Download as pdf or txt
You might also like
- Form - Bupa Claim FormDocument2 pagesForm - Bupa Claim FormJoe Sayavongsa100% (3)
- Ansi Bhma A156.40 2015 PDFDocument34 pagesAnsi Bhma A156.40 2015 PDFShawn DeolNo ratings yet
- CMS 1450 (UB 04) InstructionsDocument12 pagesCMS 1450 (UB 04) InstructionsKarna Palanivelu67% (3)
- HSTP II HMIS Hospital Heath Centre and Health PostDocument367 pagesHSTP II HMIS Hospital Heath Centre and Health PostDagmawitNo ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- UB-04 Claim Form InstructionsDocument10 pagesUB-04 Claim Form InstructionsJonna CaballeroNo ratings yet
- Medical Report and ReceiptDocument5 pagesMedical Report and Receiptkumarsam087No ratings yet
- NTUC Pa Paid Claim Form (08 2017)Document5 pagesNTUC Pa Paid Claim Form (08 2017)pat5355No ratings yet
- ME In-G Ie: Claim FormDocument4 pagesME In-G Ie: Claim FormnithiananthiNo ratings yet
- Cpahb HospitalDocument6 pagesCpahb HospitalHihiNo ratings yet
- Health Premium PlatinumDocument3 pagesHealth Premium Platinumகமலேஷ் குமார்No ratings yet
- ERP Assignment 103Document10 pagesERP Assignment 103Ralph SoansNo ratings yet
- Genins Claim Form (New)Document3 pagesGenins Claim Form (New)pratikwagh112002No ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- Medical Insurance Claim Form (Corporate)Document3 pagesMedical Insurance Claim Form (Corporate)hari198902234No ratings yet
- Claim Form & Other Documents To Be Submitted To Lic Branch/ Divisional Offices OnlyDocument1 pageClaim Form & Other Documents To Be Submitted To Lic Branch/ Divisional Offices OnlyAnonymous W9VINoTza100% (1)
- Medical and Vision Claim Form en 06 - 2018Document2 pagesMedical and Vision Claim Form en 06 - 2018andreas widyoNo ratings yet
- Healt Form LatestDocument9 pagesHealt Form LatestSadab AhmadNo ratings yet
- Certificate of Hospital Treatment - 17062019Document2 pagesCertificate of Hospital Treatment - 17062019Everest HospitalNo ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationHarold TanNo ratings yet
- Linelist Register For HIV POS PBFA and HEIs - Oct 2023Document12 pagesLinelist Register For HIV POS PBFA and HEIs - Oct 2023Migori ArtNo ratings yet
- Form BUPADocument4 pagesForm BUPAterusunduhNo ratings yet
- Bupa Global Claim FormDocument8 pagesBupa Global Claim FormALJABERNo ratings yet
- Bupa International Claim Form: 1 Patient'S DetailsDocument4 pagesBupa International Claim Form: 1 Patient'S DetailsRealty SolutionsNo ratings yet
- Aditya Birla Health Insurance Co. LimitedDocument4 pagesAditya Birla Health Insurance Co. LimitedAdeep MathurNo ratings yet
- 2-GMC Claim Check - ListDocument2 pages2-GMC Claim Check - ListChayan HalderNo ratings yet
- CF05b Path Accident and Sickness Medical ES ADocument3 pagesCF05b Path Accident and Sickness Medical ES ARedención Apostol SantiagoNo ratings yet
- Crisis Cover Kids Claim FormDocument16 pagesCrisis Cover Kids Claim FormHihiNo ratings yet
- Domiciliary Treatment - Claim Form - Borl: Details of Primary InsuredDocument1 pageDomiciliary Treatment - Claim Form - Borl: Details of Primary InsuredHimanshu Chouksey100% (1)
- NEW Domiciliary Claim Form PDFDocument1 pageNEW Domiciliary Claim Form PDFHimanshu ChoukseyNo ratings yet
- MSE Clinical Observer Application April 2021 v2Document6 pagesMSE Clinical Observer Application April 2021 v2M. GNo ratings yet
- Claim - Form - MediassitDocument4 pagesClaim - Form - MediassitKashish BangaloreNo ratings yet
- New MRD PresentationDocument40 pagesNew MRD PresentationBAHHEP BAHHEPNo ratings yet
- 5 6212887793887085843 PDFDocument11 pages5 6212887793887085843 PDFeruditeNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Aakansha GuptaNo ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationFirmament DevelopmentNo ratings yet
- Itemized Sample Billing StatementDocument2 pagesItemized Sample Billing StatementAriel CruzNo ratings yet
- The Oriental Insurance Company Limited: Hospitalisation and Domiciliary Hospitalisation Benefit Policy Claim FormDocument5 pagesThe Oriental Insurance Company Limited: Hospitalisation and Domiciliary Hospitalisation Benefit Policy Claim FormMallesh ArjaNo ratings yet
- House Job Application Form 2020Document3 pagesHouse Job Application Form 2020fatimabakhsh419No ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- Medical OpinionDocument1 pageMedical OpinionefmezahnNo ratings yet
- D StatmentDocument8 pagesD StatmentHihiNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- IRDAI Registration No. 103. Reliance General Insurance Company LimitedDocument2 pagesIRDAI Registration No. 103. Reliance General Insurance Company LimitedSumit BhallaNo ratings yet
- Maid Claim FormDocument4 pagesMaid Claim FormHihiNo ratings yet
- Hospital Benefit Claim FormDocument7 pagesHospital Benefit Claim FormEmmanuel MichaelNo ratings yet
- Claims Reimbursement Form (For MRC) : Member General Information (Required)Document2 pagesClaims Reimbursement Form (For MRC) : Member General Information (Required)lecky youNo ratings yet
- In-Patient Claim Form: (To Be Filled by Claimant Employee)Document2 pagesIn-Patient Claim Form: (To Be Filled by Claimant Employee)Khan LalaNo ratings yet
- Claim Submission Checklist - pdf4454101871738174528Document2 pagesClaim Submission Checklist - pdf4454101871738174528Bireswar SamajpatiNo ratings yet
- 1 Claim FormDocument36 pages1 Claim Formkarmayukh1No ratings yet
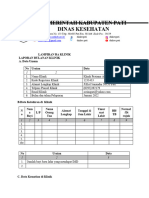
- Laporan Lampiran Ba Kesesuaian KlinikDocument5 pagesLaporan Lampiran Ba Kesesuaian KlinikYENI AYU OKTAVIANo ratings yet
- Insurance Claim FormDocument9 pagesInsurance Claim FormRahmaNo ratings yet
- DME Medical Billing Book 1662598386Document46 pagesDME Medical Billing Book 1662598386Nelson ANo ratings yet
- Clinical Face Sheet: 8 40 - A.M. - P.M. - A.M. - P.MDocument21 pagesClinical Face Sheet: 8 40 - A.M. - P.M. - A.M. - P.MRyrey Abraham PacamanaNo ratings yet
- Hospitalization Reimbursment Claim FormDocument4 pagesHospitalization Reimbursment Claim FormFarhan aliNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (2)
- 2018 Fidelis Care Medicare Advantage Dual Advantage Provider Tip SheetDocument2 pages2018 Fidelis Care Medicare Advantage Dual Advantage Provider Tip Sheetkrishna EnagaluruNo ratings yet
- Welcome To HDFC Bank NetBankingDocument2 pagesWelcome To HDFC Bank NetBankingkrishna EnagaluruNo ratings yet
- Ab 02142Document6 pagesAb 02142krishna EnagaluruNo ratings yet
- 2017 UB04 Hospital Instructions-Final 8FEB2018Document99 pages2017 UB04 Hospital Instructions-Final 8FEB2018krishna EnagaluruNo ratings yet
- Hospital Billing ScenariosDocument7 pagesHospital Billing Scenarioskrishna EnagaluruNo ratings yet
- CMS 2022 C2C RTBC EOB English 8 5X11 V4Document1 pageCMS 2022 C2C RTBC EOB English 8 5X11 V4krishna EnagaluruNo ratings yet
- Module 5 Rle - EvaluationDocument3 pagesModule 5 Rle - EvaluationKyle VargasNo ratings yet
- Principles of Learning and Motivation Part 2Document3 pagesPrinciples of Learning and Motivation Part 2Tobs AnchetaNo ratings yet
- DLL 10 - BioenergeticsDocument3 pagesDLL 10 - BioenergeticsJennifer Magango100% (1)
- Peripheral Testosterone MetabolismDocument8 pagesPeripheral Testosterone MetabolismAgung SentosaNo ratings yet
- Consolidated Teachers Individual Plan For Professional Development SCHOOL YEAR 2020-2021Document2 pagesConsolidated Teachers Individual Plan For Professional Development SCHOOL YEAR 2020-2021Anicadlien Ellipaw IninNo ratings yet
- PDBA Operations Course OutlineDocument12 pagesPDBA Operations Course OutlineQasim AbrahamsNo ratings yet
- Tagbino National High SchoolDocument2 pagesTagbino National High SchooldarelleNo ratings yet
- nnsm322m PDFDocument22 pagesnnsm322m PDFTLTPSNo ratings yet
- Application of IntegralsDocument14 pagesApplication of IntegralsSanjayNo ratings yet
- Writing Research Papers James D Lester PDFDocument4 pagesWriting Research Papers James D Lester PDFgahebak1mez2100% (1)
- 3 Phase Full Wave Bridge ConverterDocument4 pages3 Phase Full Wave Bridge Convertersubhasishpodder100% (1)
- Agrirobot PDFDocument103 pagesAgrirobot PDFMuhamad Azlan ShahNo ratings yet
- Vyshali Java ResumeDocument5 pagesVyshali Java ResumeKiran N9 ITNo ratings yet
- Machine (Mechanical) - Wikipedia, The Free EncyclopediaDocument10 pagesMachine (Mechanical) - Wikipedia, The Free EncyclopediabmxengineeringNo ratings yet
- Safir 9 Tonearm ManualDocument14 pagesSafir 9 Tonearm Manualmoma52No ratings yet
- Research Methodology - 9Document12 pagesResearch Methodology - 9OmeYadavNo ratings yet
- Green Ghost Chronicles - The Lost Book Outline - Tom Furman FitnessDocument49 pagesGreen Ghost Chronicles - The Lost Book Outline - Tom Furman Fitnessbarna284100% (1)
- Configure Anyconnect 00Document22 pagesConfigure Anyconnect 00Ruben VillafaniNo ratings yet
- Bus FestoDocument82 pagesBus FestoraphvalonNo ratings yet
- Encoder Serie Ria-40Document6 pagesEncoder Serie Ria-40Carlos NigmannNo ratings yet
- Harmonization of Strategic PlansDocument47 pagesHarmonization of Strategic PlansLisette Senoc-GarciaNo ratings yet
- Lesson Plan ON OxytocicsDocument18 pagesLesson Plan ON Oxytocicsrenu100% (2)
- Instron Low Velocity Impact TesterDocument179 pagesInstron Low Velocity Impact TesterEmre GuneyNo ratings yet
- SPM (SEN 410) Lecturer HandoutsDocument51 pagesSPM (SEN 410) Lecturer HandoutsinzovarNo ratings yet
- 459 - So FG13Document5 pages459 - So FG13ronni gunadi sNo ratings yet
- Prospective vs. Retrospective Delay Analysis: Rohit Singhal, Shishir Kant & Adarsh KumarDocument10 pagesProspective vs. Retrospective Delay Analysis: Rohit Singhal, Shishir Kant & Adarsh KumarKevin DonNo ratings yet
- CMACGM Service Description ReportDocument58 pagesCMACGM Service Description ReportMarius MoraruNo ratings yet
- Thesis Format Iit KanpurDocument7 pagesThesis Format Iit Kanpurvictoriathompsonaustin100% (2)
- Modal Adverb Lesson PlanDocument4 pagesModal Adverb Lesson Planapi-587326479100% (1)