
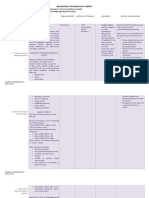
Exercise Considerations For Type 1 and Type 2.6
Exercise Considerations For Type 1 and Type 2.6
You might also like
- Int&Fun&Med&Nut&the&1 STDocument1,088 pagesInt&Fun&Med&Nut&the&1 STагата кристи100% (18)
- 7 Stars Doctors Required by WHO and FKUIDocument2 pages7 Stars Doctors Required by WHO and FKUIWidya Ayu92% (12)
- The Disease Delusion: Conquering the Causes of Chronic Illness for a Healthier, Longer, and Happier LifeFrom EverandThe Disease Delusion: Conquering the Causes of Chronic Illness for a Healthier, Longer, and Happier LifeRating: 4 out of 5 stars4/5 (11)
- Principles of RAW TrainingDocument51 pagesPrinciples of RAW TrainingAnthony DinicolantonioNo ratings yet
- Do Not Request Access To Make Your Own Copy: File Download Choose Desired FormatDocument7 pagesDo Not Request Access To Make Your Own Copy: File Download Choose Desired FormatAlex PhoNo ratings yet
- Atkinson 2014Document14 pagesAtkinson 2014nagitagtgtNo ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument16 pagesType 2 Diabetes: Annals of Internal Medicineallele94No ratings yet
- Exercise Is MedicineDocument13 pagesExercise Is MedicineFelipe Andrés Castellón Araya100% (1)
- Capstone Stem12 Group6Document32 pagesCapstone Stem12 Group6Rianne GasgoniaNo ratings yet
- Fifteen-Minute Consultation: Diabulimia and Disordered Eating in Childhood DiabetesDocument7 pagesFifteen-Minute Consultation: Diabulimia and Disordered Eating in Childhood DiabetesZara LauraNo ratings yet
- 1 Diabetes Mellitus: Practice GapsDocument15 pages1 Diabetes Mellitus: Practice Gapssari whardanie mahligai patteryNo ratings yet
- DM Tipo1Document15 pagesDM Tipo1SixtoIñaguazoNo ratings yet
- Diabetes Review LiteratureDocument72 pagesDiabetes Review LiteratureAntonio Zandre Moreira LopesNo ratings yet
- Insulin Therapy in Type 2 Diabetes Mellitus: A Practical Approach For Primary Care Physicians and Other Health Care ProfessionalsDocument12 pagesInsulin Therapy in Type 2 Diabetes Mellitus: A Practical Approach For Primary Care Physicians and Other Health Care ProfessionalsdaddaNo ratings yet
- Gregory Pir 2013Document16 pagesGregory Pir 2013Karina CamachoNo ratings yet
- Diabetes and Drug TreatmentsDocument5 pagesDiabetes and Drug TreatmentsPawel kNo ratings yet
- Literature Review On Diabetes PDFDocument4 pagesLiterature Review On Diabetes PDFklbndecnd100% (1)
- Medical Management of Acute Severe Anorexia Nervosa: Amy Norrington, Ruth Stanley, Michael Tremlett, Ginny BirrellDocument7 pagesMedical Management of Acute Severe Anorexia Nervosa: Amy Norrington, Ruth Stanley, Michael Tremlett, Ginny BirrellMarioNo ratings yet
- Tutorial 7 Health - and - Disease SEM I 2017-18Document3 pagesTutorial 7 Health - and - Disease SEM I 2017-18Denisha PhillipsNo ratings yet
- The Hidden Burden of Diabetes Mellitus in An Urban Community 60743Document9 pagesThe Hidden Burden of Diabetes Mellitus in An Urban Community 60743Solomon BerhanuNo ratings yet
- Dmso 223123 Diabetes Self Management Education Dsme Ndash Effect OnDocument11 pagesDmso 223123 Diabetes Self Management Education Dsme Ndash Effect OnQoryNo ratings yet
- Prescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsDocument10 pagesPrescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsEnzo VasquezNo ratings yet
- What Is Diabulimia and What Are The Implications For Practice?Document5 pagesWhat Is Diabulimia and What Are The Implications For Practice?Ana Raíza OliveiraNo ratings yet
- Nejm AnorexiaDocument9 pagesNejm AnorexiaRodrigo EstebanNo ratings yet
- 2006 HOUGHTONCJCM56 Insulin ResistanceDocument11 pages2006 HOUGHTONCJCM56 Insulin Resistancecikgu raineeNo ratings yet
- Rethinking Diabetes: Entanglements with Trauma, Poverty, and HIVFrom EverandRethinking Diabetes: Entanglements with Trauma, Poverty, and HIVNo ratings yet
- Ingredients Clinical Review 2017Document7 pagesIngredients Clinical Review 2017fahri azwarNo ratings yet
- Development and Validation of Five UV Spectrophotometric Methods For Simultaneous Estimation of Ramipril and Amlodipine Besylate in CapsulesDocument10 pagesDevelopment and Validation of Five UV Spectrophotometric Methods For Simultaneous Estimation of Ramipril and Amlodipine Besylate in CapsulesIJPS : A Pharmaceutical JournalNo ratings yet
- 1.1 GeneralDocument23 pages1.1 GeneralpriyankaNo ratings yet
- Anorexia NervosaDocument9 pagesAnorexia NervosaDouglas SantosNo ratings yet
- Good Paper KAP Cut Off Two LevelsDocument18 pagesGood Paper KAP Cut Off Two LevelsSiti Hadijah Aspan, M.PHNo ratings yet
- DCP69 PDFDocument12 pagesDCP69 PDFANDRES DAVID GUEVARA MENDOZANo ratings yet
- Promoting Effective Disease ManagementDocument12 pagesPromoting Effective Disease ManagementAndika SulistiawanNo ratings yet
- Unit 3 DiscussionDocument6 pagesUnit 3 DiscussionFrank PereiraNo ratings yet
- ECDMR-05-00136 Diabetes and The Power of Speech Dec 30 2020Document5 pagesECDMR-05-00136 Diabetes and The Power of Speech Dec 30 2020Fabiola Prado de NitschNo ratings yet
- Nutrients Micro and Macro Nutrients: Importance of Good NutritionDocument9 pagesNutrients Micro and Macro Nutrients: Importance of Good NutritionFRANCIS FRANCISCO. CLIMACONo ratings yet
- Diabetes Mellitus Tipo 1 LancetDocument14 pagesDiabetes Mellitus Tipo 1 LancetLina RojasNo ratings yet
- Comparing The Effect of AcupreDocument11 pagesComparing The Effect of AcupreNespitaNo ratings yet
- Pengobatan TradisionalDocument13 pagesPengobatan TradisionalDiazQurrataa DNo ratings yet
- Diabetes and Mental HealthDocument3 pagesDiabetes and Mental HealthVENNA FADILLAHNo ratings yet
- Neuropatia DiabéticaDocument18 pagesNeuropatia DiabéticaGustavo PestanaNo ratings yet
- Reproductive Impact of Eating Disorders 22Document8 pagesReproductive Impact of Eating Disorders 22adriancnlogronoNo ratings yet
- Developing A Teaching PlanDocument6 pagesDeveloping A Teaching PlanAntonette Africa MercadoNo ratings yet
- Depression and Diabetes Revised 2021Document30 pagesDepression and Diabetes Revised 2021SenaNo ratings yet
- School Board Attorney ArticleDocument8 pagesSchool Board Attorney Articlemahersvt2504No ratings yet
- Nutrition - LN 1Document9 pagesNutrition - LN 1Elena Maestre GriñanNo ratings yet
- Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFDocument15 pagesDifferentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFHadi PrasetyoNo ratings yet
- J Ajem 2019 07 013Document1 pageJ Ajem 2019 07 013daeron42No ratings yet
- Book Reviews: Fat Politics. The Real Story Behind America's Obesity EpidemicDocument2 pagesBook Reviews: Fat Politics. The Real Story Behind America's Obesity EpidemicafshanNo ratings yet
- Eating Disorders in Diabetes PDFDocument3 pagesEating Disorders in Diabetes PDFJúlia PriyaNo ratings yet
- Natural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusDocument21 pagesNatural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusparibashaiNo ratings yet
- Burton 2020Document9 pagesBurton 2020BelennQM ChupipandiNo ratings yet
- ITC Type 2 Diabetes 2019Document16 pagesITC Type 2 Diabetes 2019ALEJANDRO DUEÑAS GUTIERREZNo ratings yet
- Scollan 2011 TheoryDocument12 pagesScollan 2011 TheoryYuya PlimNo ratings yet
- Youth-Onset Type 2 Diabetes Consensus Report: Current Status, Challenges, and PrioritiesDocument8 pagesYouth-Onset Type 2 Diabetes Consensus Report: Current Status, Challenges, and PrioritiesHasan MahmoodNo ratings yet
- Reduction in The Incidence of Type 2 Diabetes With Lifestyle Intervention or MetforminDocument11 pagesReduction in The Incidence of Type 2 Diabetes With Lifestyle Intervention or MetformincontasecundarialuzNo ratings yet
- Myths and Misconceptions About Insulin Therapy Among Latinos Hispanics With Diabetes A Fresh Look at An Old Problem 2155 6156.1000482Document5 pagesMyths and Misconceptions About Insulin Therapy Among Latinos Hispanics With Diabetes A Fresh Look at An Old Problem 2155 6156.1000482Rosa RuizNo ratings yet
- Type 2 Diabetes Mellitus in Children and Adolescents: A Relatively New Clinical Problem Within Pediatric PracticeDocument5 pagesType 2 Diabetes Mellitus in Children and Adolescents: A Relatively New Clinical Problem Within Pediatric PracticeAnnisa FujiantiNo ratings yet
- Type 1 Diabetes Mellitus in Pediatric Patients and Its Impact On Relationships in The Family Enviroment - 2020Document8 pagesType 1 Diabetes Mellitus in Pediatric Patients and Its Impact On Relationships in The Family Enviroment - 2020Nisa FjrNo ratings yet
- Cap 1Document11 pagesCap 1SofiaNo ratings yet
- PTJ 1254Document11 pagesPTJ 1254angsokasatuNo ratings yet
- A Short History of The Metabolic Syndrome DefinitionsDocument8 pagesA Short History of The Metabolic Syndrome DefinitionsexraNo ratings yet
- Kinetic Sources of Lower Limb Angular Displacement.11Document7 pagesKinetic Sources of Lower Limb Angular Displacement.11Rivaldo RobinsonNo ratings yet
- Brukner and Khan S Clinical Sports Medicine Volume.30Document1 pageBrukner and Khan S Clinical Sports Medicine Volume.30Rivaldo RobinsonNo ratings yet
- Work Experience Placement Application Form v1.16Document4 pagesWork Experience Placement Application Form v1.16Rivaldo RobinsonNo ratings yet
- CW Portfolio 20 21 Template-1Document6 pagesCW Portfolio 20 21 Template-1Rivaldo RobinsonNo ratings yet
- Exercise As MedicineDocument1 pageExercise As MedicineRivaldo RobinsonNo ratings yet
- CorrespondenceDocument4 pagesCorrespondenceRivaldo RobinsonNo ratings yet
- Yoga ProjectDocument15 pagesYoga Projectmanikandan100% (3)
- Does A Calisthenics-Based Exercise Program Applied in School Improve Morphofunctional Parameters in Youth?Document11 pagesDoes A Calisthenics-Based Exercise Program Applied in School Improve Morphofunctional Parameters in Youth?Jendra WansaNo ratings yet
- The Importance of WorkoutDocument8 pagesThe Importance of WorkoutTazo BodaveliNo ratings yet
- HS Committee 64th Session - Amendments To HS Explanatory NotesDocument5 pagesHS Committee 64th Session - Amendments To HS Explanatory NotesChiNo ratings yet
- ALL ExcercisesDocument28 pagesALL ExcercisesJames ScoldNo ratings yet
- Revised Physical Fitness TestDocument2 pagesRevised Physical Fitness TestCARLYN SILVANo ratings yet
- Training-Intensity Distribution On Middle - and Long-Distance Runners A Systematic ReviewDocument27 pagesTraining-Intensity Distribution On Middle - and Long-Distance Runners A Systematic ReviewArmando NetoNo ratings yet
- 30-Article Text-75-1-10-20220520Document13 pages30-Article Text-75-1-10-20220520dija.yedijaNo ratings yet
- P.E. ReportDocument17 pagesP.E. ReportMairah PendalidayNo ratings yet
- Group 4: Global Recommendation On Physical ActivityDocument50 pagesGroup 4: Global Recommendation On Physical ActivityMYLE MANAYONNo ratings yet
- Activity Log #4: Surrey Connect Physical Education 10Document7 pagesActivity Log #4: Surrey Connect Physical Education 10Rami MustafaNo ratings yet
- Nutrition Care Plan - Febrile Client With Hepatitis ADocument3 pagesNutrition Care Plan - Febrile Client With Hepatitis AElaine ArsagaNo ratings yet
- Millennial Preferences Toward Treating Minor DiseasesDocument47 pagesMillennial Preferences Toward Treating Minor DiseasesMa Angelica Edison SesucaNo ratings yet
- Train, Brain - The Ultimate Guide To Cross Fit (2021) - Libgen - LiDocument112 pagesTrain, Brain - The Ultimate Guide To Cross Fit (2021) - Libgen - LiDayvison Santos Ifbb100% (2)
- CTRL's 10 Week ProgramDocument23 pagesCTRL's 10 Week Programpéter bathóNo ratings yet
- Hattie Ebook Final - CompressedDocument31 pagesHattie Ebook Final - CompressedJasmyn SabbahNo ratings yet
- Strategic Management Phase 2 Group212053 9Document12 pagesStrategic Management Phase 2 Group212053 9stefanyNo ratings yet
- Elc501 - Group Portfolio ForumDocument11 pagesElc501 - Group Portfolio ForumAhmad SyamiNo ratings yet
- 2018 ADA Standards of CareDocument150 pages2018 ADA Standards of CareAnonymous AvknB0cW7tNo ratings yet
- GERIATRICS 2nd Sem Midterms Combined NotesDocument23 pagesGERIATRICS 2nd Sem Midterms Combined NotesMeryville Jacildo100% (1)
- Activity Sheet No 1 PeDocument3 pagesActivity Sheet No 1 Peamy grant castilloNo ratings yet
- Career Machinations in FoodDocument31 pagesCareer Machinations in FoodShalini SehgalNo ratings yet
- Aibt Chcprp003 Learner Workbook Ecec v1.0Document58 pagesAibt Chcprp003 Learner Workbook Ecec v1.0ks khalsaNo ratings yet
- OT Practice FrameworkDocument12 pagesOT Practice Frameworkenrico_aguila100% (2)
- Activity Tracking and Calories Burn - Lab AssignmentDocument14 pagesActivity Tracking and Calories Burn - Lab AssignmentStephanie PonceNo ratings yet
- Slide Presentationthe Study of Knowledge and Attitudes About Covid 19 Among Patients in Hospital KudatDocument44 pagesSlide Presentationthe Study of Knowledge and Attitudes About Covid 19 Among Patients in Hospital KudatBlue Eyed SoulNo ratings yet
- A Year of Self-Care Daily Practices and Inspiration For Caring For Yourself (Zoe Shaw)Document184 pagesA Year of Self-Care Daily Practices and Inspiration For Caring For Yourself (Zoe Shaw)Yvette Magat100% (1)






























































































Download as pdf or txt
You might also like
- Int&Fun&Med&Nut&the&1 STDocument1,088 pagesInt&Fun&Med&Nut&the&1 STагата кристи100% (18)
- 7 Stars Doctors Required by WHO and FKUIDocument2 pages7 Stars Doctors Required by WHO and FKUIWidya Ayu92% (12)
- The Disease Delusion: Conquering the Causes of Chronic Illness for a Healthier, Longer, and Happier LifeFrom EverandThe Disease Delusion: Conquering the Causes of Chronic Illness for a Healthier, Longer, and Happier LifeRating: 4 out of 5 stars4/5 (11)
- Principles of RAW TrainingDocument51 pagesPrinciples of RAW TrainingAnthony DinicolantonioNo ratings yet
- Do Not Request Access To Make Your Own Copy: File Download Choose Desired FormatDocument7 pagesDo Not Request Access To Make Your Own Copy: File Download Choose Desired FormatAlex PhoNo ratings yet
- Atkinson 2014Document14 pagesAtkinson 2014nagitagtgtNo ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument16 pagesType 2 Diabetes: Annals of Internal Medicineallele94No ratings yet
- Exercise Is MedicineDocument13 pagesExercise Is MedicineFelipe Andrés Castellón Araya100% (1)
- Capstone Stem12 Group6Document32 pagesCapstone Stem12 Group6Rianne GasgoniaNo ratings yet
- Fifteen-Minute Consultation: Diabulimia and Disordered Eating in Childhood DiabetesDocument7 pagesFifteen-Minute Consultation: Diabulimia and Disordered Eating in Childhood DiabetesZara LauraNo ratings yet
- 1 Diabetes Mellitus: Practice GapsDocument15 pages1 Diabetes Mellitus: Practice Gapssari whardanie mahligai patteryNo ratings yet
- DM Tipo1Document15 pagesDM Tipo1SixtoIñaguazoNo ratings yet
- Diabetes Review LiteratureDocument72 pagesDiabetes Review LiteratureAntonio Zandre Moreira LopesNo ratings yet
- Insulin Therapy in Type 2 Diabetes Mellitus: A Practical Approach For Primary Care Physicians and Other Health Care ProfessionalsDocument12 pagesInsulin Therapy in Type 2 Diabetes Mellitus: A Practical Approach For Primary Care Physicians and Other Health Care ProfessionalsdaddaNo ratings yet
- Gregory Pir 2013Document16 pagesGregory Pir 2013Karina CamachoNo ratings yet
- Diabetes and Drug TreatmentsDocument5 pagesDiabetes and Drug TreatmentsPawel kNo ratings yet
- Literature Review On Diabetes PDFDocument4 pagesLiterature Review On Diabetes PDFklbndecnd100% (1)
- Medical Management of Acute Severe Anorexia Nervosa: Amy Norrington, Ruth Stanley, Michael Tremlett, Ginny BirrellDocument7 pagesMedical Management of Acute Severe Anorexia Nervosa: Amy Norrington, Ruth Stanley, Michael Tremlett, Ginny BirrellMarioNo ratings yet
- Tutorial 7 Health - and - Disease SEM I 2017-18Document3 pagesTutorial 7 Health - and - Disease SEM I 2017-18Denisha PhillipsNo ratings yet
- The Hidden Burden of Diabetes Mellitus in An Urban Community 60743Document9 pagesThe Hidden Burden of Diabetes Mellitus in An Urban Community 60743Solomon BerhanuNo ratings yet
- Dmso 223123 Diabetes Self Management Education Dsme Ndash Effect OnDocument11 pagesDmso 223123 Diabetes Self Management Education Dsme Ndash Effect OnQoryNo ratings yet
- Prescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsDocument10 pagesPrescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsEnzo VasquezNo ratings yet
- What Is Diabulimia and What Are The Implications For Practice?Document5 pagesWhat Is Diabulimia and What Are The Implications For Practice?Ana Raíza OliveiraNo ratings yet
- Nejm AnorexiaDocument9 pagesNejm AnorexiaRodrigo EstebanNo ratings yet
- 2006 HOUGHTONCJCM56 Insulin ResistanceDocument11 pages2006 HOUGHTONCJCM56 Insulin Resistancecikgu raineeNo ratings yet
- Rethinking Diabetes: Entanglements with Trauma, Poverty, and HIVFrom EverandRethinking Diabetes: Entanglements with Trauma, Poverty, and HIVNo ratings yet
- Ingredients Clinical Review 2017Document7 pagesIngredients Clinical Review 2017fahri azwarNo ratings yet
- Development and Validation of Five UV Spectrophotometric Methods For Simultaneous Estimation of Ramipril and Amlodipine Besylate in CapsulesDocument10 pagesDevelopment and Validation of Five UV Spectrophotometric Methods For Simultaneous Estimation of Ramipril and Amlodipine Besylate in CapsulesIJPS : A Pharmaceutical JournalNo ratings yet
- 1.1 GeneralDocument23 pages1.1 GeneralpriyankaNo ratings yet
- Anorexia NervosaDocument9 pagesAnorexia NervosaDouglas SantosNo ratings yet
- Good Paper KAP Cut Off Two LevelsDocument18 pagesGood Paper KAP Cut Off Two LevelsSiti Hadijah Aspan, M.PHNo ratings yet
- DCP69 PDFDocument12 pagesDCP69 PDFANDRES DAVID GUEVARA MENDOZANo ratings yet
- Promoting Effective Disease ManagementDocument12 pagesPromoting Effective Disease ManagementAndika SulistiawanNo ratings yet
- Unit 3 DiscussionDocument6 pagesUnit 3 DiscussionFrank PereiraNo ratings yet
- ECDMR-05-00136 Diabetes and The Power of Speech Dec 30 2020Document5 pagesECDMR-05-00136 Diabetes and The Power of Speech Dec 30 2020Fabiola Prado de NitschNo ratings yet
- Nutrients Micro and Macro Nutrients: Importance of Good NutritionDocument9 pagesNutrients Micro and Macro Nutrients: Importance of Good NutritionFRANCIS FRANCISCO. CLIMACONo ratings yet
- Diabetes Mellitus Tipo 1 LancetDocument14 pagesDiabetes Mellitus Tipo 1 LancetLina RojasNo ratings yet
- Comparing The Effect of AcupreDocument11 pagesComparing The Effect of AcupreNespitaNo ratings yet
- Pengobatan TradisionalDocument13 pagesPengobatan TradisionalDiazQurrataa DNo ratings yet
- Diabetes and Mental HealthDocument3 pagesDiabetes and Mental HealthVENNA FADILLAHNo ratings yet
- Neuropatia DiabéticaDocument18 pagesNeuropatia DiabéticaGustavo PestanaNo ratings yet
- Reproductive Impact of Eating Disorders 22Document8 pagesReproductive Impact of Eating Disorders 22adriancnlogronoNo ratings yet
- Developing A Teaching PlanDocument6 pagesDeveloping A Teaching PlanAntonette Africa MercadoNo ratings yet
- Depression and Diabetes Revised 2021Document30 pagesDepression and Diabetes Revised 2021SenaNo ratings yet
- School Board Attorney ArticleDocument8 pagesSchool Board Attorney Articlemahersvt2504No ratings yet
- Nutrition - LN 1Document9 pagesNutrition - LN 1Elena Maestre GriñanNo ratings yet
- Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFDocument15 pagesDifferentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFHadi PrasetyoNo ratings yet
- J Ajem 2019 07 013Document1 pageJ Ajem 2019 07 013daeron42No ratings yet
- Book Reviews: Fat Politics. The Real Story Behind America's Obesity EpidemicDocument2 pagesBook Reviews: Fat Politics. The Real Story Behind America's Obesity EpidemicafshanNo ratings yet
- Eating Disorders in Diabetes PDFDocument3 pagesEating Disorders in Diabetes PDFJúlia PriyaNo ratings yet
- Natural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusDocument21 pagesNatural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusparibashaiNo ratings yet
- Burton 2020Document9 pagesBurton 2020BelennQM ChupipandiNo ratings yet
- ITC Type 2 Diabetes 2019Document16 pagesITC Type 2 Diabetes 2019ALEJANDRO DUEÑAS GUTIERREZNo ratings yet
- Scollan 2011 TheoryDocument12 pagesScollan 2011 TheoryYuya PlimNo ratings yet
- Youth-Onset Type 2 Diabetes Consensus Report: Current Status, Challenges, and PrioritiesDocument8 pagesYouth-Onset Type 2 Diabetes Consensus Report: Current Status, Challenges, and PrioritiesHasan MahmoodNo ratings yet
- Reduction in The Incidence of Type 2 Diabetes With Lifestyle Intervention or MetforminDocument11 pagesReduction in The Incidence of Type 2 Diabetes With Lifestyle Intervention or MetformincontasecundarialuzNo ratings yet
- Myths and Misconceptions About Insulin Therapy Among Latinos Hispanics With Diabetes A Fresh Look at An Old Problem 2155 6156.1000482Document5 pagesMyths and Misconceptions About Insulin Therapy Among Latinos Hispanics With Diabetes A Fresh Look at An Old Problem 2155 6156.1000482Rosa RuizNo ratings yet
- Type 2 Diabetes Mellitus in Children and Adolescents: A Relatively New Clinical Problem Within Pediatric PracticeDocument5 pagesType 2 Diabetes Mellitus in Children and Adolescents: A Relatively New Clinical Problem Within Pediatric PracticeAnnisa FujiantiNo ratings yet
- Type 1 Diabetes Mellitus in Pediatric Patients and Its Impact On Relationships in The Family Enviroment - 2020Document8 pagesType 1 Diabetes Mellitus in Pediatric Patients and Its Impact On Relationships in The Family Enviroment - 2020Nisa FjrNo ratings yet
- Cap 1Document11 pagesCap 1SofiaNo ratings yet
- PTJ 1254Document11 pagesPTJ 1254angsokasatuNo ratings yet
- A Short History of The Metabolic Syndrome DefinitionsDocument8 pagesA Short History of The Metabolic Syndrome DefinitionsexraNo ratings yet
- Kinetic Sources of Lower Limb Angular Displacement.11Document7 pagesKinetic Sources of Lower Limb Angular Displacement.11Rivaldo RobinsonNo ratings yet
- Brukner and Khan S Clinical Sports Medicine Volume.30Document1 pageBrukner and Khan S Clinical Sports Medicine Volume.30Rivaldo RobinsonNo ratings yet
- Work Experience Placement Application Form v1.16Document4 pagesWork Experience Placement Application Form v1.16Rivaldo RobinsonNo ratings yet
- CW Portfolio 20 21 Template-1Document6 pagesCW Portfolio 20 21 Template-1Rivaldo RobinsonNo ratings yet
- Exercise As MedicineDocument1 pageExercise As MedicineRivaldo RobinsonNo ratings yet
- CorrespondenceDocument4 pagesCorrespondenceRivaldo RobinsonNo ratings yet
- Yoga ProjectDocument15 pagesYoga Projectmanikandan100% (3)
- Does A Calisthenics-Based Exercise Program Applied in School Improve Morphofunctional Parameters in Youth?Document11 pagesDoes A Calisthenics-Based Exercise Program Applied in School Improve Morphofunctional Parameters in Youth?Jendra WansaNo ratings yet
- The Importance of WorkoutDocument8 pagesThe Importance of WorkoutTazo BodaveliNo ratings yet
- HS Committee 64th Session - Amendments To HS Explanatory NotesDocument5 pagesHS Committee 64th Session - Amendments To HS Explanatory NotesChiNo ratings yet
- ALL ExcercisesDocument28 pagesALL ExcercisesJames ScoldNo ratings yet
- Revised Physical Fitness TestDocument2 pagesRevised Physical Fitness TestCARLYN SILVANo ratings yet
- Training-Intensity Distribution On Middle - and Long-Distance Runners A Systematic ReviewDocument27 pagesTraining-Intensity Distribution On Middle - and Long-Distance Runners A Systematic ReviewArmando NetoNo ratings yet
- 30-Article Text-75-1-10-20220520Document13 pages30-Article Text-75-1-10-20220520dija.yedijaNo ratings yet
- P.E. ReportDocument17 pagesP.E. ReportMairah PendalidayNo ratings yet
- Group 4: Global Recommendation On Physical ActivityDocument50 pagesGroup 4: Global Recommendation On Physical ActivityMYLE MANAYONNo ratings yet
- Activity Log #4: Surrey Connect Physical Education 10Document7 pagesActivity Log #4: Surrey Connect Physical Education 10Rami MustafaNo ratings yet
- Nutrition Care Plan - Febrile Client With Hepatitis ADocument3 pagesNutrition Care Plan - Febrile Client With Hepatitis AElaine ArsagaNo ratings yet
- Millennial Preferences Toward Treating Minor DiseasesDocument47 pagesMillennial Preferences Toward Treating Minor DiseasesMa Angelica Edison SesucaNo ratings yet
- Train, Brain - The Ultimate Guide To Cross Fit (2021) - Libgen - LiDocument112 pagesTrain, Brain - The Ultimate Guide To Cross Fit (2021) - Libgen - LiDayvison Santos Ifbb100% (2)
- CTRL's 10 Week ProgramDocument23 pagesCTRL's 10 Week Programpéter bathóNo ratings yet
- Hattie Ebook Final - CompressedDocument31 pagesHattie Ebook Final - CompressedJasmyn SabbahNo ratings yet
- Strategic Management Phase 2 Group212053 9Document12 pagesStrategic Management Phase 2 Group212053 9stefanyNo ratings yet
- Elc501 - Group Portfolio ForumDocument11 pagesElc501 - Group Portfolio ForumAhmad SyamiNo ratings yet
- 2018 ADA Standards of CareDocument150 pages2018 ADA Standards of CareAnonymous AvknB0cW7tNo ratings yet
- GERIATRICS 2nd Sem Midterms Combined NotesDocument23 pagesGERIATRICS 2nd Sem Midterms Combined NotesMeryville Jacildo100% (1)
- Activity Sheet No 1 PeDocument3 pagesActivity Sheet No 1 Peamy grant castilloNo ratings yet
- Career Machinations in FoodDocument31 pagesCareer Machinations in FoodShalini SehgalNo ratings yet
- Aibt Chcprp003 Learner Workbook Ecec v1.0Document58 pagesAibt Chcprp003 Learner Workbook Ecec v1.0ks khalsaNo ratings yet
- OT Practice FrameworkDocument12 pagesOT Practice Frameworkenrico_aguila100% (2)
- Activity Tracking and Calories Burn - Lab AssignmentDocument14 pagesActivity Tracking and Calories Burn - Lab AssignmentStephanie PonceNo ratings yet
- Slide Presentationthe Study of Knowledge and Attitudes About Covid 19 Among Patients in Hospital KudatDocument44 pagesSlide Presentationthe Study of Knowledge and Attitudes About Covid 19 Among Patients in Hospital KudatBlue Eyed SoulNo ratings yet
- A Year of Self-Care Daily Practices and Inspiration For Caring For Yourself (Zoe Shaw)Document184 pagesA Year of Self-Care Daily Practices and Inspiration For Caring For Yourself (Zoe Shaw)Yvette Magat100% (1)