Download as pdf or txt
You might also like
- Unit Test 1A: Are Big Colour Do Does Far Hair Is Long Many SizeDocument3 pagesUnit Test 1A: Are Big Colour Do Does Far Hair Is Long Many SizeБиба77% (13)
- Gom Whole ManualDocument305 pagesGom Whole Manualarakotoarson804100% (1)
- Hall Effect Lab ReportDocument6 pagesHall Effect Lab Reportruleevan25% (4)
- Icru 89 (229-260)Document32 pagesIcru 89 (229-260)Christian Ordoñez100% (1)
- Grade Ten: Science Exam NotesDocument10 pagesGrade Ten: Science Exam NotesLuna90% (21)
- Recruitment Strategies PDFDocument27 pagesRecruitment Strategies PDFjagatapsv100% (2)
- IGBRT (Image Guided Brachytherapy)Document39 pagesIGBRT (Image Guided Brachytherapy)nitinNo ratings yet
- SBRT Lung Single LesionDocument21 pagesSBRT Lung Single Lesionapi-592938880No ratings yet
- Varian Research ProposalDocument12 pagesVarian Research ProposalChandanaSanjeeNo ratings yet
- WPS Medicare IndexDocument14 pagesWPS Medicare IndexbkprodhNo ratings yet
- Lin Dega Ard 2016Document3 pagesLin Dega Ard 2016Kevin Bryan Aguirre UrviolaNo ratings yet
- Cervix (G) IGBT - DR Isha JaiswalDocument52 pagesCervix (G) IGBT - DR Isha JaiswalOshydh PojnNo ratings yet
- SBRT-VMAT Pulmón: DR Enrique CHAJON Département de Radiothérapie Centre Eugène Marquis Rennes, FranceDocument37 pagesSBRT-VMAT Pulmón: DR Enrique CHAJON Département de Radiothérapie Centre Eugène Marquis Rennes, FranceCristian Max Rau VargasNo ratings yet
- Estro RevisedDocument59 pagesEstro RevisedNishantNo ratings yet
- ICRU Report 89-79-88Document10 pagesICRU Report 89-79-88Sandra Johana Patino LeivaNo ratings yet
- 6746 13196 1 SMDocument44 pages6746 13196 1 SMTiyasNo ratings yet
- APBI Journal Club PowerPointDocument20 pagesAPBI Journal Club PowerPointRegan Ward HimeNo ratings yet
- Dr. Manoj GuptaDocument36 pagesDr. Manoj GuptaafshanNo ratings yet
- Consenso ESTRO Delimitación Vol Mama BraquiDocument6 pagesConsenso ESTRO Delimitación Vol Mama BraquiTriniNo ratings yet
- Basics of Anatomy, Planning, and Delivery: Gastrointestinal CancersDocument77 pagesBasics of Anatomy, Planning, and Delivery: Gastrointestinal CancersgammasharkNo ratings yet
- Final Rectal Cancer GEC ESTRO Handbook of BrachytherapyDocument14 pagesFinal Rectal Cancer GEC ESTRO Handbook of BrachytherapyRakesh JadhavNo ratings yet
- Abdomen X RayDocument4 pagesAbdomen X RaytimvrghsNo ratings yet
- Journal Club, GEC-ESTRODocument59 pagesJournal Club, GEC-ESTRODr. Ankita singhNo ratings yet
- Adaptative RT For Prostate Cancer Using KV CBCT - Jasper NijkampDocument8 pagesAdaptative RT For Prostate Cancer Using KV CBCT - Jasper NijkampMarcos sajcabunNo ratings yet
- Curriculum Vitae: Lulus Handayani, MDDocument31 pagesCurriculum Vitae: Lulus Handayani, MDpisangphoeNo ratings yet
- ICRU Report 89-89-104Document16 pagesICRU Report 89-89-104Sandra Johana Patino LeivaNo ratings yet
- Part 1 Week 9 - Volume DefinitionsDocument37 pagesPart 1 Week 9 - Volume DefinitionsdanNo ratings yet
- Synopsis For Delineation of CTV-T For Various Environments: General Principles of Target Contouring GTV-T ContouringDocument9 pagesSynopsis For Delineation of CTV-T For Various Environments: General Principles of Target Contouring GTV-T ContouringOnkologi Radiasi Angkatan 23No ratings yet
- User's Guide For The Synoptic MRI Report For Pre-Operative Staging of Rectal Cancer, 2015 - CCOMRIRectalStagingUserGuideDocument25 pagesUser's Guide For The Synoptic MRI Report For Pre-Operative Staging of Rectal Cancer, 2015 - CCOMRIRectalStagingUserGuideСергей СадовниковNo ratings yet
- Lung Radiotherapy General Guidelines CRT ServiceDocument3 pagesLung Radiotherapy General Guidelines CRT ServicebigskyNo ratings yet
- Z - Ding Cyberknife Vs LinacDocument26 pagesZ - Ding Cyberknife Vs Linacraheel252No ratings yet
- FS41 p34 Aptip Body OncologyDocument5 pagesFS41 p34 Aptip Body OncologybbkanilNo ratings yet
- Hepatobiliary Imaging by Multidetector Computed Tomography (MDCT)Document2 pagesHepatobiliary Imaging by Multidetector Computed Tomography (MDCT)Patwin ZadaNo ratings yet
- Austin Journal of Radiation Oncology and CancerDocument6 pagesAustin Journal of Radiation Oncology and CancerAustin Publishing GroupNo ratings yet
- NRG Protocol Radiation Therapy Template - GYN - 04-25-2018Document14 pagesNRG Protocol Radiation Therapy Template - GYN - 04-25-2018universeloNo ratings yet
- Partial Breast Irradiation: Dawn Radsek, RN Froedtert Hospital 9200 W Wisconsin Ave Milwaukee, WI 414/805-4440Document72 pagesPartial Breast Irradiation: Dawn Radsek, RN Froedtert Hospital 9200 W Wisconsin Ave Milwaukee, WI 414/805-4440Arun KUMAR.NNo ratings yet
- NRG Protocol Radiation Therapy Template - GYN - Endometrial Cancer - FinalDocument12 pagesNRG Protocol Radiation Therapy Template - GYN - Endometrial Cancer - FinalarifpharmjuNo ratings yet
- Ashith DBTDocument32 pagesAshith DBTAshith KumarNo ratings yet
- Structuri ProstataDocument70 pagesStructuri Prostatavlad_văluNo ratings yet
- Quality Assurance For Image-Guided Radiation Therapy Utilizing CT-basedDocument18 pagesQuality Assurance For Image-Guided Radiation Therapy Utilizing CT-based2016508吳翊晨No ratings yet
- Bone Marow Sparing - JCDRDocument5 pagesBone Marow Sparing - JCDRneha guptaNo ratings yet
- Kim 2010Document13 pagesKim 2010face bookNo ratings yet
- Cone Beam CT Guided Radiotherapy: Jan-Jakob SonkeDocument64 pagesCone Beam CT Guided Radiotherapy: Jan-Jakob Sonkebabba241276No ratings yet
- New Techniques in RadiotherapyDocument134 pagesNew Techniques in Radiotherapycrusader888100% (1)
- Manju Kiran.S: Presented ByDocument22 pagesManju Kiran.S: Presented ByManju KiranNo ratings yet
- IMRT Treatment Plans in Prostate Carcinoma: Comparison With 3DCRT. Dosimetric StudyDocument5 pagesIMRT Treatment Plans in Prostate Carcinoma: Comparison With 3DCRT. Dosimetric StudybambangsugandaNo ratings yet
- Bladder Cases - 2012Document9 pagesBladder Cases - 2012Fion TeoNo ratings yet
- Col Cancer StagingDocument6 pagesCol Cancer Stagingsalma2001No ratings yet
- Cervix Gec EstroDocument30 pagesCervix Gec EstroBunOg100% (1)
- Icru 50 & Icru 62Document43 pagesIcru 50 & Icru 62Eduardo Torres ZambranoNo ratings yet
- An Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTDocument9 pagesAn Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTBounegta AhmedNo ratings yet
- RSS-SBRT Lung Plan ReviewDocument32 pagesRSS-SBRT Lung Plan Reviewapi-602263051No ratings yet
- Radiotherapy Treatment Planning: Objectives, Formulations and Clinical ImplicationsDocument32 pagesRadiotherapy Treatment Planning: Objectives, Formulations and Clinical ImplicationsMed MedNo ratings yet
- Rectum - Nactrt vs. SCRTDocument68 pagesRectum - Nactrt vs. SCRTAkhil Thomas JacobNo ratings yet
- 3D Imrt VmatDocument13 pages3D Imrt VmatCristi Arias BadaNo ratings yet
- 03 GYN GEC ESTRO NovemberDocument14 pages03 GYN GEC ESTRO NovemberAndreas RonaldNo ratings yet
- Breast Cancer Early StageDocument89 pagesBreast Cancer Early StageSuranjan MaitraNo ratings yet
- CSingle Fraction Lung SABR Case Study James Cook (1)Document4 pagesCSingle Fraction Lung SABR Case Study James Cook (1)nabila.elsayed022No ratings yet
- Part 2 Week 9 - Treatment PlanningDocument50 pagesPart 2 Week 9 - Treatment PlanningdanNo ratings yet
- Curso - Volúmenes - ESTRO - Octubre - 2015 - Dra - ArenasDocument105 pagesCurso - Volúmenes - ESTRO - Octubre - 2015 - Dra - ArenasTriniNo ratings yet
- Shouldconebeam Computedtomographybe Routinelyobtainedinimplant Planning?Document17 pagesShouldconebeam Computedtomographybe Routinelyobtainedinimplant Planning?javiers45No ratings yet
- Computerized Medical Imaging and Graphics: Haiyun Liu, Xinde Chen, Zhijian He, Jun LiDocument5 pagesComputerized Medical Imaging and Graphics: Haiyun Liu, Xinde Chen, Zhijian He, Jun LiJuniosNo ratings yet
- Endoscopic Management of Colorectal T1(SM) CarcinomaFrom EverandEndoscopic Management of Colorectal T1(SM) CarcinomaShinji TanakaNo ratings yet
- Flow of DebateDocument2 pagesFlow of DebateIPQ PioneerNo ratings yet
- High School Delegate Country Worksheet 2014Document3 pagesHigh School Delegate Country Worksheet 2014IPQ PioneerNo ratings yet
- Points and MotionsDocument2 pagesPoints and MotionsIPQ PioneerNo ratings yet
- Flow of DebateDocument2 pagesFlow of DebateIPQ PioneerNo ratings yet
- MUN Student Handbook2020 (LATEST)Document21 pagesMUN Student Handbook2020 (LATEST)IPQ PioneerNo ratings yet
- SBRT Lung Setup Correction StrategiesDocument24 pagesSBRT Lung Setup Correction StrategiesIPQ PioneerNo ratings yet
- SRS Brain Setup Correction StrategiesDocument21 pagesSRS Brain Setup Correction StrategiesIPQ PioneerNo ratings yet
- Computer Network Unit-5 NotesDocument44 pagesComputer Network Unit-5 NotessuchitaNo ratings yet
- Malcolm Knox - The Wonder Lover (Extract)Document36 pagesMalcolm Knox - The Wonder Lover (Extract)Allen & UnwinNo ratings yet
- Hso422567 Issue2Document13 pagesHso422567 Issue2Александр ЩербаковNo ratings yet
- Method Statement For The Installation and Recovery of Temporary RoadwaysDocument15 pagesMethod Statement For The Installation and Recovery of Temporary Roadwaysandreipopa84No ratings yet
- Popular Mechanics - Volume 2 (1902)Document416 pagesPopular Mechanics - Volume 2 (1902)Cem AvciNo ratings yet
- 9-Engineering Data AnalysisDocument4 pages9-Engineering Data AnalysisJevan CalaqueNo ratings yet
- Hooverphonic Biography (2000)Document4 pagesHooverphonic Biography (2000)6980MulhollandDriveNo ratings yet
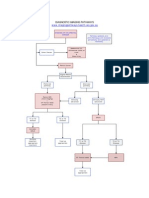
- West Bengal Health Recruitment Board: Documents Verification - Cum - Interview Call LetterDocument1 pageWest Bengal Health Recruitment Board: Documents Verification - Cum - Interview Call LetterSoumya BhattacharyaNo ratings yet
- NEC - 2017-10-26 - High Frequency TradingDocument53 pagesNEC - 2017-10-26 - High Frequency TradingAlexander GloyNo ratings yet
- Biochem TestADocument6 pagesBiochem TestAaby251188No ratings yet
- Reclaim Feeders BrochureDocument8 pagesReclaim Feeders Brochureelsieazcuna024No ratings yet
- Hardtop F15 PDFDocument4 pagesHardtop F15 PDFBiju_PottayilNo ratings yet
- 02 12 HLG AirfoilDocument7 pages02 12 HLG Airfoillojzemulec5966No ratings yet
- Manipulative Information and MediaDocument11 pagesManipulative Information and Mediamielin kaye villanuevaNo ratings yet
- Orgin of Biopotential and Its PropogationDocument11 pagesOrgin of Biopotential and Its PropogationAleeshaNo ratings yet
- Atlas of Obstetric UltrasoundDocument48 pagesAtlas of Obstetric UltrasoundSanchia Theresa100% (1)
- Template - Bullet CVDocument1 pageTemplate - Bullet CVVanny Achyani JoyowijoyoNo ratings yet
- Socio CulturalDocument12 pagesSocio CulturalVikas SharmaNo ratings yet
- IHITES - Volume 3 - Issue 4 - Pages 27-31Document6 pagesIHITES - Volume 3 - Issue 4 - Pages 27-31jonaNo ratings yet
- Kik0000001944 PDFDocument2 pagesKik0000001944 PDFSyahril Abdal SaudNo ratings yet
- Valerie Reuben v. US Airways Inc, 3rd Cir. (2012)Document5 pagesValerie Reuben v. US Airways Inc, 3rd Cir. (2012)Scribd Government DocsNo ratings yet
- The Efficient Strategies of Mcdonald'sDocument4 pagesThe Efficient Strategies of Mcdonald'sTabinda Shabbir KhanNo ratings yet
- Indian Oil Corporation LimitedDocument40 pagesIndian Oil Corporation LimitedAnu Jindal100% (1)
- Photography QuestionnaireDocument2 pagesPhotography Questionnaires2sarathNo ratings yet
- Recipes From The Epicurious Cookbook by Tanya Steel and The Editors of EpicuriousDocument11 pagesRecipes From The Epicurious Cookbook by Tanya Steel and The Editors of EpicuriousThe Recipe ClubNo ratings yet