Download as pdf or txt
You might also like
- ACR EducationDocument53 pagesACR EducationamereNo ratings yet
- Terazosin Hytrin Drug CardDocument1 pageTerazosin Hytrin Drug CardSheri490No ratings yet
- Teaching PlanDocument2 pagesTeaching PlanalyNo ratings yet
- Genetic Variations in The Gene in Primary Aldosteronism Patients From Xinjiang, ChinaDocument6 pagesGenetic Variations in The Gene in Primary Aldosteronism Patients From Xinjiang, ChinaamnaNo ratings yet
- Hiperaldosterenismo PrimarioDocument10 pagesHiperaldosterenismo Primariobyrock66No ratings yet
- Articulo 2 YaDocument9 pagesArticulo 2 YaLaura EscobarNo ratings yet
- Artikel p2Document8 pagesArtikel p2Umi Darozah ZenNo ratings yet
- Acute Intermittent Porphyria - Clinicopathologic Correlation - Report of A Case and Review of The Literature (1997)Document7 pagesAcute Intermittent Porphyria - Clinicopathologic Correlation - Report of A Case and Review of The Literature (1997)Triple ANo ratings yet
- Global REACH 2018: Volume Regulation in High-Altitude Andeans With and Without Chronic Mountain SicknessDocument9 pagesGlobal REACH 2018: Volume Regulation in High-Altitude Andeans With and Without Chronic Mountain SicknessFiorella LeyvaNo ratings yet
- Optimal PH Strategy For Hypothermic Circulatory Ar PDFDocument2 pagesOptimal PH Strategy For Hypothermic Circulatory Ar PDFKhairunnisa FitriNo ratings yet
- AcuapurinasDocument7 pagesAcuapurinasLenner Urtecho CalderonNo ratings yet
- 2140 FullDocument8 pages2140 FullShukr Wesman BlbasNo ratings yet
- Del Toro 2006Document5 pagesDel Toro 2006NATALIA MARTINEZ CORDOBANo ratings yet
- Chong Et Al-2006-European Journal of Heart FailureDocument6 pagesChong Et Al-2006-European Journal of Heart FailureginaNo ratings yet
- Ferric Carboxymaltose in Patients With Heart Failure and Iron DeficiencyDocument13 pagesFerric Carboxymaltose in Patients With Heart Failure and Iron DeficiencyfathaNo ratings yet
- Effects of Candesartan and Amlodipine On Cardiovascular Events in Hypertensive Patients With Chronic Kidney DiseaseDocument8 pagesEffects of Candesartan and Amlodipine On Cardiovascular Events in Hypertensive Patients With Chronic Kidney Diseasenova sorayaNo ratings yet
- Awad 2003Document5 pagesAwad 2003Jansen ChNo ratings yet
- Small Interfering RNA To ReduceDocument10 pagesSmall Interfering RNA To ReduceMahmoud Abu MayalehNo ratings yet
- Copeptin, Insulin Resistance, and Risk of Incident Diabetes in Older MenDocument8 pagesCopeptin, Insulin Resistance, and Risk of Incident Diabetes in Older MenFrisilia LeauaNo ratings yet
- Corin and Left Atrial Cardiomyopathy, Hypertension, Arrhythmia, and FibrosisDocument8 pagesCorin and Left Atrial Cardiomyopathy, Hypertension, Arrhythmia, and FibrosisAdriana MoorNo ratings yet
- Left Ventricular Hypertrophy Is Associated With Inflammation in Sodium Loaded Subtotal Nephrectomized RatsDocument8 pagesLeft Ventricular Hypertrophy Is Associated With Inflammation in Sodium Loaded Subtotal Nephrectomized RatsLuis Marcas VilaNo ratings yet
- Rodriguez G - Serum ACE Activity in Normal Children and in Those With SarcoidosisDocument5 pagesRodriguez G - Serum ACE Activity in Normal Children and in Those With SarcoidosisPhaimNo ratings yet
- Glutathione Peroxidase 1 Activity and Cardiovascular Events in Patients With Coronary Artery DiseaseDocument9 pagesGlutathione Peroxidase 1 Activity and Cardiovascular Events in Patients With Coronary Artery Diseaseapi-26034055No ratings yet
- Abstracts / Atherosclerosis 252 (2016) E1 Ee196 E185Document2 pagesAbstracts / Atherosclerosis 252 (2016) E1 Ee196 E185MaulNo ratings yet
- CK and LBMDocument8 pagesCK and LBMSarathNo ratings yet
- Emerick Et Al 1999 HepatologyDocument8 pagesEmerick Et Al 1999 Hepatologyagustinus salimNo ratings yet
- Nejmoa 2211023Document10 pagesNejmoa 2211023EvelynNo ratings yet
- Madara PoisonDocument3 pagesMadara PoisonMillenium AyurvedaNo ratings yet
- Journal Jantung-2Document23 pagesJournal Jantung-2Achmad IstiyonoNo ratings yet
- Salt Sensitivity of Blood Pressure in NKCC1-deficient MiceDocument9 pagesSalt Sensitivity of Blood Pressure in NKCC1-deficient MiceHongyu LiNo ratings yet
- The Association Between Serum Uric Acid Level and Coronary Artery DiseaseDocument8 pagesThe Association Between Serum Uric Acid Level and Coronary Artery DiseasemikeNo ratings yet
- Citicoline Improved Cardiovascular Function in Animal Model of DysautonomiaDocument12 pagesCiticoline Improved Cardiovascular Function in Animal Model of DysautonomiaShaimaa NasrNo ratings yet
- The Effect of Combined Aerobic and Resistance Exercise Training On Vascular Function in Type 2 DiabetesDocument7 pagesThe Effect of Combined Aerobic and Resistance Exercise Training On Vascular Function in Type 2 DiabetesZINATUL WIDADNo ratings yet
- Primary Aldosteronism Caused by Unilateral Adrenal Hyperplasia: Rethinking The Accuracy of Imaging StudiesDocument5 pagesPrimary Aldosteronism Caused by Unilateral Adrenal Hyperplasia: Rethinking The Accuracy of Imaging StudiesRonald DelosendoNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- A Rare Cause of AA Amyloidosis and End-Stage Kidney Failure: QuestionsDocument3 pagesA Rare Cause of AA Amyloidosis and End-Stage Kidney Failure: QuestionsSezen YılmazNo ratings yet
- Role of Inflammation and Oxidative Stress in Atrial FibrillationDocument7 pagesRole of Inflammation and Oxidative Stress in Atrial FibrillationM Rizki FadlanNo ratings yet
- Li 2004Document8 pagesLi 2004Shukr Wesman BlbasNo ratings yet
- Comparison of The Plasma Levels of Apolipoproteins B and A-L, and Other Risk Factors in Men and Women With Premature Coronary Artery DiseaseDocument7 pagesComparison of The Plasma Levels of Apolipoproteins B and A-L, and Other Risk Factors in Men and Women With Premature Coronary Artery DiseaseCamilo HernándezNo ratings yet
- TMP AE98Document5 pagesTMP AE98FrontiersNo ratings yet
- Genome Wide Gene Expression Array Identifies NovelDocument16 pagesGenome Wide Gene Expression Array Identifies NovelAswin RNo ratings yet
- The Effect of Spironolactone Use On Heart Failure Mortality: A Population-Based StudyDocument5 pagesThe Effect of Spironolactone Use On Heart Failure Mortality: A Population-Based StudyRizkaFelinaNo ratings yet
- Where Hypertension Happens: CommentariesDocument4 pagesWhere Hypertension Happens: CommentariesIlvita MayasariNo ratings yet
- Age-Associated Changes in Electrophysiologic Remodeling: A Potential Contributor To Initiation of Atrial FibrillationDocument11 pagesAge-Associated Changes in Electrophysiologic Remodeling: A Potential Contributor To Initiation of Atrial FibrillationDr Nouf AlshwairaNo ratings yet
- Natural Selection On Genes Related To Cardiovascular Health in High-Altitude Adapted AndeansDocument16 pagesNatural Selection On Genes Related To Cardiovascular Health in High-Altitude Adapted AndeansokerNo ratings yet
- Anemia in Canine Chronic Kidney Disease Is Multifactorial2Document6 pagesAnemia in Canine Chronic Kidney Disease Is Multifactorial2vanessadllpNo ratings yet
- Hepatology - 2012 - Fede - Adrenocortical Dysfunction in Liver Disease A Systematic ReviewDocument10 pagesHepatology - 2012 - Fede - Adrenocortical Dysfunction in Liver Disease A Systematic ReviewJelena PaunovicNo ratings yet
- InnisDocument6 pagesInnisapi-289577018No ratings yet
- Yi 2006 ACE2 Polymorphisms in China HTDocument12 pagesYi 2006 ACE2 Polymorphisms in China HTGolden Era BookwormNo ratings yet
- Long QT Pada CSWSDocument6 pagesLong QT Pada CSWSSofie HanafiahNo ratings yet
- eNOS AND MIDocument7 pageseNOS AND MIShukr Wesman BlbasNo ratings yet
- Boss Ola 2009Document8 pagesBoss Ola 2009nettoxsNo ratings yet
- Prittie-2006-Journal of Veterinary Emergency and Critical CareDocument11 pagesPrittie-2006-Journal of Veterinary Emergency and Critical Carejose fdoNo ratings yet
- When Past Is Prologue: Clinical Problem-SolvingDocument7 pagesWhen Past Is Prologue: Clinical Problem-SolvingJoni WitziNo ratings yet
- Evaluationandmanagement Ofprimary Hyperaldosteronism: Frances T. Lee,, Dina ElarajDocument15 pagesEvaluationandmanagement Ofprimary Hyperaldosteronism: Frances T. Lee,, Dina ElarajDiego BallesterosNo ratings yet
- Effect of Curcumin On Inhibiting Atherogenesis by Down-Regulating Lipocalin-2 Expression in Apolipoprotein E Knockout MiceDocument11 pagesEffect of Curcumin On Inhibiting Atherogenesis by Down-Regulating Lipocalin-2 Expression in Apolipoprotein E Knockout MicemaulanaardhiNo ratings yet
- The Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFDocument6 pagesThe Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFmaciasdrNo ratings yet
- How Dangerous Is Hyperkalemia?Document11 pagesHow Dangerous Is Hyperkalemia?Erika SalazarNo ratings yet
- Serum Electrolyte Levels and Outcomes in Patients Hospitalized With Hepatic EncephalopathyDocument7 pagesSerum Electrolyte Levels and Outcomes in Patients Hospitalized With Hepatic EncephalopathyhimayatullahNo ratings yet
- Anastomosis Vol 1 Issue 2 PDFDocument36 pagesAnastomosis Vol 1 Issue 2 PDFRashin PNo ratings yet
- JAH3 7 E009890Document20 pagesJAH3 7 E009890Ganda AgylNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Jcem 4398Document5 pagesJcem 4398vegagbNo ratings yet
- Outcomesofpatientsundergoingsurgeryforprimaryaldosteronismbasedonadrenalvenoussamplingandradiology ESE2018Document6 pagesOutcomesofpatientsundergoingsurgeryforprimaryaldosteronismbasedonadrenalvenoussamplingandradiology ESE2018vegagbNo ratings yet
- 990 FullDocument7 pages990 FullvegagbNo ratings yet
- United States Patent: (10) Patent No .: US 9, 883, 909 B2Document29 pagesUnited States Patent: (10) Patent No .: US 9, 883, 909 B2vegagbNo ratings yet
- Sonicwall Analyzer: Application Traffic Analytics, Visualization and Reporting ToolDocument4 pagesSonicwall Analyzer: Application Traffic Analytics, Visualization and Reporting ToolvegagbNo ratings yet
- Filthy RagsDocument6 pagesFilthy RagsvegagbNo ratings yet
- The Story of Penicillin - University of Oxford PDFDocument3 pagesThe Story of Penicillin - University of Oxford PDFvegagbNo ratings yet
- A Call To Thought Purity: by Harold S. MartinDocument4 pagesA Call To Thought Purity: by Harold S. MartinvegagbNo ratings yet
- ACE InhibitorsDocument8 pagesACE InhibitorsJohn HillNo ratings yet
- Prediction of Preeclampsia Throughout Gestation With Maternal Characteristics and Biophysical and Biochemical Markers: A Longitudinal StudyDocument22 pagesPrediction of Preeclampsia Throughout Gestation With Maternal Characteristics and Biophysical and Biochemical Markers: A Longitudinal StudydhapitstinNo ratings yet
- Cardiovascular Diseases (CVD) Greatly Threaten Filipinos Today. The Filipino Faces The Risk ofDocument8 pagesCardiovascular Diseases (CVD) Greatly Threaten Filipinos Today. The Filipino Faces The Risk ofHikari 光 ShidouNo ratings yet
- Prototype Histories (Clerking) .Document51 pagesPrototype Histories (Clerking) .IgbashioNo ratings yet
- Pregnancy Induced HypertensionDocument25 pagesPregnancy Induced HypertensionPauPauNo ratings yet
- Pengaruh Terapi Emotional Freedom Technique (EFT) Terhadap Depresi Pada Klien Hipertensi (The Effect Emotional Freedom Technique (EFT) Therapy OnDocument8 pagesPengaruh Terapi Emotional Freedom Technique (EFT) Terhadap Depresi Pada Klien Hipertensi (The Effect Emotional Freedom Technique (EFT) Therapy OnHellyatill HasanahNo ratings yet
- UWORLDNCLEXreview2021 PDFDocument100 pagesUWORLDNCLEXreview2021 PDFmahshid kianiNo ratings yet
- Isman Firdaus, DR, SP - JP (K), FIHA: QualificationDocument38 pagesIsman Firdaus, DR, SP - JP (K), FIHA: QualificationGhinna Septhiana PratiwiNo ratings yet
- Medicinal Uses of Elaichi or CardamomDocument11 pagesMedicinal Uses of Elaichi or CardamomjnaguNo ratings yet
- Final ProposalDocument5 pagesFinal ProposalKs ZaraNo ratings yet
- Targeted Weight Reduction Using Sibutramine.Document4 pagesTargeted Weight Reduction Using Sibutramine.International Medical PublisherNo ratings yet
- Losartan Plus HydrochlorothiazideDocument18 pagesLosartan Plus Hydrochlorothiazidegmsanto7No ratings yet
- Hypertension in ChildrenDocument32 pagesHypertension in ChildrenmikhaelyosiaNo ratings yet
- Cor PulmonaleDocument33 pagesCor PulmonaleSanda AnaNo ratings yet
- CF SharpDocument13 pagesCF Sharpluiz ManieboNo ratings yet
- Vi. Anatomy and Physiology: Anatomical Structures and Physiology of The Affected Body Organ/ SystemsDocument18 pagesVi. Anatomy and Physiology: Anatomical Structures and Physiology of The Affected Body Organ/ SystemsZhailyn Joy DumlaoNo ratings yet
- SIMI - Volume Comunicazioni Orali e PosterDocument212 pagesSIMI - Volume Comunicazioni Orali e Postermaria wahyuniNo ratings yet
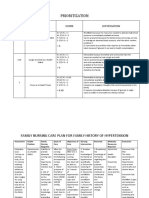
- Family Nursing Care Plan HypertensionDocument4 pagesFamily Nursing Care Plan HypertensionDarlene Joy AquinoNo ratings yet
- Acupuncture Miriam Lee - Yin and Yang - HeartDocument24 pagesAcupuncture Miriam Lee - Yin and Yang - HeartAurora Alina Bujor-FlueranNo ratings yet
- Ministry of Home Affairs Circular (English)Document5 pagesMinistry of Home Affairs Circular (English)umahsuthanNo ratings yet
- Environmental Noise and Sleep DisturbancesDocument4 pagesEnvironmental Noise and Sleep DisturbancesCamilo PalacioNo ratings yet
- Guias Hipertension 2023 Esc AnalisisDocument12 pagesGuias Hipertension 2023 Esc Analisismiguel contrerasNo ratings yet
- IGNOU Block 4 Unit 2 Non-Communicable Diseases 1Document20 pagesIGNOU Block 4 Unit 2 Non-Communicable Diseases 1erice.researchNo ratings yet
- Co Q10Document29 pagesCo Q10ags375No ratings yet
- 2023 ESH Hypertension Guideline Update - Bringing Us Closer Together Across The Pond - American College of CardiologyDocument7 pages2023 ESH Hypertension Guideline Update - Bringing Us Closer Together Across The Pond - American College of Cardiologyhalticabral2022No ratings yet
- HB Sands Seniors Huntington BeachDocument28 pagesHB Sands Seniors Huntington BeachHBNewsPressNo ratings yet
- @enmagazine Psr7bcdt2ridkoDocument28 pages@enmagazine Psr7bcdt2ridkorahulNo ratings yet