Download as pdf or txt
You might also like
- Hypertension Concept MapDocument1 pageHypertension Concept Mapashleydean100% (7)
- P2 Top 200 Part 1Document10 pagesP2 Top 200 Part 1Drashtibahen PatelNo ratings yet
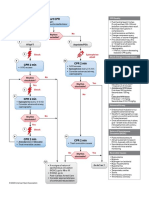
- Adult Cardiac Arrest Algorithm: VF/PVT Asystole/PEADocument8 pagesAdult Cardiac Arrest Algorithm: VF/PVT Asystole/PEAVitor Hugo100% (3)
- Algo ArrestDocument2 pagesAlgo ArrestLocomotorica FK UkiNo ratings yet
- Antidote Chart: N-Acetylcysteine, NAC (Mucomyst) PO: Loading Dose: 140mg/kg PO: NauseaDocument11 pagesAntidote Chart: N-Acetylcysteine, NAC (Mucomyst) PO: Loading Dose: 140mg/kg PO: NauseaTapioca PearlNo ratings yet
- Jane Detailed Lesson PlanDocument8 pagesJane Detailed Lesson PlanYe ShuaNo ratings yet
- L7. Autonomic Nervous System (ANS) IIDocument8 pagesL7. Autonomic Nervous System (ANS) IIsabahNo ratings yet
- Week 5Document5 pagesWeek 5Joanna BakNo ratings yet
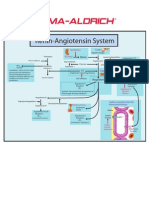
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- L11. GIT - Respiratory Tract DrugsDocument14 pagesL11. GIT - Respiratory Tract DrugssabahNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- UrologyDocument5 pagesUrologyJoshua AtienzaNo ratings yet
- ACLS 2015 Algorithm and Anesthesia ACLS PDFDocument14 pagesACLS 2015 Algorithm and Anesthesia ACLS PDFTaufiqurrahman RizkiNo ratings yet
- Antidote Toxic Exposure Indication Dose Lab Monitoring Adverse Rxns CommentsDocument5 pagesAntidote Toxic Exposure Indication Dose Lab Monitoring Adverse Rxns CommentsAjie FloridaNo ratings yet
- (BatMC MedSurg) Palma - NCPDocument4 pages(BatMC MedSurg) Palma - NCPJann Reinna PALMANo ratings yet
- Drug-Study ErgonDocument2 pagesDrug-Study ErgonPaolo UyNo ratings yet
- Bored Lang AqDocument2 pagesBored Lang AqKIANA LOUISE ROMANONo ratings yet
- LOSARTAN (ARBs) Drug Study (GERIATRICS)Document5 pagesLOSARTAN (ARBs) Drug Study (GERIATRICS)CHRISTIE MONTANONo ratings yet
- AutacoidsDocument12 pagesAutacoidsRamiz IsrafNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- NCP AnemiaDocument1 pageNCP AnemiaJennah JozelleNo ratings yet
- Effects: PharmacokineticsDocument7 pagesEffects: PharmacokineticsShiraz SiddiquiNo ratings yet
- Pals TachycardiaDocument1 pagePals TachycardiadarlingcarvajalduqueNo ratings yet
- ACLS AritmiaDocument18 pagesACLS AritmiaZega AgustianNo ratings yet
- Anti HistaminesDocument5 pagesAnti HistaminesAnkit PandeyNo ratings yet
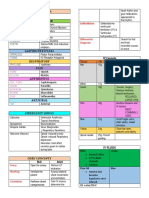
- BP Regulation Medications ChartDocument6 pagesBP Regulation Medications ChartsydNo ratings yet
- Stress Eco and Eco ReportDocument4 pagesStress Eco and Eco ReportguptarichaandassociatesNo ratings yet
- 1.inhibit Synergistic EffectDocument8 pages1.inhibit Synergistic EffectSITTIE JOBAISAH TOMINAMAN ALINo ratings yet
- HPN Drug StudyDocument4 pagesHPN Drug StudyJohn Haider Colorado GamolNo ratings yet
- DiazepamDocument4 pagesDiazepamElyhna Mara U. GonzalesNo ratings yet
- Drug StudyDocument3 pagesDrug Studychinchin ramosNo ratings yet
- Adult Asystole or PeaDocument1 pageAdult Asystole or PeamayNo ratings yet
- 14 1pm EPODocument1 page14 1pm EPOReal TetisoraNo ratings yet
- AclsDocument1 pageAclsJoice DasNo ratings yet
- Drug Study 3Document5 pagesDrug Study 3jasper pachingelNo ratings yet
- Cardiac Arrest Algorithm: Give OxygenDocument2 pagesCardiac Arrest Algorithm: Give OxygenJunius SimarmataNo ratings yet
- Adenosine: Scheduling BLS (CPR/First Aid) Acls PalsDocument4 pagesAdenosine: Scheduling BLS (CPR/First Aid) Acls PalsPhilippe Ceasar C. BascoNo ratings yet
- Oxytocin Drug StudyDocument1 pageOxytocin Drug Studysweetpixie1887% (15)
- BP Regulation Medications ChartDocument5 pagesBP Regulation Medications ChartLovely CervantesNo ratings yet
- Management of Normal Labour ChartDocument1 pageManagement of Normal Labour ChartwedishaNo ratings yet
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocument1 pageWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- Electrolyte - Water BalanceDocument5 pagesElectrolyte - Water BalancechrisibinuNo ratings yet
- Drug Study For Paracetamol, Omeprazole and Vitamin B ComplexDocument3 pagesDrug Study For Paracetamol, Omeprazole and Vitamin B ComplexMichelle Manibale R.N100% (4)
- Wa0000.Document7 pagesWa0000.benitez1228No ratings yet
- Optimizing Clinical Benefit of Anticoagulant in Acute Coronary Syndrome and Venous ThrombosisDocument46 pagesOptimizing Clinical Benefit of Anticoagulant in Acute Coronary Syndrome and Venous ThrombosisCresti Chandra PradeltaNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- Pcol 2Document9 pagesPcol 2cyk7xcdsj4No ratings yet
- Surgery PancreasDocument15 pagesSurgery PancreasAnnie HadassahNo ratings yet
- Note 2 Dec 2022Document3 pagesNote 2 Dec 2022Queen ShNo ratings yet
- Figure 4 AlgorithmACLS CACOVID 220101Document1 pageFigure 4 AlgorithmACLS CACOVID 220101AndhikaNo ratings yet
- L8. Central Nervous System (CNS) IDocument11 pagesL8. Central Nervous System (CNS) IsabahNo ratings yet
- L7. Autonomic Nervous System (ANS) IIDocument8 pagesL7. Autonomic Nervous System (ANS) IIsabahNo ratings yet
- L12. Endocrine System DrugsDocument12 pagesL12. Endocrine System DrugssabahNo ratings yet
- L11. GIT - Respiratory Tract DrugsDocument14 pagesL11. GIT - Respiratory Tract DrugssabahNo ratings yet
- B.pharmacy Time Table June 2010Document7 pagesB.pharmacy Time Table June 2010jntuforumNo ratings yet
- 1 s2.0 S0921448819302093 MainDocument9 pages1 s2.0 S0921448819302093 MainHenry Daniel Ruiz AlbaNo ratings yet
- Medical Terminlogy Body Planes SectionsDocument75 pagesMedical Terminlogy Body Planes SectionsSTEM-G.04 Kiarrah Katrina BotinNo ratings yet
- Polycythemia PaedsDocument12 pagesPolycythemia PaedscesczatNo ratings yet
- Four Abdominal Quadrants and Nine Abdominal Regions - Anatomy and PhysiologyDocument6 pagesFour Abdominal Quadrants and Nine Abdominal Regions - Anatomy and PhysiologySpoiled BratNo ratings yet
- Sodium Potassium Pump and Action PotentialDocument4 pagesSodium Potassium Pump and Action PotentialPiyush BhallaNo ratings yet
- Questions G 1Document8 pagesQuestions G 1Nader Smadi80% (5)
- Lesson 1 - The Human Body - 1.2. - Anatomical PositionsDocument5 pagesLesson 1 - The Human Body - 1.2. - Anatomical PositionsAlphine DalgoNo ratings yet
- DR Stuart Crisp DR Per Grinsted: Written byDocument8 pagesDR Stuart Crisp DR Per Grinsted: Written byRizky MarethaNo ratings yet
- EXAM BipolarDocument14 pagesEXAM BipolarTiong NeeNo ratings yet
- Electrical Hazard in BiomedicalDocument14 pagesElectrical Hazard in BiomedicalDhurai Onely100% (1)
- Fitness Program GuideDocument24 pagesFitness Program Guideandreea gheorgheNo ratings yet
- Biliary Enteric BypassDocument25 pagesBiliary Enteric BypassAlexandru Ferdohleb100% (1)
- Yatas Bedding Catalogue 1 ComDocument97 pagesYatas Bedding Catalogue 1 ComMirza Ibrar razaNo ratings yet
- The Muscular System: © 2011 The Mcgraw Hill Companies, Inc. All Rights ReservedDocument67 pagesThe Muscular System: © 2011 The Mcgraw Hill Companies, Inc. All Rights ReservedJoanna PoshnjaNo ratings yet
- Snake Anatomy and PhysiologyDocument3 pagesSnake Anatomy and Physiologybrpnaidu2157No ratings yet
- Treatment of Anxiety Disorders: Cherryrich M. Cheng, MD, DSBPPDocument43 pagesTreatment of Anxiety Disorders: Cherryrich M. Cheng, MD, DSBPPDexter FloresNo ratings yet
- Review of Evidence Suggesting That The Fascia Network Could Be The Anatomical Basis For Acupoints and Meridians in The Human BodyDocument7 pagesReview of Evidence Suggesting That The Fascia Network Could Be The Anatomical Basis For Acupoints and Meridians in The Human BodyscribalbNo ratings yet
- Circadian RhythmsDocument2 pagesCircadian RhythmsOmar Saleh100% (1)
- All Gone: A Memoir of My Mother's Dementia With Refreshments by Alex WitchelDocument4 pagesAll Gone: A Memoir of My Mother's Dementia With Refreshments by Alex WitchelSouthern California Public RadioNo ratings yet
- Neural Control and Coordination - Shobhit NirwanDocument14 pagesNeural Control and Coordination - Shobhit NirwanSWASTIKA MALONo ratings yet
- IDC 4U2 - Unit 3 Task 5 - SSDocument4 pagesIDC 4U2 - Unit 3 Task 5 - SSsavannah.e.stonehouseNo ratings yet
- Proteinas RecombinantesDocument16 pagesProteinas Recombinanteskike1790No ratings yet
- Week 2 Learning Objectives - Structure and Function of CarbohydratesDocument2 pagesWeek 2 Learning Objectives - Structure and Function of Carbohydratessteve457No ratings yet
- Anesthesiology PDFDocument40 pagesAnesthesiology PDFBiswajyoti SahuNo ratings yet
- Serology Part1Document18 pagesSerology Part1Alina Mihaela MarianNo ratings yet
- Tamil Nadu Board Class 12 BioBotany Study Material Guide in EnglishDocument55 pagesTamil Nadu Board Class 12 BioBotany Study Material Guide in Englishx a m xNo ratings yet
- Case Presentation: Riantika Nur Utami 30101407303Document40 pagesCase Presentation: Riantika Nur Utami 30101407303RiantikaNo ratings yet
- Physiology of HemoglobinDocument6 pagesPhysiology of HemoglobinAldi DenandaNo ratings yet