
Starvation Ketosis and The Kidney: In-Depth Topic Review
Starvation Ketosis and The Kidney: In-Depth Topic Review
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- General Organic and Biochemistry 10Th Edition Katherine Denniston Full ChapterDocument67 pagesGeneral Organic and Biochemistry 10Th Edition Katherine Denniston Full Chapterrichard.hafer244100% (11)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Maida Testing ProcedureDocument6 pagesMaida Testing ProcedureRahul Suryavanshi100% (1)
- DURIT Thermal-CoatingsDocument8 pagesDURIT Thermal-CoatingsMatheusNo ratings yet
- Aw0331f MSDSDocument2 pagesAw0331f MSDSson.nh98bgNo ratings yet
- Fick'S Law of DiffusionDocument10 pagesFick'S Law of DiffusiondhruvNo ratings yet
- Platinum-Group Elements PDFDocument6 pagesPlatinum-Group Elements PDFcristianNo ratings yet
- CHANGES IN PH OF MILK DURING FREEZING AND FROZEN STORAGEDocument6 pagesCHANGES IN PH OF MILK DURING FREEZING AND FROZEN STORAGEching chongNo ratings yet
- 17ME64 DME II Module 5Document13 pages17ME64 DME II Module 5Shridhar ChinuuNo ratings yet
- PC Cell 64004Document1 pagePC Cell 64004SutarnoNo ratings yet
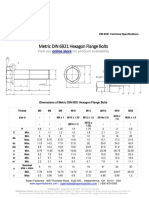
- Metric DIN 6921 Hexagon Flange Bolts: Visit Our For Product AvailabilityDocument5 pagesMetric DIN 6921 Hexagon Flange Bolts: Visit Our For Product AvailabilityJaganNo ratings yet
- Ert 312 - Lecture 5Document43 pagesErt 312 - Lecture 5mabmi17No ratings yet
- 1129eatx Carbocrylic 1290 - Atex - A Euclpsds EnglishDocument11 pages1129eatx Carbocrylic 1290 - Atex - A Euclpsds EnglishclintonNo ratings yet
- 8 Sterility Testing of PharmaceuticalsDocument14 pages8 Sterility Testing of PharmaceuticalsGaurav MudaduNo ratings yet
- Fire ExtinguisherDocument51 pagesFire ExtinguisherStephen AnoffNo ratings yet
- Ammonium Hydroxide, 1.0N (1.0M) : Safety Data SheetDocument7 pagesAmmonium Hydroxide, 1.0N (1.0M) : Safety Data Sheetminyoon sugarNo ratings yet
- Vinegar Planning and Design LabDocument3 pagesVinegar Planning and Design LabKim ThaiNo ratings yet
- 10MM - 60.960 TonDocument4 pages10MM - 60.960 TonRAJKUMAR CHATTERJEE. (RAJA.)100% (1)
- B679-98 (2009) Standard Specification For Electrodeposited Coatings of Palladium For Engineering Use PDFDocument6 pagesB679-98 (2009) Standard Specification For Electrodeposited Coatings of Palladium For Engineering Use PDFdiego rodriguezNo ratings yet
- Viia GroupDocument30 pagesViia GroupTarun SharmaNo ratings yet
- VizagSteel MgmtTRAINEEDocument28 pagesVizagSteel MgmtTRAINEERaghu88% (16)
- General Chem 1 Summative Test CherryDocument5 pagesGeneral Chem 1 Summative Test CherryJoshua RaguinganNo ratings yet
- Gaswelcome: AV.S Ram PrasadDocument50 pagesGaswelcome: AV.S Ram PrasadAkhil MetlaNo ratings yet
- Research Report 296Document53 pagesResearch Report 296marcela walterosNo ratings yet
- Fatigue: TorsionalDocument9 pagesFatigue: TorsionalShankar RamanNo ratings yet
- Polytechnics JAMB BrochureDocument62 pagesPolytechnics JAMB BrochureÃdë Kùñ LëNo ratings yet
- Chrome Plated On SSDocument5 pagesChrome Plated On SSamh.fpdNo ratings yet
- Research Paper in PHYSICSDocument8 pagesResearch Paper in PHYSICSAngelica Rico100% (1)
- Sound Velocity Chart PDFDocument1 pageSound Velocity Chart PDFJamesNo ratings yet
- Chapter 3 EvapotranspirationDocument20 pagesChapter 3 EvapotranspirationnimcanNo ratings yet
- Generon Membrane 4100 CPDocument2 pagesGeneron Membrane 4100 CPJavier Garcia MarquezNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- General Organic and Biochemistry 10Th Edition Katherine Denniston Full ChapterDocument67 pagesGeneral Organic and Biochemistry 10Th Edition Katherine Denniston Full Chapterrichard.hafer244100% (11)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Maida Testing ProcedureDocument6 pagesMaida Testing ProcedureRahul Suryavanshi100% (1)
- DURIT Thermal-CoatingsDocument8 pagesDURIT Thermal-CoatingsMatheusNo ratings yet
- Aw0331f MSDSDocument2 pagesAw0331f MSDSson.nh98bgNo ratings yet
- Fick'S Law of DiffusionDocument10 pagesFick'S Law of DiffusiondhruvNo ratings yet
- Platinum-Group Elements PDFDocument6 pagesPlatinum-Group Elements PDFcristianNo ratings yet
- CHANGES IN PH OF MILK DURING FREEZING AND FROZEN STORAGEDocument6 pagesCHANGES IN PH OF MILK DURING FREEZING AND FROZEN STORAGEching chongNo ratings yet
- 17ME64 DME II Module 5Document13 pages17ME64 DME II Module 5Shridhar ChinuuNo ratings yet
- PC Cell 64004Document1 pagePC Cell 64004SutarnoNo ratings yet
- Metric DIN 6921 Hexagon Flange Bolts: Visit Our For Product AvailabilityDocument5 pagesMetric DIN 6921 Hexagon Flange Bolts: Visit Our For Product AvailabilityJaganNo ratings yet
- Ert 312 - Lecture 5Document43 pagesErt 312 - Lecture 5mabmi17No ratings yet
- 1129eatx Carbocrylic 1290 - Atex - A Euclpsds EnglishDocument11 pages1129eatx Carbocrylic 1290 - Atex - A Euclpsds EnglishclintonNo ratings yet
- 8 Sterility Testing of PharmaceuticalsDocument14 pages8 Sterility Testing of PharmaceuticalsGaurav MudaduNo ratings yet
- Fire ExtinguisherDocument51 pagesFire ExtinguisherStephen AnoffNo ratings yet
- Ammonium Hydroxide, 1.0N (1.0M) : Safety Data SheetDocument7 pagesAmmonium Hydroxide, 1.0N (1.0M) : Safety Data Sheetminyoon sugarNo ratings yet
- Vinegar Planning and Design LabDocument3 pagesVinegar Planning and Design LabKim ThaiNo ratings yet
- 10MM - 60.960 TonDocument4 pages10MM - 60.960 TonRAJKUMAR CHATTERJEE. (RAJA.)100% (1)
- B679-98 (2009) Standard Specification For Electrodeposited Coatings of Palladium For Engineering Use PDFDocument6 pagesB679-98 (2009) Standard Specification For Electrodeposited Coatings of Palladium For Engineering Use PDFdiego rodriguezNo ratings yet
- Viia GroupDocument30 pagesViia GroupTarun SharmaNo ratings yet
- VizagSteel MgmtTRAINEEDocument28 pagesVizagSteel MgmtTRAINEERaghu88% (16)
- General Chem 1 Summative Test CherryDocument5 pagesGeneral Chem 1 Summative Test CherryJoshua RaguinganNo ratings yet
- Gaswelcome: AV.S Ram PrasadDocument50 pagesGaswelcome: AV.S Ram PrasadAkhil MetlaNo ratings yet
- Research Report 296Document53 pagesResearch Report 296marcela walterosNo ratings yet
- Fatigue: TorsionalDocument9 pagesFatigue: TorsionalShankar RamanNo ratings yet
- Polytechnics JAMB BrochureDocument62 pagesPolytechnics JAMB BrochureÃdë Kùñ LëNo ratings yet
- Chrome Plated On SSDocument5 pagesChrome Plated On SSamh.fpdNo ratings yet
- Research Paper in PHYSICSDocument8 pagesResearch Paper in PHYSICSAngelica Rico100% (1)
- Sound Velocity Chart PDFDocument1 pageSound Velocity Chart PDFJamesNo ratings yet
- Chapter 3 EvapotranspirationDocument20 pagesChapter 3 EvapotranspirationnimcanNo ratings yet
- Generon Membrane 4100 CPDocument2 pagesGeneron Membrane 4100 CPJavier Garcia MarquezNo ratings yet