
Effective Communication in Nursing
Effective Communication in Nursing
You might also like
- RPAH Elimination Diet Handbook With Food Shopping Guide PDFDocument33 pagesRPAH Elimination Diet Handbook With Food Shopping Guide PDFmalamatiyya33% (6)
- Effective Communication Skills in Nursing PracticeDocument7 pagesEffective Communication Skills in Nursing Practiceprisoner17100% (2)
- Makalah Manajemen CommunicationDocument16 pagesMakalah Manajemen CommunicationKhairunnisa FifiNo ratings yet
- Communication and Its BarriersDocument35 pagesCommunication and Its Barriersdibyendu_mondal67% (6)
- Effective Communication in NursingDocument19 pagesEffective Communication in Nursingyanuar anazdiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsPrassetya BebekNo ratings yet
- Pert 7 KLMPK 6Document25 pagesPert 7 KLMPK 6tata ydsNo ratings yet
- Nama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BDocument23 pagesNama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BEvina DianNo ratings yet
- Communication NEWDocument16 pagesCommunication NEWNawaloka NTSNo ratings yet
- Kelompok 8, 3a-1Document21 pagesKelompok 8, 3a-1Tyania MaharaniNo ratings yet
- Comunication& IprDocument24 pagesComunication& IprRaju67% (3)
- KD Boy WorkDocument17 pagesKD Boy WorkikebuakupearlNo ratings yet
- Communication ProcessDocument4 pagesCommunication Processdebora saroinsongNo ratings yet
- Thesis On Psychodynmic Traits in Adherence To Therapeutic Communication SkillsDocument22 pagesThesis On Psychodynmic Traits in Adherence To Therapeutic Communication SkillsLexa NalzaroNo ratings yet
- Therapeutic Com. Module StudentsDocument15 pagesTherapeutic Com. Module StudentsteuuuuNo ratings yet
- 1104 3528 1 PBDocument15 pages1104 3528 1 PBIqbal Rizky AnandaNo ratings yet
- Therapeutic Communication Book - 2nd Year - High InstituteDocument30 pagesTherapeutic Communication Book - 2nd Year - High InstituteSamantha Vera100% (1)
- Therapeutic CommunicationDocument15 pagesTherapeutic CommunicationIvy CalladaNo ratings yet
- Fed413 - Communications in Educational OrganisationsDocument4 pagesFed413 - Communications in Educational OrganisationsIbrahm ShosanyaNo ratings yet
- Nursing Management & Leadership: Unit II: CommunicationDocument37 pagesNursing Management & Leadership: Unit II: Communicationxr4dmNo ratings yet
- Preliminary: Noor Ariyani Rokhmah, AnggorowatiDocument2 pagesPreliminary: Noor Ariyani Rokhmah, AnggorowatiIta NovitaNo ratings yet
- SSB201 - Chapter 1Document16 pagesSSB201 - Chapter 1Tran Mai Khanh (K17 CT)No ratings yet
- Submitted To: Prof. Geetanjali Kapoor: CommunicationDocument10 pagesSubmitted To: Prof. Geetanjali Kapoor: CommunicationDeepali JadhavNo ratings yet
- AuditoriumDocument36 pagesAuditoriumAshrafNo ratings yet
- Communication and Interaction I Experienced Among Patients/clients/carersDocument8 pagesCommunication and Interaction I Experienced Among Patients/clients/carersRanzo FranqNo ratings yet
- Communication and Interpersonal RelationshipDocument20 pagesCommunication and Interpersonal RelationshipPinki BarmanNo ratings yet
- Communication and NPRDocument74 pagesCommunication and NPRabhishekkumar825245No ratings yet
- Therapeutic Communication Among Health ProfessionalsDocument4 pagesTherapeutic Communication Among Health ProfessionalsEsther OwusuNo ratings yet
- Competencies in English Communication Course NotesDocument52 pagesCompetencies in English Communication Course NotesIlie RomeoNo ratings yet
- Communication: Dr. Prakashkumar RathodDocument26 pagesCommunication: Dr. Prakashkumar RathodHafiz ShoaibNo ratings yet
- Communication Theories and Their Use in BusinessDocument49 pagesCommunication Theories and Their Use in BusinessshamielpeNo ratings yet
- Communication in A WorkplaceDocument18 pagesCommunication in A WorkplaceLeigh TenerosNo ratings yet
- BAB 1 - Komunikasi (English)Document64 pagesBAB 1 - Komunikasi (English)Conrad TarihoranNo ratings yet
- Role of Communication in Specific To Nursing ProfessionDocument12 pagesRole of Communication in Specific To Nursing ProfessionmsajaydeepakNo ratings yet
- Faisal Hossan - Introduction To Effective Caring - MJS - PPTDocument14 pagesFaisal Hossan - Introduction To Effective Caring - MJS - PPTJshadekNo ratings yet
- Unit 1 Communication: StructureDocument19 pagesUnit 1 Communication: StructureAnonymous zkruZiehlYNo ratings yet
- Av Aids File - FinalDocument58 pagesAv Aids File - FinalSindhu S NairNo ratings yet
- Communication in ExtensionDocument9 pagesCommunication in ExtensionVal Vincent M. LosariaNo ratings yet
- Lecture Notes On CEM 222 CommunicationDocument18 pagesLecture Notes On CEM 222 CommunicationAkubuike EluwaNo ratings yet
- Study Guide Psych Nursing 4Document14 pagesStudy Guide Psych Nursing 4christine mercadoNo ratings yet
- Communication Training ModuleDocument25 pagesCommunication Training ModuleMosneagu AndreeaNo ratings yet
- SSB201 - Slot 3Document17 pagesSSB201 - Slot 3phtrungtin2320No ratings yet
- Effective Communication SkillsDocument7 pagesEffective Communication SkillsArt Christian RamosNo ratings yet
- SSB201 - Slot 3Document17 pagesSSB201 - Slot 3Hoàng Thảo Vân NguyễnNo ratings yet
- Purposive Communication FinalDocument67 pagesPurposive Communication Finalentisar MaladoNo ratings yet
- Interaction Nursing Staff PDFDocument12 pagesInteraction Nursing Staff PDFLina SafitriNo ratings yet
- Managerial CommunicationDocument24 pagesManagerial CommunicationSai KiranNo ratings yet
- CommunicationDocument20 pagesCommunicationZoe FormosoNo ratings yet
- 1527055293H13CT03 Qi PDFDocument12 pages1527055293H13CT03 Qi PDFHarish KumarNo ratings yet
- CommunicationDocument18 pagesCommunicationAileen A. MonaresNo ratings yet
- CommunicationDocument5 pagesCommunicationSneha KhapraNo ratings yet
- Communication ProcessDocument21 pagesCommunication ProcessSheikh Gulzar AhmadNo ratings yet
- Wa0057.Document9 pagesWa0057.samyhager205No ratings yet
- CommunicationDocument76 pagesCommunicationShibili AbrahamNo ratings yet
- Assignment of Effective CommunicationDocument4 pagesAssignment of Effective CommunicationMd. Rashed Mahbub Sumon100% (4)
- Lesson 1-Overview of The Communication Process PDFDocument18 pagesLesson 1-Overview of The Communication Process PDFIchiroue Whan G100% (1)
- Concept and Theory Communication and Therapeutic CommunicationDocument22 pagesConcept and Theory Communication and Therapeutic CommunicationDzi Putri CiemNo ratings yet
- Communication ProcessDocument4 pagesCommunication Processanon_189062430No ratings yet
- Communication Skills For Medical Students: An Overview: Eview ArticleDocument7 pagesCommunication Skills For Medical Students: An Overview: Eview ArticleRazaria DailyneNo ratings yet
- Communication in Pa: Presented by Ansha Shamas Presented To Ma'am Farzana SyedDocument17 pagesCommunication in Pa: Presented by Ansha Shamas Presented To Ma'am Farzana Syedansha shamasNo ratings yet
- The Practitioners Handbook To Patient Communication From Theory To Practice: The Practitioners Handbook To Patient Communication From Theory To Practice, #4From EverandThe Practitioners Handbook To Patient Communication From Theory To Practice: The Practitioners Handbook To Patient Communication From Theory To Practice, #4No ratings yet
- Use of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyDocument5 pagesUse of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyRafael MartinsNo ratings yet
- Practice Guidelines For Telemental HealthDocument51 pagesPractice Guidelines For Telemental HealthNataanatiNo ratings yet
- UrinDocument2 pagesUrinaniaNo ratings yet
- Complete Hydatidiform MoleDocument1 pageComplete Hydatidiform MoleWilliam BarreraNo ratings yet
- Glycation of HemoglobinDocument3 pagesGlycation of Hemoglobinmadison DeliNo ratings yet
- File 819765613Document21 pagesFile 819765613tin tinNo ratings yet
- VA Emergency Care RulesDocument3 pagesVA Emergency Care RulesSunflower WilliamsNo ratings yet
- Sumaoang C. - Exercise No. 1 - Follow UpDocument3 pagesSumaoang C. - Exercise No. 1 - Follow UpBogartNo ratings yet
- Activity Intolerance NCPDocument2 pagesActivity Intolerance NCPrhieyan82% (11)
- MGN 522 (M+F) : Maritime and Coastguard AgencyDocument12 pagesMGN 522 (M+F) : Maritime and Coastguard AgencygeorgesagunaNo ratings yet
- AhmedabadDocument39 pagesAhmedabadacme financialNo ratings yet
- Virtual Planning of ImplantDocument6 pagesVirtual Planning of ImplantChekkarraj Sharanya KeshapurNo ratings yet
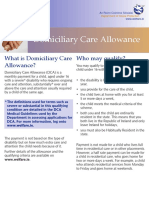
- What Is Domiciliary Care Allowance? Who May Qualify?Document4 pagesWhat Is Domiciliary Care Allowance? Who May Qualify?Alexandra IzsakNo ratings yet
- Mental Health EssayDocument5 pagesMental Health Essaycameronbullard2000No ratings yet
- New HookDocument5 pagesNew Hookhugeellis2No ratings yet
- Prayer House, 7 Elegbeleye Street, Ikosi, Ketu, Lagos: 0817 777 3285Document2 pagesPrayer House, 7 Elegbeleye Street, Ikosi, Ketu, Lagos: 0817 777 3285ChrisNo ratings yet
- Associations Between Content Types of Early Media Exposure and Subsequent Attentional ProblemsDocument9 pagesAssociations Between Content Types of Early Media Exposure and Subsequent Attentional ProblemsMaria Laurika SimatupangNo ratings yet
- Physical Inactivity TestDocument66 pagesPhysical Inactivity TestNHEMSTERS xoxoNo ratings yet
- Function and Role of DHODocument1 pageFunction and Role of DHOcopy smartNo ratings yet
- Journal of Nutrition College, Volume 5, Nomor 1, Tahun 2016Document8 pagesJournal of Nutrition College, Volume 5, Nomor 1, Tahun 2016Wiwik UliyaniNo ratings yet
- Michael Vance AutopsyDocument9 pagesMichael Vance AutopsyOKCFOXNo ratings yet
- Concepts in Health & Disease: K.Sagar Asso ProfessorDocument86 pagesConcepts in Health & Disease: K.Sagar Asso Professorkuruvagadda sagarNo ratings yet
- 14 QuestionnaireDocument8 pages14 QuestionnaireKutral EeswaranNo ratings yet
- 74-Other Professional, Scientific and Technical ActivitiesDocument4 pages74-Other Professional, Scientific and Technical ActivitiesCrazed NinjaNo ratings yet
- 2017-05-01 Final Nystatin Notice To Customer Letter PDFDocument2 pages2017-05-01 Final Nystatin Notice To Customer Letter PDFsaidvaretNo ratings yet
- Physical Therapy Protocol Shoulder Rotator Cuff Repair 26dec17Document2 pagesPhysical Therapy Protocol Shoulder Rotator Cuff Repair 26dec17LeonardoValenzuelaNo ratings yet
- Read Tiny Habits Online by BJ Fogg - BooksDocument5 pagesRead Tiny Habits Online by BJ Fogg - BookssamKaravana2No ratings yet
- Lean in 13 Presentation 2Document22 pagesLean in 13 Presentation 2ahosier100% (3)
- Hatchery Brochure PDFDocument8 pagesHatchery Brochure PDFUmair ShafiqueNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- RPAH Elimination Diet Handbook With Food Shopping Guide PDFDocument33 pagesRPAH Elimination Diet Handbook With Food Shopping Guide PDFmalamatiyya33% (6)
- Effective Communication Skills in Nursing PracticeDocument7 pagesEffective Communication Skills in Nursing Practiceprisoner17100% (2)
- Makalah Manajemen CommunicationDocument16 pagesMakalah Manajemen CommunicationKhairunnisa FifiNo ratings yet
- Communication and Its BarriersDocument35 pagesCommunication and Its Barriersdibyendu_mondal67% (6)
- Effective Communication in NursingDocument19 pagesEffective Communication in Nursingyanuar anazdiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsPrassetya BebekNo ratings yet
- Pert 7 KLMPK 6Document25 pagesPert 7 KLMPK 6tata ydsNo ratings yet
- Nama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BDocument23 pagesNama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BEvina DianNo ratings yet
- Communication NEWDocument16 pagesCommunication NEWNawaloka NTSNo ratings yet
- Kelompok 8, 3a-1Document21 pagesKelompok 8, 3a-1Tyania MaharaniNo ratings yet
- Comunication& IprDocument24 pagesComunication& IprRaju67% (3)
- KD Boy WorkDocument17 pagesKD Boy WorkikebuakupearlNo ratings yet
- Communication ProcessDocument4 pagesCommunication Processdebora saroinsongNo ratings yet
- Thesis On Psychodynmic Traits in Adherence To Therapeutic Communication SkillsDocument22 pagesThesis On Psychodynmic Traits in Adherence To Therapeutic Communication SkillsLexa NalzaroNo ratings yet
- Therapeutic Com. Module StudentsDocument15 pagesTherapeutic Com. Module StudentsteuuuuNo ratings yet
- 1104 3528 1 PBDocument15 pages1104 3528 1 PBIqbal Rizky AnandaNo ratings yet
- Therapeutic Communication Book - 2nd Year - High InstituteDocument30 pagesTherapeutic Communication Book - 2nd Year - High InstituteSamantha Vera100% (1)
- Therapeutic CommunicationDocument15 pagesTherapeutic CommunicationIvy CalladaNo ratings yet
- Fed413 - Communications in Educational OrganisationsDocument4 pagesFed413 - Communications in Educational OrganisationsIbrahm ShosanyaNo ratings yet
- Nursing Management & Leadership: Unit II: CommunicationDocument37 pagesNursing Management & Leadership: Unit II: Communicationxr4dmNo ratings yet
- Preliminary: Noor Ariyani Rokhmah, AnggorowatiDocument2 pagesPreliminary: Noor Ariyani Rokhmah, AnggorowatiIta NovitaNo ratings yet
- SSB201 - Chapter 1Document16 pagesSSB201 - Chapter 1Tran Mai Khanh (K17 CT)No ratings yet
- Submitted To: Prof. Geetanjali Kapoor: CommunicationDocument10 pagesSubmitted To: Prof. Geetanjali Kapoor: CommunicationDeepali JadhavNo ratings yet
- AuditoriumDocument36 pagesAuditoriumAshrafNo ratings yet
- Communication and Interaction I Experienced Among Patients/clients/carersDocument8 pagesCommunication and Interaction I Experienced Among Patients/clients/carersRanzo FranqNo ratings yet
- Communication and Interpersonal RelationshipDocument20 pagesCommunication and Interpersonal RelationshipPinki BarmanNo ratings yet
- Communication and NPRDocument74 pagesCommunication and NPRabhishekkumar825245No ratings yet
- Therapeutic Communication Among Health ProfessionalsDocument4 pagesTherapeutic Communication Among Health ProfessionalsEsther OwusuNo ratings yet
- Competencies in English Communication Course NotesDocument52 pagesCompetencies in English Communication Course NotesIlie RomeoNo ratings yet
- Communication: Dr. Prakashkumar RathodDocument26 pagesCommunication: Dr. Prakashkumar RathodHafiz ShoaibNo ratings yet
- Communication Theories and Their Use in BusinessDocument49 pagesCommunication Theories and Their Use in BusinessshamielpeNo ratings yet
- Communication in A WorkplaceDocument18 pagesCommunication in A WorkplaceLeigh TenerosNo ratings yet
- BAB 1 - Komunikasi (English)Document64 pagesBAB 1 - Komunikasi (English)Conrad TarihoranNo ratings yet
- Role of Communication in Specific To Nursing ProfessionDocument12 pagesRole of Communication in Specific To Nursing ProfessionmsajaydeepakNo ratings yet
- Faisal Hossan - Introduction To Effective Caring - MJS - PPTDocument14 pagesFaisal Hossan - Introduction To Effective Caring - MJS - PPTJshadekNo ratings yet
- Unit 1 Communication: StructureDocument19 pagesUnit 1 Communication: StructureAnonymous zkruZiehlYNo ratings yet
- Av Aids File - FinalDocument58 pagesAv Aids File - FinalSindhu S NairNo ratings yet
- Communication in ExtensionDocument9 pagesCommunication in ExtensionVal Vincent M. LosariaNo ratings yet
- Lecture Notes On CEM 222 CommunicationDocument18 pagesLecture Notes On CEM 222 CommunicationAkubuike EluwaNo ratings yet
- Study Guide Psych Nursing 4Document14 pagesStudy Guide Psych Nursing 4christine mercadoNo ratings yet
- Communication Training ModuleDocument25 pagesCommunication Training ModuleMosneagu AndreeaNo ratings yet
- SSB201 - Slot 3Document17 pagesSSB201 - Slot 3phtrungtin2320No ratings yet
- Effective Communication SkillsDocument7 pagesEffective Communication SkillsArt Christian RamosNo ratings yet
- SSB201 - Slot 3Document17 pagesSSB201 - Slot 3Hoàng Thảo Vân NguyễnNo ratings yet
- Purposive Communication FinalDocument67 pagesPurposive Communication Finalentisar MaladoNo ratings yet
- Interaction Nursing Staff PDFDocument12 pagesInteraction Nursing Staff PDFLina SafitriNo ratings yet
- Managerial CommunicationDocument24 pagesManagerial CommunicationSai KiranNo ratings yet
- CommunicationDocument20 pagesCommunicationZoe FormosoNo ratings yet
- 1527055293H13CT03 Qi PDFDocument12 pages1527055293H13CT03 Qi PDFHarish KumarNo ratings yet
- CommunicationDocument18 pagesCommunicationAileen A. MonaresNo ratings yet
- CommunicationDocument5 pagesCommunicationSneha KhapraNo ratings yet
- Communication ProcessDocument21 pagesCommunication ProcessSheikh Gulzar AhmadNo ratings yet
- Wa0057.Document9 pagesWa0057.samyhager205No ratings yet
- CommunicationDocument76 pagesCommunicationShibili AbrahamNo ratings yet
- Assignment of Effective CommunicationDocument4 pagesAssignment of Effective CommunicationMd. Rashed Mahbub Sumon100% (4)
- Lesson 1-Overview of The Communication Process PDFDocument18 pagesLesson 1-Overview of The Communication Process PDFIchiroue Whan G100% (1)
- Concept and Theory Communication and Therapeutic CommunicationDocument22 pagesConcept and Theory Communication and Therapeutic CommunicationDzi Putri CiemNo ratings yet
- Communication ProcessDocument4 pagesCommunication Processanon_189062430No ratings yet
- Communication Skills For Medical Students: An Overview: Eview ArticleDocument7 pagesCommunication Skills For Medical Students: An Overview: Eview ArticleRazaria DailyneNo ratings yet
- Communication in Pa: Presented by Ansha Shamas Presented To Ma'am Farzana SyedDocument17 pagesCommunication in Pa: Presented by Ansha Shamas Presented To Ma'am Farzana Syedansha shamasNo ratings yet
- The Practitioners Handbook To Patient Communication From Theory To Practice: The Practitioners Handbook To Patient Communication From Theory To Practice, #4From EverandThe Practitioners Handbook To Patient Communication From Theory To Practice: The Practitioners Handbook To Patient Communication From Theory To Practice, #4No ratings yet
- Use of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyDocument5 pagesUse of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyRafael MartinsNo ratings yet
- Practice Guidelines For Telemental HealthDocument51 pagesPractice Guidelines For Telemental HealthNataanatiNo ratings yet
- UrinDocument2 pagesUrinaniaNo ratings yet
- Complete Hydatidiform MoleDocument1 pageComplete Hydatidiform MoleWilliam BarreraNo ratings yet
- Glycation of HemoglobinDocument3 pagesGlycation of Hemoglobinmadison DeliNo ratings yet
- File 819765613Document21 pagesFile 819765613tin tinNo ratings yet
- VA Emergency Care RulesDocument3 pagesVA Emergency Care RulesSunflower WilliamsNo ratings yet
- Sumaoang C. - Exercise No. 1 - Follow UpDocument3 pagesSumaoang C. - Exercise No. 1 - Follow UpBogartNo ratings yet
- Activity Intolerance NCPDocument2 pagesActivity Intolerance NCPrhieyan82% (11)
- MGN 522 (M+F) : Maritime and Coastguard AgencyDocument12 pagesMGN 522 (M+F) : Maritime and Coastguard AgencygeorgesagunaNo ratings yet
- AhmedabadDocument39 pagesAhmedabadacme financialNo ratings yet
- Virtual Planning of ImplantDocument6 pagesVirtual Planning of ImplantChekkarraj Sharanya KeshapurNo ratings yet
- What Is Domiciliary Care Allowance? Who May Qualify?Document4 pagesWhat Is Domiciliary Care Allowance? Who May Qualify?Alexandra IzsakNo ratings yet
- Mental Health EssayDocument5 pagesMental Health Essaycameronbullard2000No ratings yet
- New HookDocument5 pagesNew Hookhugeellis2No ratings yet
- Prayer House, 7 Elegbeleye Street, Ikosi, Ketu, Lagos: 0817 777 3285Document2 pagesPrayer House, 7 Elegbeleye Street, Ikosi, Ketu, Lagos: 0817 777 3285ChrisNo ratings yet
- Associations Between Content Types of Early Media Exposure and Subsequent Attentional ProblemsDocument9 pagesAssociations Between Content Types of Early Media Exposure and Subsequent Attentional ProblemsMaria Laurika SimatupangNo ratings yet
- Physical Inactivity TestDocument66 pagesPhysical Inactivity TestNHEMSTERS xoxoNo ratings yet
- Function and Role of DHODocument1 pageFunction and Role of DHOcopy smartNo ratings yet
- Journal of Nutrition College, Volume 5, Nomor 1, Tahun 2016Document8 pagesJournal of Nutrition College, Volume 5, Nomor 1, Tahun 2016Wiwik UliyaniNo ratings yet
- Michael Vance AutopsyDocument9 pagesMichael Vance AutopsyOKCFOXNo ratings yet
- Concepts in Health & Disease: K.Sagar Asso ProfessorDocument86 pagesConcepts in Health & Disease: K.Sagar Asso Professorkuruvagadda sagarNo ratings yet
- 14 QuestionnaireDocument8 pages14 QuestionnaireKutral EeswaranNo ratings yet
- 74-Other Professional, Scientific and Technical ActivitiesDocument4 pages74-Other Professional, Scientific and Technical ActivitiesCrazed NinjaNo ratings yet
- 2017-05-01 Final Nystatin Notice To Customer Letter PDFDocument2 pages2017-05-01 Final Nystatin Notice To Customer Letter PDFsaidvaretNo ratings yet
- Physical Therapy Protocol Shoulder Rotator Cuff Repair 26dec17Document2 pagesPhysical Therapy Protocol Shoulder Rotator Cuff Repair 26dec17LeonardoValenzuelaNo ratings yet
- Read Tiny Habits Online by BJ Fogg - BooksDocument5 pagesRead Tiny Habits Online by BJ Fogg - BookssamKaravana2No ratings yet
- Lean in 13 Presentation 2Document22 pagesLean in 13 Presentation 2ahosier100% (3)
- Hatchery Brochure PDFDocument8 pagesHatchery Brochure PDFUmair ShafiqueNo ratings yet