocument87 pagesAss ScigheinbaNo ratings yet