Download as pdf or txt
You might also like
- Liver CirrhosisDocument31 pagesLiver CirrhosisMarisol Jane Jomaya50% (2)
- 1 - Chapter 1. Introduction To Healthcare FinanceDocument1 page1 - Chapter 1. Introduction To Healthcare Financenadia nuraniNo ratings yet
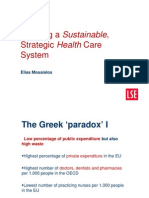
- Creating A Sustainable, Strategic Health Care System: Elias MossialosDocument20 pagesCreating A Sustainable, Strategic Health Care System: Elias MossialosΤσεκουράτος ΕθνικοφιλελεύθεροςNo ratings yet
- UK V's US HealthcareDocument16 pagesUK V's US HealthcareAnthony WoodheadNo ratings yet
- Comparing Health System Performance in OECD CountriesDocument14 pagesComparing Health System Performance in OECD CountriesromanpollyNo ratings yet
- Healthcare System and Problems of Medical Personnel in GeorgiaDocument6 pagesHealthcare System and Problems of Medical Personnel in Georgianino burdiashviliNo ratings yet
- 500 Research Proposal Templete (Suggested)Document9 pages500 Research Proposal Templete (Suggested)sara gadNo ratings yet
- Economics 2015 4Document57 pagesEconomics 2015 4Azmi Rizki LubisNo ratings yet
- 1 s2.0 S2212828X18300598 MainDocument19 pages1 s2.0 S2212828X18300598 Mainmandeep kaurNo ratings yet
- Council of The European Union Brussels, 10 March 2003Document36 pagesCouncil of The European Union Brussels, 10 March 2003Antonia Milena LambaNo ratings yet
- Lec1 Introduction STDocument37 pagesLec1 Introduction STMiracleTesfayeNo ratings yet
- Health Insurance SystemDocument39 pagesHealth Insurance SystemᎷᏒ.ᏴᎬᎪᏚᎢ.No ratings yet
- WHO HIS HSR 17.15 Eng PDFDocument12 pagesWHO HIS HSR 17.15 Eng PDFNebyuNo ratings yet
- Anderson and Frogner Health Spending HA '08Document10 pagesAnderson and Frogner Health Spending HA '08Michelle WebbNo ratings yet
- Health Effects of Financial Crisis Omens of A Greek Tragedy-The Lancet, Early Online Publication, 10 October 2011Document5 pagesHealth Effects of Financial Crisis Omens of A Greek Tragedy-The Lancet, Early Online Publication, 10 October 2011jimdioNo ratings yet
- GG2071 Health DevelopmentDocument38 pagesGG2071 Health DevelopmentamyhryhorukNo ratings yet
- Taking The PulseDocument12 pagesTaking The PulseLuke DezarNo ratings yet
- 2019 CHP FR EnglishDocument24 pages2019 CHP FR EnglishCarmine de LuciaNo ratings yet
- E, E, M F: T D I M C R: Quality Fficiency AND Arket UndamentalsDocument45 pagesE, E, M F: T D I M C R: Quality Fficiency AND Arket UndamentalsafsNo ratings yet
- Public Health Security and Forecasting Economic Trends: Selected Papers of Beijing Forum2006Document8 pagesPublic Health Security and Forecasting Economic Trends: Selected Papers of Beijing Forum2006Dita MarthaNo ratings yet
- NR 17 - Lesões Musculoesqueléticas No Setor Da SaúdeDocument23 pagesNR 17 - Lesões Musculoesqueléticas No Setor Da SaúdeCPSSTNo ratings yet
- Review ArticleDocument9 pagesReview Article123065No ratings yet
- 2.CiberneticaTHE USE OF QUANTITATIVE TECHNIQUES IN THE ANALYSIS OF GEOGRAPHICAL FEATURES REGARDING PATIENTS WITH ACUTE CORONARY SYNDROMESDocument18 pages2.CiberneticaTHE USE OF QUANTITATIVE TECHNIQUES IN THE ANALYSIS OF GEOGRAPHICAL FEATURES REGARDING PATIENTS WITH ACUTE CORONARY SYNDROMESbogdan.oancea3651No ratings yet
- Health2020: A New WHO Strategy To Promote Well-Being and Tackle Chronic Diseases in EuropeDocument16 pagesHealth2020: A New WHO Strategy To Promote Well-Being and Tackle Chronic Diseases in EuropeFit for Work EuropeNo ratings yet
- Luxembourg LU: State of Health in The EUDocument24 pagesLuxembourg LU: State of Health in The EUSilvia BotarcaNo ratings yet
- HI08 Comparing Payor PerformaceDocument10 pagesHI08 Comparing Payor PerformaceCenterbackNo ratings yet
- Expanding Accessto Cancer Care and Control in LMICs: Lessons For Health Systems 051211Document36 pagesExpanding Accessto Cancer Care and Control in LMICs: Lessons For Health Systems 051211Presentaciones_FKNo ratings yet
- Population Aging and Economic Growth: P G D ADocument38 pagesPopulation Aging and Economic Growth: P G D AHukam ChandNo ratings yet
- Country Health Profile 2019 Sweden PDFDocument24 pagesCountry Health Profile 2019 Sweden PDFIlu MatsonNo ratings yet
- 2018 Healthatglance Sum enDocument4 pages2018 Healthatglance Sum enLucian SalaNo ratings yet
- BMJ Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To BMJ: British Medical JournalDocument4 pagesBMJ Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To BMJ: British Medical Journalashakow8849No ratings yet
- Ijphcs: A Comparison of Hiv/Aids Health Policy in Selected Developed and Developing CountriesDocument14 pagesIjphcs: A Comparison of Hiv/Aids Health Policy in Selected Developed and Developing Countriesadelin ransunNo ratings yet
- 1 The Industrial Organization of Health Care Markets PDFDocument63 pages1 The Industrial Organization of Health Care Markets PDFRafael Ruiz-MonroyNo ratings yet
- Michael Gregg - Field Epidemiology Tahap Awal InvestigasiDocument61 pagesMichael Gregg - Field Epidemiology Tahap Awal InvestigasiMegan TariNo ratings yet
- The Persistance Of....Document36 pagesThe Persistance Of....agapito di sousaNo ratings yet
- Does Rising Income Inequality Affect Mortality Rates in Advanced Economies?Document24 pagesDoes Rising Income Inequality Affect Mortality Rates in Advanced Economies?Puspitha PuspithaNo ratings yet
- Hospital Capacity in Germany PreDocument12 pagesHospital Capacity in Germany PreRASMITA BHANDARINo ratings yet
- World Health Report 2008Document5 pagesWorld Health Report 2008suryo bantoloNo ratings yet
- Maternal Mortality RateDocument17 pagesMaternal Mortality Rateapi-19731757No ratings yet
- Recessions and HealthDocument23 pagesRecessions and HealthTyson SmithNo ratings yet
- 2004-07-17 The Health of Nations - The Economist - Tome 1Document8 pages2004-07-17 The Health of Nations - The Economist - Tome 1Guillaume ZhangNo ratings yet
- Obesity, Inflammation, and Periodontal Disease: Critical Reviews in Oral Biology & MedicineDocument11 pagesObesity, Inflammation, and Periodontal Disease: Critical Reviews in Oral Biology & MedicineClaudia Patricia Ballen GarzonNo ratings yet
- Romania: Health Sector Policy Note I. Background and AccomplishmentsDocument11 pagesRomania: Health Sector Policy Note I. Background and AccomplishmentsMaria Gabriela PopaNo ratings yet
- Ep101.1-4 Fa - 2010.11 - V1.0Document5 pagesEp101.1-4 Fa - 2010.11 - V1.0AngellaNo ratings yet
- Cristian Vlădescu Vasile Astărăstoae Silvia Gabriela ScînteeDocument10 pagesCristian Vlădescu Vasile Astărăstoae Silvia Gabriela ScînteeaditeocanNo ratings yet
- Health Econ BibDocument262 pagesHealth Econ BibAhmed HassanNo ratings yet
- 758 ResearchpaperfinalDocument20 pages758 Researchpaperfinalapi-209297122No ratings yet
- A Successful and Sustainable Health System - How To Get There From HereDocument8 pagesA Successful and Sustainable Health System - How To Get There From HereSherlocknovNo ratings yet
- The World Bank - NCDs in JamaicaDocument78 pagesThe World Bank - NCDs in JamaicaeyecarecaribbeanNo ratings yet
- Country Health Profile 2019 CroatiaDocument24 pagesCountry Health Profile 2019 CroatiaMichele BigarelliNo ratings yet
- Job Satisfaction of Physicians in RussiaDocument11 pagesJob Satisfaction of Physicians in RussiaAnnisa OktantianiNo ratings yet
- Human DevelopmentDocument6 pagesHuman DevelopmentjohnmorriscryptoNo ratings yet
- Causes of Death Analysis 1990-2013 by HSEDocument55 pagesCauses of Death Analysis 1990-2013 by HSEРуслан ЗайдуллинNo ratings yet
- Cochran-Mantel-Haenszel Test: Figure 1. Age-Adjusted Incidence of Melanoma by Race and Gender SEER Data, 1973-1998Document5 pagesCochran-Mantel-Haenszel Test: Figure 1. Age-Adjusted Incidence of Melanoma by Race and Gender SEER Data, 1973-1998apb91781No ratings yet
- Healthcare As Social InfrastructureDocument29 pagesHealthcare As Social InfrastructureJohn Andrei BoninaNo ratings yet
- Leading Causes of MortalityDocument12 pagesLeading Causes of MortalityJayricDepalobosNo ratings yet
- Primary Health Care Systems (Primasys) : Case Study From EthiopiaDocument12 pagesPrimary Health Care Systems (Primasys) : Case Study From EthiopiaMuluken TesfayeNo ratings yet
- Health Disparities and Health Education-1finalDocument12 pagesHealth Disparities and Health Education-1finalbrendahronoh254No ratings yet
- Economic Modelling: Laurent Augier, Amy YalyDocument11 pagesEconomic Modelling: Laurent Augier, Amy YalyserhanNo ratings yet
- Primary Health Care Systems (Primasys) : Case Study From MexicoDocument16 pagesPrimary Health Care Systems (Primasys) : Case Study From MexicoEpi SidaNo ratings yet
- Key Health System Indicators: Djibouti: Health Systems ProfileDocument2 pagesKey Health System Indicators: Djibouti: Health Systems ProfilemNo ratings yet
- Telemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.From EverandTelemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.No ratings yet
- Universal Declaration of Human RightsDocument8 pagesUniversal Declaration of Human RightselectedwessNo ratings yet
- Aw-Kars2020-1-Desain Kualitatif-Mei 152020Document89 pagesAw-Kars2020-1-Desain Kualitatif-Mei 152020nadia nuraniNo ratings yet
- Residensi Kajian Swot RS Karsui Jusuf 2020Document40 pagesResidensi Kajian Swot RS Karsui Jusuf 2020nadia nuraniNo ratings yet
- Health System Resilience in Managing Pandemic Covid-19Document8 pagesHealth System Resilience in Managing Pandemic Covid-19nadia nuraniNo ratings yet
- Pembelajaran EpidDocument23 pagesPembelajaran Epidnadia nuraniNo ratings yet
- TK RS 2018 Cambridge Memorial Hospital By-Laws (Canada)Document33 pagesTK RS 2018 Cambridge Memorial Hospital By-Laws (Canada)nadia nuraniNo ratings yet
- Structure Literature Review Business ProcessDocument28 pagesStructure Literature Review Business Processnadia nuraniNo ratings yet
- Hospital Marketing Hospital Marketing: Wahyu SulistiadiDocument32 pagesHospital Marketing Hospital Marketing: Wahyu Sulistiadinadia nuraniNo ratings yet
- Hospital Marketing: Concept & ImplementationsDocument46 pagesHospital Marketing: Concept & Implementationsnadia nuraniNo ratings yet
- 4.analisis Situasi, FKK-SWOTDocument93 pages4.analisis Situasi, FKK-SWOTnadia nuraniNo ratings yet
- Health Policy Brief: Telehealth Parity LawsDocument5 pagesHealth Policy Brief: Telehealth Parity Lawsnadia nuraniNo ratings yet
- Toshiba Xario XG Yanamed PDFDocument6 pagesToshiba Xario XG Yanamed PDFHassan bin QasimNo ratings yet
- Integrating Health and Wellness in Mental Health Counseling: Clinical, Educational, and Policy ImplicationsDocument13 pagesIntegrating Health and Wellness in Mental Health Counseling: Clinical, Educational, and Policy ImplicationsGabriela Sanchez100% (1)
- Weekly Agenda 12 Reading Exam PracticeDocument13 pagesWeekly Agenda 12 Reading Exam PracticeValerie Cordoba TeranNo ratings yet
- Thoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Document4 pagesThoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Mincheol KangNo ratings yet
- Abdominal Compartment Syndrome and Intra Abdominal.21 PDFDocument9 pagesAbdominal Compartment Syndrome and Intra Abdominal.21 PDFFIA SlotNo ratings yet
- SCOLIOSISDocument4 pagesSCOLIOSISapi-3822433No ratings yet
- Acute Nephrotic SyndromeDocument1 pageAcute Nephrotic SyndromeXarius FidelNo ratings yet
- Norway Rats: Damage Prevention and Control MethodsDocument16 pagesNorway Rats: Damage Prevention and Control MethodswiamNo ratings yet
- Drug Study (Burn Injury) ManuscriptDocument4 pagesDrug Study (Burn Injury) ManuscriptEricka VillanuevaNo ratings yet
- Year 9 Yealy Exam 2022Document25 pagesYear 9 Yealy Exam 2022fraNo ratings yet
- Surgery 4 - Answers v1 (Wide)Document55 pagesSurgery 4 - Answers v1 (Wide)Humzala BashamNo ratings yet
- PHILOSOPHY and DISABILITYDocument21 pagesPHILOSOPHY and DISABILITYLuhan Albert YnarezNo ratings yet
- Case StudyDocument7 pagesCase StudyLimit.マイクNo ratings yet
- Catalog PrismxelDocument2 pagesCatalog PrismxelValentin DNo ratings yet
- NIH Public Access: Author ManuscriptDocument24 pagesNIH Public Access: Author ManuscriptAnonymous hTivgzixVNNo ratings yet
- Clinical Science Questions and AnswersDocument30 pagesClinical Science Questions and Answersrakeeb qadriNo ratings yet
- (BIO) Chapter 4 - Nutrition in HumanDocument21 pages(BIO) Chapter 4 - Nutrition in Humantaco ghoulNo ratings yet
- The Chemistry of Natural Product Plant Secondary MetabolitesDocument9 pagesThe Chemistry of Natural Product Plant Secondary MetabolitesImdad HussainNo ratings yet
- Cureus 0015 00000046390Document8 pagesCureus 0015 00000046390vita udiNo ratings yet
- Volume 46, Issue 7, February 12, 2016Document64 pagesVolume 46, Issue 7, February 12, 2016BladeNo ratings yet
- Jufe 4 10.30Document17 pagesJufe 4 10.30LíaNo ratings yet
- Classification of PulpitisDocument18 pagesClassification of PulpitisEkrar Okto ViarNo ratings yet
- 6.1-EnT EnteroPluri TubeDocument12 pages6.1-EnT EnteroPluri TubeRAO NABEEL AKRAMNo ratings yet
- Faith Independent, January 23, 2013Document16 pagesFaith Independent, January 23, 2013surfnewmediaNo ratings yet
- 29 Recommended and Released Varieties 2011Document44 pages29 Recommended and Released Varieties 2011Fay Bacalso GascoNo ratings yet
- Clinical Understanding of The Sign "Blue Sclera" in Some CasesDocument4 pagesClinical Understanding of The Sign "Blue Sclera" in Some CasesDr. Bikash BiswasNo ratings yet
- Antibiotic PolicyDocument35 pagesAntibiotic PolicyArpita Garg100% (2)
- Mod14 TerminologyDocument6 pagesMod14 Terminologypilsen_01No ratings yet
- 2020 Can Pelvic Floor Muscle TrainingDocument2 pages2020 Can Pelvic Floor Muscle Trainingjuan pabloNo ratings yet