Download as pdf or txt
You might also like
- Emra Sportsmedicine Splint Guide PDFDocument4 pagesEmra Sportsmedicine Splint Guide PDFDhimas HartantoNo ratings yet
- Neurology LocalizationDocument6 pagesNeurology LocalizationPramod ThapaNo ratings yet
- DOH ASC LTO at Checklist Otorhinolaryngologic 1262015rev1Document3 pagesDOH ASC LTO at Checklist Otorhinolaryngologic 1262015rev1al gulNo ratings yet
- Chapter9reviewDocument7 pagesChapter9reviewkaitlyn.erik6No ratings yet
- Aime Pocket Card May 2014 3Document2 pagesAime Pocket Card May 2014 3Miguel XanaduNo ratings yet
- AnesthesiaDocument24 pagesAnesthesialittle wordsNo ratings yet
- Practical Electronics 1965 04Document84 pagesPractical Electronics 1965 04Carlos SoaresNo ratings yet
- AIRWAY MANAGEMENT (Clinical Anaesthesiology 5 Ed. by M & M)Document30 pagesAIRWAY MANAGEMENT (Clinical Anaesthesiology 5 Ed. by M & M)Kay BristolNo ratings yet
- La Faringe. SNM Del Nervio Glosofaríngeo. Plexo FaríngeoDocument24 pagesLa Faringe. SNM Del Nervio Glosofaríngeo. Plexo FaríngeocristinaNo ratings yet
- ATLSDocument29 pagesATLSmasriemarshalyNo ratings yet
- Human PhysiologyDocument35 pagesHuman Physiologyrohansewaliya9899No ratings yet
- PracticalsDocument47 pagesPracticalsmiss0101angelNo ratings yet
- Surgery & Ortho PracticalDocument52 pagesSurgery & Ortho Practicalmeadwaiet1999No ratings yet
- Img 057Document1 pageImg 057charloteinfantado3019No ratings yet
- Respiratory System HistologyDocument14 pagesRespiratory System HistologySilhouette SignNo ratings yet
- 10 Respiratory System 2Document73 pages10 Respiratory System 2Angel BumanglagNo ratings yet
- Summary of Head DR - Ihab - 3Document41 pagesSummary of Head DR - Ihab - 3ايمان عبد الشافى100% (1)
- EarthwormDocument24 pagesEarthworm10306anshkumarNo ratings yet
- Canine Radiographs: Click Skeleton To EnterDocument456 pagesCanine Radiographs: Click Skeleton To EnterAndres Luna Mendez100% (2)
- Airway AdjunctsDocument29 pagesAirway AdjunctsReza Fitra Kusuma NegaraNo ratings yet
- Pharyngeal Airways ActivityDocument7 pagesPharyngeal Airways Activitymarc gorospeNo ratings yet
- Adobe Scan 18-Jul-2023Document22 pagesAdobe Scan 18-Jul-2023AFFANNo ratings yet
- The Respiratory System: A Fixed Learning ModuleDocument38 pagesThe Respiratory System: A Fixed Learning ModulerezaNo ratings yet
- CPAP Vs NIV BiPAPDocument8 pagesCPAP Vs NIV BiPAPcharlyn206No ratings yet
- Dausvlonglade: ToungeDocument10 pagesDausvlonglade: ToungeSARYC GAMINGNo ratings yet
- Lower Limb by DR Ashwini SirDocument13 pagesLower Limb by DR Ashwini Sirvani1234guptaNo ratings yet
- Breathing and Exchange of Gases (Hand Written Notes)Document27 pagesBreathing and Exchange of Gases (Hand Written Notes)ashutoshkumar110920No ratings yet
- Nose PDFDocument6 pagesNose PDFNiranjanPandeyNo ratings yet
- Canine RadiographsDocument456 pagesCanine RadiographsThe World of Relaxing MusicNo ratings yet
- Método Canto E Delle SedieDocument196 pagesMétodo Canto E Delle SedieSsue30No ratings yet
- Ndeb ShortcutsDocument5 pagesNdeb ShortcutsParneetNo ratings yet
- AnatomyDocument26 pagesAnatomyAvinashNo ratings yet
- Blended ANFO-based ExplosivesDocument5 pagesBlended ANFO-based Explosivesalvaroaac4No ratings yet
- Cranial NervesDocument1 pageCranial NervesFluffy_iceNo ratings yet
- Trauma For FmgeDocument17 pagesTrauma For FmgeMuhammad ZeeshanNo ratings yet
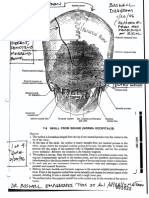
- 7-9 Skull From Behind (Norma Occipitalis)Document4 pages7-9 Skull From Behind (Norma Occipitalis)Zohaib Ur RahmanNo ratings yet
- AnesDocument18 pagesAnesEun SaekNo ratings yet
- Platinum Notes - AnaesthesiaDocument46 pagesPlatinum Notes - AnaesthesiaANMOLNo ratings yet
- Ent InstrumentsDocument26 pagesEnt Instrumentsrashidarinsha49No ratings yet
- Midterms - Medsurg LecDocument23 pagesMidterms - Medsurg LecGiel Margareth LindoNo ratings yet
- B I I o P F: Illfish Dentification in Ndian Cean Elagic IsheriesDocument12 pagesB I I o P F: Illfish Dentification in Ndian Cean Elagic Isheriesaribudi setiawanNo ratings yet
- Adobe Scan 02-Sep-2021Document16 pagesAdobe Scan 02-Sep-2021akijain20095No ratings yet
- Anatomy: StomachDocument83 pagesAnatomy: StomachIntisar AL SenaniNo ratings yet
- RSI Assessment HODocument4 pagesRSI Assessment HOlalalalalalalalalala happinessNo ratings yet
- Ana 211 Review-1Document15 pagesAna 211 Review-1LoisNo ratings yet
- Screenshot 2024-03-11 at 4.26.01 PMDocument25 pagesScreenshot 2024-03-11 at 4.26.01 PMLogic GatesNo ratings yet
- Respiratory HistologyDocument2 pagesRespiratory Histologyemptech3No ratings yet
- NotesDocument5 pagesNotesGrantNo ratings yet
- Scan Aug 14 2020Document1 pageScan Aug 14 2020api-483339757No ratings yet
- Visual Pathway LesionDocument9 pagesVisual Pathway LesionMsd KishorNo ratings yet
- St-04g Charfix Humeral-Nail Rev P-009 2022-11-24 en PassDocument58 pagesSt-04g Charfix Humeral-Nail Rev P-009 2022-11-24 en PassMetzliNo ratings yet
- Jurassic World The Park Is OpenDocument25 pagesJurassic World The Park Is OpenYasbroNo ratings yet
- Unit 4, Pharmaceutcal Inorganic Chemistry, B Pharmacy 1st Sem, Carewell PharmaDocument16 pagesUnit 4, Pharmaceutcal Inorganic Chemistry, B Pharmacy 1st Sem, Carewell Pharmayprv749kftNo ratings yet
- Infographic TitleDocument1 pageInfographic TitleScribdTranslationsNo ratings yet
- Septoplastia BeckerDocument9 pagesSeptoplastia BeckerHector UlloqueNo ratings yet
- Anatomy Lab 1Document32 pagesAnatomy Lab 1محمد جوابرهNo ratings yet
- 4250 Lec18 15Document13 pages4250 Lec18 15Carlos Enrique Pijo PerezNo ratings yet
- EMRA SportsMedicine Splint GuideDocument4 pagesEMRA SportsMedicine Splint Guidehppyduck32No ratings yet
- Special Senses TimesDocument41 pagesSpecial Senses TimesBilal MuzaffarNo ratings yet
- Pedicle Flaps in Reconstruction of The LipDocument8 pagesPedicle Flaps in Reconstruction of The LipBenedetta GuarinoNo ratings yet
- D-Day: The Air and Sea Invasion of Normandy in PhotosFrom EverandD-Day: The Air and Sea Invasion of Normandy in PhotosRating: 5 out of 5 stars5/5 (1)
- AnatomyDocument26 pagesAnatomyAvinashNo ratings yet
- Mvaiue-T:÷÷ :: PolynesiaDocument29 pagesMvaiue-T:÷÷ :: PolynesiaAvinashNo ratings yet
- 5 6111433489465213115Document39 pages5 6111433489465213115AvinashNo ratings yet
- Transfusion Medicine - RK SaranDocument80 pagesTransfusion Medicine - RK SaranAvinashNo ratings yet
- Squamous Cell Carcinoma of The Cervix With Cranial Metastasis A Case ReportDocument4 pagesSquamous Cell Carcinoma of The Cervix With Cranial Metastasis A Case ReportJonelle baloloyNo ratings yet
- 1516 4446 RBP 1516444620200013Document3 pages1516 4446 RBP 1516444620200013Luisa RamirezNo ratings yet
- Magnetic Resonance Imaging: Anjali Wadhwa, Anuj Bhardwaj, Vivek Singh Verma TDocument13 pagesMagnetic Resonance Imaging: Anjali Wadhwa, Anuj Bhardwaj, Vivek Singh Verma T20D221 - LAKSHMI PRIYA ANo ratings yet
- Test Bank For Radiographic Pathology For Technologists 7th Edition by KowalczykDocument8 pagesTest Bank For Radiographic Pathology For Technologists 7th Edition by KowalczykAudrey Snook100% (35)
- Prevention of Ureteral Injuries in Gynecologic SurgeryDocument5 pagesPrevention of Ureteral Injuries in Gynecologic Surgery黃靖貽No ratings yet
- Ch01 Anatomy BasicsDocument1 pageCh01 Anatomy BasicsrenjiniNo ratings yet
- Lymphatic Drainage of Head and NeckDocument60 pagesLymphatic Drainage of Head and NeckKhadija VasiNo ratings yet
- Grade 12 NotesDocument5 pagesGrade 12 Noteshafsag307No ratings yet
- Botulinum Toxin in CancerDocument11 pagesBotulinum Toxin in CancerAlicia Ramirez HernandezNo ratings yet
- 2.7 Cell Division Going Wrong - Cancer PDFDocument8 pages2.7 Cell Division Going Wrong - Cancer PDFAntoline Natasha RayappanNo ratings yet
- SNC2D1 Biology Unit ReviewDocument3 pagesSNC2D1 Biology Unit ReviewSA - 10WB 933839 The Woodlands SSNo ratings yet
- Acquired Infantile Horner Syndrome and Spontaneous Internal Carotid Artery Dissection: A Case Report and Review of LiteratureDocument10 pagesAcquired Infantile Horner Syndrome and Spontaneous Internal Carotid Artery Dissection: A Case Report and Review of LiteratureDanielle SangalangNo ratings yet
- Differential Diagnosis: Hallows Around LightDocument10 pagesDifferential Diagnosis: Hallows Around LightfeedodeedoNo ratings yet
- Holmes - Clinical Neurophysiology of Infancy Childhood and AdolescenceDocument856 pagesHolmes - Clinical Neurophysiology of Infancy Childhood and AdolescenceMarysol UlloaNo ratings yet
- Third Nerve Palsy Analysis of 1400 Personally Examined InpatientsDocument9 pagesThird Nerve Palsy Analysis of 1400 Personally Examined Inpatientstenthousand hoursNo ratings yet
- PD22 Hap1 L03Document33 pagesPD22 Hap1 L03Ka Yan LAUNo ratings yet
- FNA CCX Ovojnice, CSF, KŽ Za Miru 2020 - gs15FDocument194 pagesFNA CCX Ovojnice, CSF, KŽ Za Miru 2020 - gs15FGoran SimicNo ratings yet
- NYSORA Hazdics RegionalDocument8 pagesNYSORA Hazdics RegionalAishu BNo ratings yet
- Production of SpeechDocument12 pagesProduction of Speechaika.kadyralievaNo ratings yet
- Crohn DiseaseDocument18 pagesCrohn Diseasecharlester0927No ratings yet
- Cranial Nerves in Health and Disease (2nd Edition) - (XI. Accessory Nerve)Document11 pagesCranial Nerves in Health and Disease (2nd Edition) - (XI. Accessory Nerve)Pierre PradelNo ratings yet
- Approach To A Patient With JaundiceDocument33 pagesApproach To A Patient With JaundiceManish AdhikariNo ratings yet
- Digestive and Endocrine System: 5141 CN 111 - Anatomy and PhysiologyDocument4 pagesDigestive and Endocrine System: 5141 CN 111 - Anatomy and PhysiologyAlthea Joyce OngNo ratings yet
- General Surgery - 1st Term McqsDocument4 pagesGeneral Surgery - 1st Term Mcqswajeehafatima432No ratings yet
- The Biology of Mind: Powerpoint® PresentationDocument56 pagesThe Biology of Mind: Powerpoint® PresentationJessa PacamparaNo ratings yet
- Horner Syndrome: A Clinical Review: Timothy J. MartinDocument10 pagesHorner Syndrome: A Clinical Review: Timothy J. Martinpresentator dadakanNo ratings yet
- Aquaporin 4 Is Differentially Increased and Depolarized in Association With Tau and Amyloid-BetaDocument33 pagesAquaporin 4 Is Differentially Increased and Depolarized in Association With Tau and Amyloid-BetaAndrade GuiNo ratings yet
- Physical and Healthy ImpairmentsDocument27 pagesPhysical and Healthy ImpairmentsMwanalushi KanjalaNo ratings yet
- Understanding Anatomy PhysiologyDocument72 pagesUnderstanding Anatomy PhysiologyPipe Marhín100% (1)