
Chemotherapeutics 1
Chemotherapeutics 1
You might also like
- Scientology: Integrity and HonestyDocument41 pagesScientology: Integrity and HonestyOfficial Church of Scientology86% (7)
- Bruno Groening Teachings PDFDocument6 pagesBruno Groening Teachings PDFAnonymous AHIfjTqLFlNo ratings yet
- Antibacterial DrugsDocument48 pagesAntibacterial DrugsDarlington Dimitri (zeecomedy)No ratings yet
- Unit 4Document111 pagesUnit 4Bea Bianca CruzNo ratings yet
- Antibiotics and VaccinesDocument19 pagesAntibiotics and Vaccineslarphs214No ratings yet
- Am and Amr 2020Document46 pagesAm and Amr 2020Mikhael JHNo ratings yet
- Lac 10&11 PPTDocument16 pagesLac 10&11 PPTRaghdaNo ratings yet
- L16 Antibiotics - in - Oral - Maxillofacial - SurgeryDocument75 pagesL16 Antibiotics - in - Oral - Maxillofacial - SurgeryJu JuNo ratings yet
- DP On AglDocument12 pagesDP On AglDeepikaNo ratings yet
- Mechanism of Action of Antibiotics: Subject:Pharmaceutical Microbiology DATE:18/09/2019Document12 pagesMechanism of Action of Antibiotics: Subject:Pharmaceutical Microbiology DATE:18/09/2019rubyNo ratings yet
- Chapter 9 Surgical Infections and Antibiotic SelectionDocument42 pagesChapter 9 Surgical Infections and Antibiotic SelectionSteven Mark MananguNo ratings yet
- Antibacterial Drugs: B.K. SatriyasaDocument56 pagesAntibacterial Drugs: B.K. SatriyasaVicNo ratings yet
- Antifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Document37 pagesAntifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Hafsat JimetaNo ratings yet
- Pharma Part 1 and 2Document10 pagesPharma Part 1 and 2BRYCE WILLIAM GONo ratings yet
- AntibioticsDocument63 pagesAntibioticsSahin mollickNo ratings yet
- Inhibitor of Bacterial Protein SynthesisDocument83 pagesInhibitor of Bacterial Protein SynthesisNdayisaba CorneilleNo ratings yet
- AntibioticsDocument64 pagesAntibioticsogatojohnsonNo ratings yet
- Antimicrobial Agent: DR Retno Budiarti M.Kes Microbiology Department FK UhtDocument43 pagesAntimicrobial Agent: DR Retno Budiarti M.Kes Microbiology Department FK UhtAlunaficha Melody KiraniaNo ratings yet
- Antmicrobial AgentDocument93 pagesAntmicrobial Agentdrnuaman5No ratings yet
- Newer Antibiotics: Guide: DR Saroja A ODocument51 pagesNewer Antibiotics: Guide: DR Saroja A OparahulNo ratings yet
- Lincosamides (Pharmacology of Antibiotics) - Group 6 PresentationDocument19 pagesLincosamides (Pharmacology of Antibiotics) - Group 6 PresentationGelmark OlivaresNo ratings yet
- Pharma 14 To 23Document298 pagesPharma 14 To 23Loai Mohammed IssaNo ratings yet
- Drugs To Control InfectionDocument14 pagesDrugs To Control InfectionkristiannedenNo ratings yet
- AntibioticsDocument84 pagesAntibioticsNandini GulurNo ratings yet
- Antibacterial Class 03Document80 pagesAntibacterial Class 03tsegaab yosephNo ratings yet
- 5 AminoglycosidesDocument7 pages5 AminoglycosidesNashat SaadiNo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- Antibiotics en NurseDocument118 pagesAntibiotics en Nurseabsolomon777No ratings yet
- PharmaDocument16 pagesPharmaPaula Grace MorfeNo ratings yet
- Using Antimicrobial Agents To Control Mirobial Growth in VivoDocument39 pagesUsing Antimicrobial Agents To Control Mirobial Growth in VivoHannah BuquironNo ratings yet
- Sterilization and DisinfectionDocument65 pagesSterilization and DisinfectionJohn Marlou De GuzmanNo ratings yet
- Antibiotics 1Document64 pagesAntibiotics 1Justin Ancog100% (1)
- Anti Infectives 3Document74 pagesAnti Infectives 3Clarise MoringNo ratings yet
- AntimicrobialsDocument130 pagesAntimicrobialsPATRICK ROSHAN ANo ratings yet
- Damage To Cell MembraneDocument7 pagesDamage To Cell MembraneEsteph CortesNo ratings yet
- Chapter 10. ChemotherapyDocument157 pagesChapter 10. ChemotherapyAbel GirmaNo ratings yet
- Chapter 044Document5 pagesChapter 044borisdevic223No ratings yet
- Antibiotic, Anti-Infective Antimicrobials Drugs: Antimicrobial Drugs Class Mode of ActionsDocument16 pagesAntibiotic, Anti-Infective Antimicrobials Drugs: Antimicrobial Drugs Class Mode of ActionsBSN FilesNo ratings yet
- Inhibiting The Growth of Pathogens in VivoDocument25 pagesInhibiting The Growth of Pathogens in VivoRoshwell RegalaNo ratings yet
- ANTIBIOTICS Pharmacology NursingDocument10 pagesANTIBIOTICS Pharmacology NursingRalph Alfonse De JesusNo ratings yet
- Introduction To Antimicrobials Page 1 of 6Document6 pagesIntroduction To Antimicrobials Page 1 of 6Hassan.shehriNo ratings yet
- Antimicrobial Pharmacology 9Document164 pagesAntimicrobial Pharmacology 9elias adugnaNo ratings yet
- Basics of AntibioticsDocument42 pagesBasics of AntibioticsAsma BakheitNo ratings yet
- Antibiotics: Presenter: Naila InamDocument41 pagesAntibiotics: Presenter: Naila InamInam KhanNo ratings yet
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- B LactamAntibioticsDocument63 pagesB LactamAntibioticsNishant NamdeoNo ratings yet
- Antimicrobial DrugsDocument63 pagesAntimicrobial DrugsRonalyn UgatNo ratings yet
- AMINOGLYCOSIDESDocument45 pagesAMINOGLYCOSIDESAbdullah EmadNo ratings yet
- Antibiotics in Veterinary UseDocument83 pagesAntibiotics in Veterinary Usehansmeet100% (1)
- AMINOGLYCOSIDEDocument18 pagesAMINOGLYCOSIDEVinayKumarNo ratings yet
- Medmastery Antimicrobial - Stewardship - HandbookDocument65 pagesMedmastery Antimicrobial - Stewardship - HandbookHhaNo ratings yet
- Summary On All The Important Points in AntibioticsDocument38 pagesSummary On All The Important Points in Antibioticsrozaadil99No ratings yet
- Protein Synthesis Inhibitors 1Document23 pagesProtein Synthesis Inhibitors 1Johnathan DevidNo ratings yet
- Antimicrobial Drugs: Eti Nurwening SholikhahDocument50 pagesAntimicrobial Drugs: Eti Nurwening SholikhahYogi SetiawanNo ratings yet
- Lecture Note Antibacterial AgentsDocument14 pagesLecture Note Antibacterial AgentsSimonNo ratings yet
- Microbiology Assignmentt TradeDocument14 pagesMicrobiology Assignmentt TradeADITYAROOP PATHAKNo ratings yet
- Chapter 12 Powerpoint LDocument50 pagesChapter 12 Powerpoint LDennis Nabor Muñoz, RN,RMNo ratings yet
- Antibacterial and Antiinfective AgentsDocument80 pagesAntibacterial and Antiinfective AgentsAbbeygale GalanNo ratings yet
- Approach To Antibiotics in SurgeryDocument30 pagesApproach To Antibiotics in SurgeryzahraaNo ratings yet
- (PHARMA A) 3.3 - Antibiotics I - Dr. Cruz (2024)Document15 pages(PHARMA A) 3.3 - Antibiotics I - Dr. Cruz (2024)Miguel Luis NavarreteNo ratings yet
- Antibiotics in Oral and Maxillofacial SurgeryDocument25 pagesAntibiotics in Oral and Maxillofacial Surgeryindian dental academyNo ratings yet
- Amoxicillin: A Beginner's 20-Minute Quick Guide Overview on its Use Cases to Treat Bacterial Infection and Side EffectsFrom EverandAmoxicillin: A Beginner's 20-Minute Quick Guide Overview on its Use Cases to Treat Bacterial Infection and Side EffectsNo ratings yet
- Hyperemesis Gravida Til Spontanous AbortionDocument24 pagesHyperemesis Gravida Til Spontanous AbortionDilausan B MolukNo ratings yet
- Result - 7 - 2 - 2023, 12 - 59 - 48 AMDocument1 pageResult - 7 - 2 - 2023, 12 - 59 - 48 AMDilausan B MolukNo ratings yet
- Pathophysiology: Physical ExaminationDocument2 pagesPathophysiology: Physical ExaminationDilausan B MolukNo ratings yet
- Gestational ConditionDocument26 pagesGestational ConditionDilausan B MolukNo ratings yet
- Probable CauseDocument4 pagesProbable CauseDilausan B MolukNo ratings yet
- Atrial SD PathoDocument1 pageAtrial SD PathoDilausan B MolukNo ratings yet
- Health ProblemDocument2 pagesHealth ProblemDilausan B MolukNo ratings yet
- ASD PathoDocument1 pageASD PathoDilausan B MolukNo ratings yet
- Fats: Saturated and UnsaturatedDocument6 pagesFats: Saturated and UnsaturatedDilausan B MolukNo ratings yet
- Analgesics Non-Narcotic Analgesics Non-Narcotic Analgesics Common Uses What I Need To Know As A Brand New NurseDocument2 pagesAnalgesics Non-Narcotic Analgesics Non-Narcotic Analgesics Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- Respiratory System Medications Respiratory System Meds Common Uses What I Need To Know As A Brand New NurseDocument2 pagesRespiratory System Medications Respiratory System Meds Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- Statistics For Analysis of Experimental Data: January 2001Document26 pagesStatistics For Analysis of Experimental Data: January 2001Dilausan B MolukNo ratings yet
- UntitledDocument2 pagesUntitledDilausan B MolukNo ratings yet
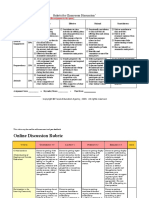
- Discussion Rubric ExamplesDocument6 pagesDiscussion Rubric ExamplesDilausan B MolukNo ratings yet
- Men'S Health Selected Men'S Health Agents Common Uses What I Need To Know As A Brand New NurseDocument1 pageMen'S Health Selected Men'S Health Agents Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- DocumentDocument1 pageDocumentDilausan B MolukNo ratings yet
- Renal System Diuretic Agents Common Uses What I Need To Know As A Brand New NurseDocument1 pageRenal System Diuretic Agents Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- Calamansis Are More Viable With Ecological Segments Than Manufactured PesticidesDocument1 pageCalamansis Are More Viable With Ecological Segments Than Manufactured PesticidesDilausan B MolukNo ratings yet
- UntitledDocument1 pageUntitledDilausan B MolukNo ratings yet
- My Has BeenDocument2 pagesMy Has BeenDilausan B MolukNo ratings yet
- Activity 11Document3 pagesActivity 11Dilausan B MolukNo ratings yet
- E-Policies, Activites and Grading SystemDocument3 pagesE-Policies, Activites and Grading SystemDilausan B MolukNo ratings yet
- Rhu d1 Compiled December LatestDocument169 pagesRhu d1 Compiled December LatestDilausan B MolukNo ratings yet
- DocumentDocument4 pagesDocumentDilausan B MolukNo ratings yet
- Pregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDocument5 pagesPregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDilausan B MolukNo ratings yet
- Comprehensive ReportDocument4 pagesComprehensive ReportDilausan B MolukNo ratings yet
- Citibank Vs Sps CabamonganDocument10 pagesCitibank Vs Sps CabamonganNovo FarmsNo ratings yet
- JJ205 Engineering Mechanics - Case Study 2 - Different Between Ac Motor and DC MotorDocument6 pagesJJ205 Engineering Mechanics - Case Study 2 - Different Between Ac Motor and DC MotorabidsufianNo ratings yet
- People Vs VillacortaDocument2 pagesPeople Vs VillacortaAma LakwatseraNo ratings yet
- 10 Hadiths On Self-Help PDFDocument28 pages10 Hadiths On Self-Help PDFStudij2011100% (1)
- A Report On: Application of Big Data and Business Analytics in Fashion IndustryDocument9 pagesA Report On: Application of Big Data and Business Analytics in Fashion IndustryAadarsh MahajanNo ratings yet
- S&C JDDocument6 pagesS&C JDAarzooMinza khanNo ratings yet
- WEEKLY HOME LEARNING PLAN (Esp 8)Document2 pagesWEEKLY HOME LEARNING PLAN (Esp 8)Grace Mary Tedlos Booc100% (1)
- Real Estate Development 5Th Edition Principles and Process Full ChapterDocument22 pagesReal Estate Development 5Th Edition Principles and Process Full Chaptermary.jauregui841100% (54)
- Serbian BeekeeperDocument52 pagesSerbian Beekeeperstormbrush100% (3)
- ASSIGMENT 2 ScribDocument14 pagesASSIGMENT 2 Scribruslanaziz100% (1)
- UML TutorialDocument9 pagesUML TutorialKadeKapoerNo ratings yet
- Escaler Vs CADocument4 pagesEscaler Vs CAjessapuerinNo ratings yet
- Clearing Vows and Contracts From The Akashic RecordsDocument3 pagesClearing Vows and Contracts From The Akashic Recordssbota100% (15)
- Latihan Soal Recount TextDocument5 pagesLatihan Soal Recount TextArty YuniarNo ratings yet
- DLL - MTB 3 - Q2 - W1Document3 pagesDLL - MTB 3 - Q2 - W1Esther LabariaNo ratings yet
- Eastern: Unit Northern and IndiaDocument11 pagesEastern: Unit Northern and IndiaPratima MukherjeeNo ratings yet
- CAE Multiple Choice Cloze 5Document7 pagesCAE Multiple Choice Cloze 5Sentido Común Alternativo SCANo ratings yet
- OG8 Journal 082316 For PrintDocument168 pagesOG8 Journal 082316 For PrintMarlon MagtiraNo ratings yet
- Benedict Joseph Labre LitanyDocument3 pagesBenedict Joseph Labre Litanydonmage100% (2)
- Hg-Module 1-Answer SheetsDocument4 pagesHg-Module 1-Answer SheetsMathPad with Teacher AnabelNo ratings yet
- EVoting SDS DocumentDocument58 pagesEVoting SDS DocumentKahfulwara MuhammadNo ratings yet
- CMDBuild AdministratorManual ENG V240Document134 pagesCMDBuild AdministratorManual ENG V240jesusferre2No ratings yet
- Exam June QuestionsDocument14 pagesExam June QuestionsQuynh Ngoc DangNo ratings yet
- 0905PPCDocument39 pages0905PPCsamir samiraNo ratings yet
- Requirements Analysis Document TemplateDocument11 pagesRequirements Analysis Document TemplateGiovanbattista CelatoNo ratings yet
- Grammar-Inversion ExercisesDocument2 pagesGrammar-Inversion ExercisesGeorgiaNo ratings yet
- Informative Speech Outline 1Document3 pagesInformative Speech Outline 1api-645506504No ratings yet
- Depression in Young People and The ElderlyDocument28 pagesDepression in Young People and The ElderlyJennyMae Ladica QueruelaNo ratings yet

















































































































Download as pdf or txt
You might also like
- Scientology: Integrity and HonestyDocument41 pagesScientology: Integrity and HonestyOfficial Church of Scientology86% (7)
- Bruno Groening Teachings PDFDocument6 pagesBruno Groening Teachings PDFAnonymous AHIfjTqLFlNo ratings yet
- Antibacterial DrugsDocument48 pagesAntibacterial DrugsDarlington Dimitri (zeecomedy)No ratings yet
- Unit 4Document111 pagesUnit 4Bea Bianca CruzNo ratings yet
- Antibiotics and VaccinesDocument19 pagesAntibiotics and Vaccineslarphs214No ratings yet
- Am and Amr 2020Document46 pagesAm and Amr 2020Mikhael JHNo ratings yet
- Lac 10&11 PPTDocument16 pagesLac 10&11 PPTRaghdaNo ratings yet
- L16 Antibiotics - in - Oral - Maxillofacial - SurgeryDocument75 pagesL16 Antibiotics - in - Oral - Maxillofacial - SurgeryJu JuNo ratings yet
- DP On AglDocument12 pagesDP On AglDeepikaNo ratings yet
- Mechanism of Action of Antibiotics: Subject:Pharmaceutical Microbiology DATE:18/09/2019Document12 pagesMechanism of Action of Antibiotics: Subject:Pharmaceutical Microbiology DATE:18/09/2019rubyNo ratings yet
- Chapter 9 Surgical Infections and Antibiotic SelectionDocument42 pagesChapter 9 Surgical Infections and Antibiotic SelectionSteven Mark MananguNo ratings yet
- Antibacterial Drugs: B.K. SatriyasaDocument56 pagesAntibacterial Drugs: B.K. SatriyasaVicNo ratings yet
- Antifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Document37 pagesAntifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Hafsat JimetaNo ratings yet
- Pharma Part 1 and 2Document10 pagesPharma Part 1 and 2BRYCE WILLIAM GONo ratings yet
- AntibioticsDocument63 pagesAntibioticsSahin mollickNo ratings yet
- Inhibitor of Bacterial Protein SynthesisDocument83 pagesInhibitor of Bacterial Protein SynthesisNdayisaba CorneilleNo ratings yet
- AntibioticsDocument64 pagesAntibioticsogatojohnsonNo ratings yet
- Antimicrobial Agent: DR Retno Budiarti M.Kes Microbiology Department FK UhtDocument43 pagesAntimicrobial Agent: DR Retno Budiarti M.Kes Microbiology Department FK UhtAlunaficha Melody KiraniaNo ratings yet
- Antmicrobial AgentDocument93 pagesAntmicrobial Agentdrnuaman5No ratings yet
- Newer Antibiotics: Guide: DR Saroja A ODocument51 pagesNewer Antibiotics: Guide: DR Saroja A OparahulNo ratings yet
- Lincosamides (Pharmacology of Antibiotics) - Group 6 PresentationDocument19 pagesLincosamides (Pharmacology of Antibiotics) - Group 6 PresentationGelmark OlivaresNo ratings yet
- Pharma 14 To 23Document298 pagesPharma 14 To 23Loai Mohammed IssaNo ratings yet
- Drugs To Control InfectionDocument14 pagesDrugs To Control InfectionkristiannedenNo ratings yet
- AntibioticsDocument84 pagesAntibioticsNandini GulurNo ratings yet
- Antibacterial Class 03Document80 pagesAntibacterial Class 03tsegaab yosephNo ratings yet
- 5 AminoglycosidesDocument7 pages5 AminoglycosidesNashat SaadiNo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- Antibiotics en NurseDocument118 pagesAntibiotics en Nurseabsolomon777No ratings yet
- PharmaDocument16 pagesPharmaPaula Grace MorfeNo ratings yet
- Using Antimicrobial Agents To Control Mirobial Growth in VivoDocument39 pagesUsing Antimicrobial Agents To Control Mirobial Growth in VivoHannah BuquironNo ratings yet
- Sterilization and DisinfectionDocument65 pagesSterilization and DisinfectionJohn Marlou De GuzmanNo ratings yet
- Antibiotics 1Document64 pagesAntibiotics 1Justin Ancog100% (1)
- Anti Infectives 3Document74 pagesAnti Infectives 3Clarise MoringNo ratings yet
- AntimicrobialsDocument130 pagesAntimicrobialsPATRICK ROSHAN ANo ratings yet
- Damage To Cell MembraneDocument7 pagesDamage To Cell MembraneEsteph CortesNo ratings yet
- Chapter 10. ChemotherapyDocument157 pagesChapter 10. ChemotherapyAbel GirmaNo ratings yet
- Chapter 044Document5 pagesChapter 044borisdevic223No ratings yet
- Antibiotic, Anti-Infective Antimicrobials Drugs: Antimicrobial Drugs Class Mode of ActionsDocument16 pagesAntibiotic, Anti-Infective Antimicrobials Drugs: Antimicrobial Drugs Class Mode of ActionsBSN FilesNo ratings yet
- Inhibiting The Growth of Pathogens in VivoDocument25 pagesInhibiting The Growth of Pathogens in VivoRoshwell RegalaNo ratings yet
- ANTIBIOTICS Pharmacology NursingDocument10 pagesANTIBIOTICS Pharmacology NursingRalph Alfonse De JesusNo ratings yet
- Introduction To Antimicrobials Page 1 of 6Document6 pagesIntroduction To Antimicrobials Page 1 of 6Hassan.shehriNo ratings yet
- Antimicrobial Pharmacology 9Document164 pagesAntimicrobial Pharmacology 9elias adugnaNo ratings yet
- Basics of AntibioticsDocument42 pagesBasics of AntibioticsAsma BakheitNo ratings yet
- Antibiotics: Presenter: Naila InamDocument41 pagesAntibiotics: Presenter: Naila InamInam KhanNo ratings yet
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- B LactamAntibioticsDocument63 pagesB LactamAntibioticsNishant NamdeoNo ratings yet
- Antimicrobial DrugsDocument63 pagesAntimicrobial DrugsRonalyn UgatNo ratings yet
- AMINOGLYCOSIDESDocument45 pagesAMINOGLYCOSIDESAbdullah EmadNo ratings yet
- Antibiotics in Veterinary UseDocument83 pagesAntibiotics in Veterinary Usehansmeet100% (1)
- AMINOGLYCOSIDEDocument18 pagesAMINOGLYCOSIDEVinayKumarNo ratings yet
- Medmastery Antimicrobial - Stewardship - HandbookDocument65 pagesMedmastery Antimicrobial - Stewardship - HandbookHhaNo ratings yet
- Summary On All The Important Points in AntibioticsDocument38 pagesSummary On All The Important Points in Antibioticsrozaadil99No ratings yet
- Protein Synthesis Inhibitors 1Document23 pagesProtein Synthesis Inhibitors 1Johnathan DevidNo ratings yet
- Antimicrobial Drugs: Eti Nurwening SholikhahDocument50 pagesAntimicrobial Drugs: Eti Nurwening SholikhahYogi SetiawanNo ratings yet
- Lecture Note Antibacterial AgentsDocument14 pagesLecture Note Antibacterial AgentsSimonNo ratings yet
- Microbiology Assignmentt TradeDocument14 pagesMicrobiology Assignmentt TradeADITYAROOP PATHAKNo ratings yet
- Chapter 12 Powerpoint LDocument50 pagesChapter 12 Powerpoint LDennis Nabor Muñoz, RN,RMNo ratings yet
- Antibacterial and Antiinfective AgentsDocument80 pagesAntibacterial and Antiinfective AgentsAbbeygale GalanNo ratings yet
- Approach To Antibiotics in SurgeryDocument30 pagesApproach To Antibiotics in SurgeryzahraaNo ratings yet
- (PHARMA A) 3.3 - Antibiotics I - Dr. Cruz (2024)Document15 pages(PHARMA A) 3.3 - Antibiotics I - Dr. Cruz (2024)Miguel Luis NavarreteNo ratings yet
- Antibiotics in Oral and Maxillofacial SurgeryDocument25 pagesAntibiotics in Oral and Maxillofacial Surgeryindian dental academyNo ratings yet
- Amoxicillin: A Beginner's 20-Minute Quick Guide Overview on its Use Cases to Treat Bacterial Infection and Side EffectsFrom EverandAmoxicillin: A Beginner's 20-Minute Quick Guide Overview on its Use Cases to Treat Bacterial Infection and Side EffectsNo ratings yet
- Hyperemesis Gravida Til Spontanous AbortionDocument24 pagesHyperemesis Gravida Til Spontanous AbortionDilausan B MolukNo ratings yet
- Result - 7 - 2 - 2023, 12 - 59 - 48 AMDocument1 pageResult - 7 - 2 - 2023, 12 - 59 - 48 AMDilausan B MolukNo ratings yet
- Pathophysiology: Physical ExaminationDocument2 pagesPathophysiology: Physical ExaminationDilausan B MolukNo ratings yet
- Gestational ConditionDocument26 pagesGestational ConditionDilausan B MolukNo ratings yet
- Probable CauseDocument4 pagesProbable CauseDilausan B MolukNo ratings yet
- Atrial SD PathoDocument1 pageAtrial SD PathoDilausan B MolukNo ratings yet
- Health ProblemDocument2 pagesHealth ProblemDilausan B MolukNo ratings yet
- ASD PathoDocument1 pageASD PathoDilausan B MolukNo ratings yet
- Fats: Saturated and UnsaturatedDocument6 pagesFats: Saturated and UnsaturatedDilausan B MolukNo ratings yet
- Analgesics Non-Narcotic Analgesics Non-Narcotic Analgesics Common Uses What I Need To Know As A Brand New NurseDocument2 pagesAnalgesics Non-Narcotic Analgesics Non-Narcotic Analgesics Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- Respiratory System Medications Respiratory System Meds Common Uses What I Need To Know As A Brand New NurseDocument2 pagesRespiratory System Medications Respiratory System Meds Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- Statistics For Analysis of Experimental Data: January 2001Document26 pagesStatistics For Analysis of Experimental Data: January 2001Dilausan B MolukNo ratings yet
- UntitledDocument2 pagesUntitledDilausan B MolukNo ratings yet
- Discussion Rubric ExamplesDocument6 pagesDiscussion Rubric ExamplesDilausan B MolukNo ratings yet
- Men'S Health Selected Men'S Health Agents Common Uses What I Need To Know As A Brand New NurseDocument1 pageMen'S Health Selected Men'S Health Agents Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- DocumentDocument1 pageDocumentDilausan B MolukNo ratings yet
- Renal System Diuretic Agents Common Uses What I Need To Know As A Brand New NurseDocument1 pageRenal System Diuretic Agents Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- Calamansis Are More Viable With Ecological Segments Than Manufactured PesticidesDocument1 pageCalamansis Are More Viable With Ecological Segments Than Manufactured PesticidesDilausan B MolukNo ratings yet
- UntitledDocument1 pageUntitledDilausan B MolukNo ratings yet
- My Has BeenDocument2 pagesMy Has BeenDilausan B MolukNo ratings yet
- Activity 11Document3 pagesActivity 11Dilausan B MolukNo ratings yet
- E-Policies, Activites and Grading SystemDocument3 pagesE-Policies, Activites and Grading SystemDilausan B MolukNo ratings yet
- Rhu d1 Compiled December LatestDocument169 pagesRhu d1 Compiled December LatestDilausan B MolukNo ratings yet
- DocumentDocument4 pagesDocumentDilausan B MolukNo ratings yet
- Pregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDocument5 pagesPregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDilausan B MolukNo ratings yet
- Comprehensive ReportDocument4 pagesComprehensive ReportDilausan B MolukNo ratings yet
- Citibank Vs Sps CabamonganDocument10 pagesCitibank Vs Sps CabamonganNovo FarmsNo ratings yet
- JJ205 Engineering Mechanics - Case Study 2 - Different Between Ac Motor and DC MotorDocument6 pagesJJ205 Engineering Mechanics - Case Study 2 - Different Between Ac Motor and DC MotorabidsufianNo ratings yet
- People Vs VillacortaDocument2 pagesPeople Vs VillacortaAma LakwatseraNo ratings yet
- 10 Hadiths On Self-Help PDFDocument28 pages10 Hadiths On Self-Help PDFStudij2011100% (1)
- A Report On: Application of Big Data and Business Analytics in Fashion IndustryDocument9 pagesA Report On: Application of Big Data and Business Analytics in Fashion IndustryAadarsh MahajanNo ratings yet
- S&C JDDocument6 pagesS&C JDAarzooMinza khanNo ratings yet
- WEEKLY HOME LEARNING PLAN (Esp 8)Document2 pagesWEEKLY HOME LEARNING PLAN (Esp 8)Grace Mary Tedlos Booc100% (1)
- Real Estate Development 5Th Edition Principles and Process Full ChapterDocument22 pagesReal Estate Development 5Th Edition Principles and Process Full Chaptermary.jauregui841100% (54)
- Serbian BeekeeperDocument52 pagesSerbian Beekeeperstormbrush100% (3)
- ASSIGMENT 2 ScribDocument14 pagesASSIGMENT 2 Scribruslanaziz100% (1)
- UML TutorialDocument9 pagesUML TutorialKadeKapoerNo ratings yet
- Escaler Vs CADocument4 pagesEscaler Vs CAjessapuerinNo ratings yet
- Clearing Vows and Contracts From The Akashic RecordsDocument3 pagesClearing Vows and Contracts From The Akashic Recordssbota100% (15)
- Latihan Soal Recount TextDocument5 pagesLatihan Soal Recount TextArty YuniarNo ratings yet
- DLL - MTB 3 - Q2 - W1Document3 pagesDLL - MTB 3 - Q2 - W1Esther LabariaNo ratings yet
- Eastern: Unit Northern and IndiaDocument11 pagesEastern: Unit Northern and IndiaPratima MukherjeeNo ratings yet
- CAE Multiple Choice Cloze 5Document7 pagesCAE Multiple Choice Cloze 5Sentido Común Alternativo SCANo ratings yet
- OG8 Journal 082316 For PrintDocument168 pagesOG8 Journal 082316 For PrintMarlon MagtiraNo ratings yet
- Benedict Joseph Labre LitanyDocument3 pagesBenedict Joseph Labre Litanydonmage100% (2)
- Hg-Module 1-Answer SheetsDocument4 pagesHg-Module 1-Answer SheetsMathPad with Teacher AnabelNo ratings yet
- EVoting SDS DocumentDocument58 pagesEVoting SDS DocumentKahfulwara MuhammadNo ratings yet
- CMDBuild AdministratorManual ENG V240Document134 pagesCMDBuild AdministratorManual ENG V240jesusferre2No ratings yet
- Exam June QuestionsDocument14 pagesExam June QuestionsQuynh Ngoc DangNo ratings yet
- 0905PPCDocument39 pages0905PPCsamir samiraNo ratings yet
- Requirements Analysis Document TemplateDocument11 pagesRequirements Analysis Document TemplateGiovanbattista CelatoNo ratings yet
- Grammar-Inversion ExercisesDocument2 pagesGrammar-Inversion ExercisesGeorgiaNo ratings yet
- Informative Speech Outline 1Document3 pagesInformative Speech Outline 1api-645506504No ratings yet
- Depression in Young People and The ElderlyDocument28 pagesDepression in Young People and The ElderlyJennyMae Ladica QueruelaNo ratings yet