Download as pdf or txt
You might also like
- Communication of Cancer-Related Genetic and Genomic Infor-Mation: A Landscape Analysis of ReviewsDocument12 pagesCommunication of Cancer-Related Genetic and Genomic Infor-Mation: A Landscape Analysis of ReviewsRatih puspita DewiNo ratings yet
- 1 s2.0 S030438352100447X MainDocument14 pages1 s2.0 S030438352100447X MainRick ZHUNo ratings yet
- 9424-Article Text-69428-1-10-20200725Document10 pages9424-Article Text-69428-1-10-20200725KELLY ALEJANDRA CAICEDO DIAZNo ratings yet
- The Role of Ablative Radiotherapy in Older Adults With Limited Metastatic DiseaseDocument7 pagesThe Role of Ablative Radiotherapy in Older Adults With Limited Metastatic DiseaseRaul Matute MartinNo ratings yet
- Older Adults With Cancer and Their Caregivers - Current Landscape and Future Directions For Clinical CareDocument14 pagesOlder Adults With Cancer and Their Caregivers - Current Landscape and Future Directions For Clinical CareSybil LandrinNo ratings yet
- Ni Hms 957840Document19 pagesNi Hms 957840dokterlisaNo ratings yet
- Nihms 1660337Document32 pagesNihms 1660337Gretell HenriquezNo ratings yet
- Therapeutic Advances in Alcohol Associated HepatitDocument12 pagesTherapeutic Advances in Alcohol Associated HepatitCláudia SilvaNo ratings yet
- Prognostic Factors For Long-Term Survival After GlioblastomaDocument4 pagesPrognostic Factors For Long-Term Survival After GlioblastomaALINo ratings yet
- MM GuidelineDocument40 pagesMM GuidelineANDREANo ratings yet
- ST Gallen 2021 A OncologyDocument20 pagesST Gallen 2021 A OncologyJorge Apolo PinzaNo ratings yet
- Feasibility and Outcome of Haploidentical Hematopoietic Stem Cell Transplant With Post Transplantation Cyclophosphamide in High Risk Malignancies in ChildrenDocument4 pagesFeasibility and Outcome of Haploidentical Hematopoietic Stem Cell Transplant With Post Transplantation Cyclophosphamide in High Risk Malignancies in ChildrenHerald Scholarly Open AccessNo ratings yet
- Hepatocellular Carcinoma: Clinical Frontiers and PerspectivesDocument13 pagesHepatocellular Carcinoma: Clinical Frontiers and PerspectivesMisnariahIdrusNo ratings yet
- Edbk 159244Document11 pagesEdbk 159244ayuNo ratings yet
- ProfilaksisDocument4 pagesProfilaksisLatifah MaharaniNo ratings yet
- Nihms 1745031Document38 pagesNihms 1745031Rapho1253No ratings yet
- Machine Learning Approaches To Drug Response Prediction: Challenges and Recent ProgressDocument10 pagesMachine Learning Approaches To Drug Response Prediction: Challenges and Recent ProgressKunel KumarNo ratings yet
- Editorial Transl Medicine ReportsDocument4 pagesEditorial Transl Medicine Reportsapi-334757816No ratings yet
- Metastasis Patterns and PrognoDocument17 pagesMetastasis Patterns and Prognosatria divaNo ratings yet
- The Prevalence and Outcomes of Frail Older Adults in Clinical Trials in Multiple Myeloma: A Systematic ReviewDocument13 pagesThe Prevalence and Outcomes of Frail Older Adults in Clinical Trials in Multiple Myeloma: A Systematic Reviewfga.crislainebernardino01No ratings yet
- Treatment of The Elderly When Cure Is The GoalDocument8 pagesTreatment of The Elderly When Cure Is The GoalCatia AraujoNo ratings yet
- Tauber Et Al. (2019) - Effect of Psychological - RecurrenceDocument18 pagesTauber Et Al. (2019) - Effect of Psychological - RecurrenceViridiana Eguía MartínezNo ratings yet
- Palliative Chemotherapy For Advanced Colorectal Cancer Systemati 2000Document5 pagesPalliative Chemotherapy For Advanced Colorectal Cancer Systemati 2000Wiro SablengNo ratings yet
- Sickle Cell Literature ReviewDocument8 pagesSickle Cell Literature Reviewafdtnybjp100% (1)
- Outcome of Allogeneic Hematopoietic Stem Cell Transplantati - 2019 - Biology ofDocument9 pagesOutcome of Allogeneic Hematopoietic Stem Cell Transplantati - 2019 - Biology ofFrankenstein MelancholyNo ratings yet
- 2021 Cancer VaccineDocument9 pages2021 Cancer VaccineDenisse IuliaNo ratings yet
- (JURNAL, Eng) Prescribing Potentially Inappropriate Medications For The Elderly According To Beers Criteria, Systematic ReviewDocument12 pages(JURNAL, Eng) Prescribing Potentially Inappropriate Medications For The Elderly According To Beers Criteria, Systematic ReviewAurellia Annisa WulandariNo ratings yet
- Comparison of Total Body Irradiation Versus Non-Total Body Irradiation Containing Regimens For de Novo Acute Myeloid Leukemia in ChildrenDocument7 pagesComparison of Total Body Irradiation Versus Non-Total Body Irradiation Containing Regimens For de Novo Acute Myeloid Leukemia in ChildrenAbdurrahman HasanuddinNo ratings yet
- hsr2 214Document7 pageshsr2 214mehakNo ratings yet
- 2020, JCO - disseminationandImplementationofPalliative CareinOncologyDocument8 pages2020, JCO - disseminationandImplementationofPalliative CareinOncologycharmyshkuNo ratings yet
- Hurria ToxicidadDocument9 pagesHurria ToxicidadKathyMarambioNo ratings yet
- Precision Oncology Colorectal CancerDocument23 pagesPrecision Oncology Colorectal CancerNasheen NaidooNo ratings yet
- Implications of Cancer Prior To and After Heart TransplantationDocument8 pagesImplications of Cancer Prior To and After Heart TransplantationRaúl MartínezNo ratings yet
- Endometrial Cancer Molecular Classification and FuDocument13 pagesEndometrial Cancer Molecular Classification and Fuafzaahmad212No ratings yet
- Dawczak Debicka 2022 Complementary and Alternative TheraDocument15 pagesDawczak Debicka 2022 Complementary and Alternative Therabisak.j.adelaNo ratings yet
- Clinical Practice Guidelines and Quality of Care For Older Patients With Multiple Comorbid DiseasesDocument9 pagesClinical Practice Guidelines and Quality of Care For Older Patients With Multiple Comorbid DiseasesBiblioteca Centro Médico De Mar del PlataNo ratings yet
- Leblanc 2018Document8 pagesLeblanc 2018Eunice BarrosNo ratings yet
- Biology of Blood and Marrow Transplantation: Sudipto Mukherjee, Dominic Boccaccio, Mikkael A. Sekeres, Edward CopelanDocument9 pagesBiology of Blood and Marrow Transplantation: Sudipto Mukherjee, Dominic Boccaccio, Mikkael A. Sekeres, Edward CopelanFran QuagliarielloNo ratings yet
- Fmolb 11 1394585Document18 pagesFmolb 11 1394585Rodrigo SierraNo ratings yet
- Mathematical and Statistical Modeling in Cancer Systems BiologyDocument8 pagesMathematical and Statistical Modeling in Cancer Systems Biologyblumarin99No ratings yet
- Modeling and Analyzing Predictive Monthly Survival in Females Diagnosed With Gynecological CancersDocument10 pagesModeling and Analyzing Predictive Monthly Survival in Females Diagnosed With Gynecological CancersIJPHSNo ratings yet
- Roylance 1997Document8 pagesRoylance 1997barti koksNo ratings yet
- Health-Promoting Behaviors Among Patients With Coronary Artery Disease in PalestineDocument10 pagesHealth-Promoting Behaviors Among Patients With Coronary Artery Disease in Palestineاحمد العايديNo ratings yet
- Decision Making in Differences of Sex DevelopmentDocument3 pagesDecision Making in Differences of Sex DevelopmentHamad ShahNo ratings yet
- How I Treat Acute Myeloid LeukemiaDocument10 pagesHow I Treat Acute Myeloid LeukemiaSutiara Prihatining TyasNo ratings yet
- HHS Public Access: Active Surveillance For Low-Risk Cancers - A Viable Solution To Overtreatment?Document5 pagesHHS Public Access: Active Surveillance For Low-Risk Cancers - A Viable Solution To Overtreatment?Pedro Gómez RNo ratings yet
- Biomarkers For The Diagnosis of Cholangiocarcinoma A Systematic Review 2018Document10 pagesBiomarkers For The Diagnosis of Cholangiocarcinoma A Systematic Review 2018Anna MariaNo ratings yet
- Jurnal Ipd 10Document8 pagesJurnal Ipd 10indra mendilaNo ratings yet
- HHS Public AccessDocument17 pagesHHS Public Accessm_manuela2002No ratings yet
- 10 1200@jco 18 02112Document10 pages10 1200@jco 18 02112jessicamraguiarNo ratings yet
- Nihms 1506873Document26 pagesNihms 1506873Ariana HurtadoNo ratings yet
- Healthcare SpendingDocument20 pagesHealthcare Spendingmikeb92556No ratings yet
- Advanced Basal Cell Carcinoma: Epidemiology and Therapeutic InnovationsDocument6 pagesAdvanced Basal Cell Carcinoma: Epidemiology and Therapeutic InnovationstonyStarkNo ratings yet
- Logistical and Structural Challenges Are The Major Obstacles For Family Medicine Physicians' Ability To Administer Adult VaccinesDocument7 pagesLogistical and Structural Challenges Are The Major Obstacles For Family Medicine Physicians' Ability To Administer Adult Vaccinescarla laureanoNo ratings yet
- Bluethmann2016 PDFDocument9 pagesBluethmann2016 PDFramangNo ratings yet
- 2023 10 1 451 PDFDocument16 pages2023 10 1 451 PDFBeatriz Melo de Almeida100% (1)
- CMW 051Document4 pagesCMW 051Laila Kurnia PramonoNo ratings yet
- 1 s2.0 S0305737217300531 MainDocument11 pages1 s2.0 S0305737217300531 MaindadupipaNo ratings yet
- How I Treat Newly Diagnosed Chronic Phase CMLDocument9 pagesHow I Treat Newly Diagnosed Chronic Phase CMLDenisse SarabiaNo ratings yet
- Precision Medicine Oncology: A PrimerFrom EverandPrecision Medicine Oncology: A PrimerLorna Rodriguez-RodriguezNo ratings yet
- 1 s2.0 S1083879120307060 MainDocument7 pages1 s2.0 S1083879120307060 MainCommon JaiswalNo ratings yet
- 1 s2.0 S1083879120305863 MainDocument4 pages1 s2.0 S1083879120305863 MainCommon JaiswalNo ratings yet
- 1 s2.0 S1083879120305735 MainDocument3 pages1 s2.0 S1083879120305735 MainCommon JaiswalNo ratings yet
- Iit M Dad Diploma An3 Exam QPD3Document229 pagesIit M Dad Diploma An3 Exam QPD3Common JaiswalNo ratings yet
- Category Specifics Comments: Bethesda Classification of Cervical CytologyDocument2 pagesCategory Specifics Comments: Bethesda Classification of Cervical Cytologysaad awanNo ratings yet
- Erdosteine Ref NOV07Document1 pageErdosteine Ref NOV07dofqueriaNo ratings yet
- Kinds of Practice: Bayaborda, Bulaun, Caab, CabilosDocument62 pagesKinds of Practice: Bayaborda, Bulaun, Caab, Cabilosbayaborda.madeleinegraceNo ratings yet
- Par QDocument2 pagesPar Qaicel sagaNo ratings yet
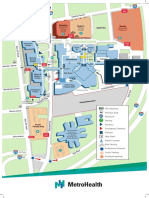
- Main Campus Map Version March 2021Document2 pagesMain Campus Map Version March 2021cjarcher1677No ratings yet
- Ilovepdf MergedDocument125 pagesIlovepdf MergedinnyNo ratings yet
- Alexis GDocument2 pagesAlexis Gapi-518586529No ratings yet
- 4th Generation HIV TestingDocument31 pages4th Generation HIV TestingSC SCNo ratings yet
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Document8 pagesDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Anonymous iJc2y0No ratings yet
- Sausage FinalDocument15 pagesSausage FinalJohn Michael Valencia SabioNo ratings yet
- Objectives:: General ObjectiveDocument6 pagesObjectives:: General ObjectiveGio Carlo QuiambaoNo ratings yet
- Gynae BOOK NEWDocument23 pagesGynae BOOK NEWMuhtasim HaqueNo ratings yet
- 30320Document392 pages303209dsNo ratings yet
- Dr. Clemente InterviewDocument2 pagesDr. Clemente InterviewCandice Trixia Tiu TanNo ratings yet
- Jurnal Gizi Klinik Indonesia: Fast Food and Soft Drink Consumption As Obesity Risk Factor AdolescentsDocument15 pagesJurnal Gizi Klinik Indonesia: Fast Food and Soft Drink Consumption As Obesity Risk Factor AdolescentsResti PerdanaNo ratings yet
- The Accuracy of Different Dental Impression Techniques For Implant-Supported Dental Prostheses: A Systematic Review and Meta - AnalysisDocument19 pagesThe Accuracy of Different Dental Impression Techniques For Implant-Supported Dental Prostheses: A Systematic Review and Meta - AnalysisAnonymous AyxIccS4aXNo ratings yet
- Mcu-Fdt Medical Foundation Hospital Out Patient Services: Chief Complaint: History of Present IllnessDocument2 pagesMcu-Fdt Medical Foundation Hospital Out Patient Services: Chief Complaint: History of Present IllnessvinbNo ratings yet
- 1 Pathogen Vs Antigen Activity - Pilar Julissa Ruiz ValdezDocument4 pages1 Pathogen Vs Antigen Activity - Pilar Julissa Ruiz Valdezapi-375915571No ratings yet
- Neonatal Respiratory DistressDocument54 pagesNeonatal Respiratory DistressMohamad Saleh100% (1)
- 1 Scrub 2 CircuDocument2 pages1 Scrub 2 CircuKatrina CaveNo ratings yet
- Gina Shenoda, BS, MBADocument3 pagesGina Shenoda, BS, MBACristian RamirezNo ratings yet
- BMH-NM Surgical Site Infection Reduction Poster 04162021Document1 pageBMH-NM Surgical Site Infection Reduction Poster 04162021Baptist Memorial Health CareNo ratings yet
- Medical EthicsDocument27 pagesMedical Ethicspriyarajan007No ratings yet
- Cefixime For Community Acquired InfectionDocument14 pagesCefixime For Community Acquired InfectionSupriNo ratings yet
- Consenso EUR TQTDocument12 pagesConsenso EUR TQTCamila Villalobos BravoNo ratings yet
- European Guidelines For Urinalysis A CollaborativeDocument7 pagesEuropean Guidelines For Urinalysis A CollaborativeTaufan LutfiNo ratings yet
- General-Luna Elem Districtschool NS Baseline Consolidation Sy2023-2024Document99 pagesGeneral-Luna Elem Districtschool NS Baseline Consolidation Sy2023-2024roseannurakNo ratings yet
- Risk Assessment For Working On or Near WaterDocument1 pageRisk Assessment For Working On or Near WaterRicardo Dalisay100% (2)
- Hepatitis E InfectionDocument27 pagesHepatitis E Infectiontummalapalli venkateswara raoNo ratings yet
- Carcinocin MateriaDocument6 pagesCarcinocin MateriassNo ratings yet