Download as pdf or txt
You might also like
- Stroke Topic DiscussionDocument19 pagesStroke Topic Discussionapi-648714317No ratings yet
- Brosur Suction Pro 72Document4 pagesBrosur Suction Pro 72Anonymous tbJ24554No ratings yet
- (Oxy) Med-Surg Checklist With RationaleDocument13 pages(Oxy) Med-Surg Checklist With RationaleUri Perez MontedeRamos100% (1)
- Is This The Man Behind The Global Coronavirus PandemicDocument6 pagesIs This The Man Behind The Global Coronavirus PandemicMonte CarloNo ratings yet
- Acute Coronary Syndrome - YMDocument64 pagesAcute Coronary Syndrome - YMNirwanaNo ratings yet
- ACS Management in Pandemic EraDocument56 pagesACS Management in Pandemic EraFatmawati nersNo ratings yet
- An Update Management of Acute Ischemic Stroke: SurotoDocument36 pagesAn Update Management of Acute Ischemic Stroke: SurotoShinta DianNo ratings yet
- How To Stratify The Risk and When To Refer: NsteacsDocument28 pagesHow To Stratify The Risk and When To Refer: NsteacsRatna TambaNo ratings yet
- Esc Acs GuidelinesDocument62 pagesEsc Acs GuidelineszakiyaNo ratings yet
- Transient Ischemic AttackDocument23 pagesTransient Ischemic AttackAnonymous 9xHTwHYNo ratings yet
- Acute Heart Failure in Acute Coronary Syndrome: Buying Time To RevascularizationDocument43 pagesAcute Heart Failure in Acute Coronary Syndrome: Buying Time To RevascularizationMunasir BahriNo ratings yet
- ACS-Karim AbdellatifDocument10 pagesACS-Karim AbdellatifKarim AbdellatifNo ratings yet
- WECOC - Management of NSTEMI and Invasive StrategyDocument42 pagesWECOC - Management of NSTEMI and Invasive StrategyAdiyanto DidietNo ratings yet
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095No ratings yet
- ACC/AHA 2009 STEMI Guideline Focused Update and What's New in 2012 GuidelineDocument44 pagesACC/AHA 2009 STEMI Guideline Focused Update and What's New in 2012 GuidelineArry Andres MissiNo ratings yet
- Transient Ischemic Attack and Minor Stroke: Diagnosis, Risk Stratification and ManagementDocument6 pagesTransient Ischemic Attack and Minor Stroke: Diagnosis, Risk Stratification and ManagementAlvaro GomezNo ratings yet
- NTSEMI and Unstable Angina ANdreaDocument17 pagesNTSEMI and Unstable Angina ANdreaandreaNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction Algorithmjitendra magarNo ratings yet
- Care Coordination With Referring PhysiciansDocument21 pagesCare Coordination With Referring Physiciansshemo hayatNo ratings yet
- ST Elevation Myocardial Infarction (STEMI) TalkDocument50 pagesST Elevation Myocardial Infarction (STEMI) TalkAfri YatiNo ratings yet
- 09.5 Hard Cases of NSTEMI Achmad Lefi MD FIHADocument29 pages09.5 Hard Cases of NSTEMI Achmad Lefi MD FIHAEmdan SengadjiNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction AlgorithmHan OWNo ratings yet
- Laporan Learning Objective Skenario 2 Blok Emergency: Sabrina Fazriesa 1418011194Document22 pagesLaporan Learning Objective Skenario 2 Blok Emergency: Sabrina Fazriesa 1418011194Sabrina FazriesaNo ratings yet
- Acs CCS 2021 KLDocument52 pagesAcs CCS 2021 KLPitchya WangmeesriNo ratings yet
- Ws Ahf - Intro Apicd 2017 - EditedDocument18 pagesWs Ahf - Intro Apicd 2017 - Editedvkhen88No ratings yet
- Interventional Cardiology Board Review (PDFDrive)Document62 pagesInterventional Cardiology Board Review (PDFDrive)wasimNo ratings yet
- Extra Acute Ischemic StrokeDocument52 pagesExtra Acute Ischemic Strokefyqmk4q8pkNo ratings yet
- Dual Antiplatelet Therapy After PCI in Patients atDocument32 pagesDual Antiplatelet Therapy After PCI in Patients atyamonaelgamNo ratings yet
- Hypertensive Crises - Current ApproachDocument35 pagesHypertensive Crises - Current ApproachShre RanjithamNo ratings yet
- Slide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSDocument20 pagesSlide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSsyahrial fazaNo ratings yet
- Conversion GateDocument25 pagesConversion GateThomas HenrryNo ratings yet
- ACS Final DraftDocument33 pagesACS Final Draftomcm17006No ratings yet
- Guidelines & Protocols: Stroke and Transient Ischemic Attack - Management and Prevention Advisory CommitteeDocument13 pagesGuidelines & Protocols: Stroke and Transient Ischemic Attack - Management and Prevention Advisory CommitteeAndi SaputraNo ratings yet
- Acute Coronay Syndrome - BACCDocument72 pagesAcute Coronay Syndrome - BACCYeyen Devyanti HandokoNo ratings yet
- Acs Review - Student VersionDocument3 pagesAcs Review - Student Versionapi-549451092No ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
- 02 ACS ManagemengtDocument38 pages02 ACS ManagemengtakeelNo ratings yet
- Antithrombotic and Thrombolytic Therapy For Ischemic Stroke Chest 2012Document36 pagesAntithrombotic and Thrombolytic Therapy For Ischemic Stroke Chest 2012dinaNo ratings yet
- Acute Coronary Syndrome (ACS) : Basic Principles For ACSDocument4 pagesAcute Coronary Syndrome (ACS) : Basic Principles For ACSRendra DananjayaNo ratings yet
- Panel Discussion ICACONDocument31 pagesPanel Discussion ICACONAnish H DaveNo ratings yet
- AtlsDocument32 pagesAtlsMahesh RajwalNo ratings yet
- Acute Coronary Syndrome & The PLATO Trial: Ticagrelor vs. ClopidogrelDocument42 pagesAcute Coronary Syndrome & The PLATO Trial: Ticagrelor vs. ClopidogrelDedeSumantraNo ratings yet
- POINT TrialDocument27 pagesPOINT TrialRutaNo ratings yet
- EHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationDocument41 pagesEHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationAmelia Maria LasloNo ratings yet
- Laporan Kasus: Myasthenia GravisDocument41 pagesLaporan Kasus: Myasthenia GravisTias DiahNo ratings yet
- ST-Elevation Myocardial Infarction (Stemi) : Present byDocument29 pagesST-Elevation Myocardial Infarction (Stemi) : Present byReema AlamriNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- Slide Speaker Candesartan For Hypertension in CKD PatientsDocument43 pagesSlide Speaker Candesartan For Hypertension in CKD Patientsesdras pramuditaNo ratings yet
- Update ACS Guidelines During PandemicDocument38 pagesUpdate ACS Guidelines During PandemicMuthiaNo ratings yet
- CCU 2017 AntiplateletDocument22 pagesCCU 2017 AntiplateletDhinie NovianiNo ratings yet
- Atrial Fibrillation TDDocument6 pagesAtrial Fibrillation TDapi-594366475No ratings yet
- Aha Guidelines StemiDocument94 pagesAha Guidelines StemiDika DekokNo ratings yet
- ATLS Advanced Trauma Life SupportDocument54 pagesATLS Advanced Trauma Life SupportdrofiliNo ratings yet
- ATLS Power Point PDFDocument54 pagesATLS Power Point PDFRizky LumalessilNo ratings yet
- NifedipineDocument11 pagesNifedipineTheaayu SukinoNo ratings yet
- Hemant Mahanand (201941103034) Case StudyDocument50 pagesHemant Mahanand (201941103034) Case StudyHemiNo ratings yet
- NSTEMIDocument29 pagesNSTEMIGeanina CreangaNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- Anti ArrhythmicsDocument46 pagesAnti Arrhythmicsmunim1192No ratings yet
- Kelantan Guidelines For Nsteacs 2nd Edition 2012 PDFDocument48 pagesKelantan Guidelines For Nsteacs 2nd Edition 2012 PDFAhmad Nafais RahimiNo ratings yet
- Case-Based Device Therapy for Heart FailureFrom EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenNo ratings yet
- DR Melisa Aziz APiCP2020 - CHD 4Document35 pagesDR Melisa Aziz APiCP2020 - CHD 4luckyariadneeNo ratings yet
- DR Vito Vascular ApicdDocument32 pagesDR Vito Vascular ApicdluckyariadneeNo ratings yet
- DR LulukDocument32 pagesDR LulukluckyariadneeNo ratings yet
- Sesi 2 DR Daniel Tanubudi SPJP FIXXDocument41 pagesSesi 2 DR Daniel Tanubudi SPJP FIXXluckyariadneeNo ratings yet
- Warsava, 2000. Prox - FemurDocument63 pagesWarsava, 2000. Prox - FemurluckyariadneeNo ratings yet
- Abstract Instruction 30th ASMIHA 4Document16 pagesAbstract Instruction 30th ASMIHA 4luckyariadneeNo ratings yet
- Closed Reduction, Traction, and Casting Techniques: Jason Tank, MDDocument75 pagesClosed Reduction, Traction, and Casting Techniques: Jason Tank, MDluckyariadneeNo ratings yet
- What Is A Bladder Diverticulum?Document3 pagesWhat Is A Bladder Diverticulum?luckyariadneeNo ratings yet
- Spina Bifida 2: NeuroDocument16 pagesSpina Bifida 2: NeuroluckyariadneeNo ratings yet
- Tibia-Open # MGDocument5 pagesTibia-Open # MGluckyariadneeNo ratings yet
- Tibial Non UnionsDocument9 pagesTibial Non UnionsluckyariadneeNo ratings yet
- NCP Drug StudyDocument8 pagesNCP Drug StudydennisNo ratings yet
- Muhammmad Nafidzul Izza061 SIStem TiaDocument6 pagesMuhammmad Nafidzul Izza061 SIStem TiaMarkocop XinNo ratings yet
- Classification of Dangerous DrugsDocument3 pagesClassification of Dangerous Drugsjinmenchie0% (1)
- What Does A Social Worker DoDocument2 pagesWhat Does A Social Worker DoRussel HoböNo ratings yet
- Glaxo Smith KlineDocument3 pagesGlaxo Smith KlineDarshan MeghjiNo ratings yet
- List of Dermatology Differential Diagnosis and Signs in DermatologyDocument54 pagesList of Dermatology Differential Diagnosis and Signs in DermatologyAhmadq76No ratings yet
- Family Care PlanDocument5 pagesFamily Care Planjay5ar5jamorabon5torNo ratings yet
- Skims Syllabus Staff NurseDocument9 pagesSkims Syllabus Staff NurseWani Zahoor50% (2)
- Healthy Sleep FsDocument4 pagesHealthy Sleep Fsvivek_sharma13No ratings yet
- Metastatic Bone DiseaseDocument34 pagesMetastatic Bone DiseaseHanif Andhika WardhanaNo ratings yet
- Final OSCE Script 220117Document18 pagesFinal OSCE Script 220117plethoraldorkNo ratings yet
- MassageDocument13 pagesMassageAjay IyerNo ratings yet
- Kirk Polka Student Generated Personal Project RubricDocument1 pageKirk Polka Student Generated Personal Project RubricKirk PolkaNo ratings yet
- Behavioral and Psychological Symptoms of Dementia (BPSDDocument17 pagesBehavioral and Psychological Symptoms of Dementia (BPSDChachaNo ratings yet
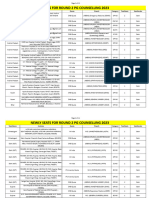
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarNo ratings yet
- Brodwin, Paul (1996) Medicine and Morality in Haiti The Contest For Healing PowerDocument256 pagesBrodwin, Paul (1996) Medicine and Morality in Haiti The Contest For Healing PowerFelipe SilvaNo ratings yet
- Alteraciones de La Motilidad Esofágica en La Manometría de Alta Resolución Clasificación de Chicago Versión 4.0Document29 pagesAlteraciones de La Motilidad Esofágica en La Manometría de Alta Resolución Clasificación de Chicago Versión 4.0Jorge Báez SepúlvedaNo ratings yet
- Top 10 Highest Paying Medical SpecialtiesDocument1 pageTop 10 Highest Paying Medical SpecialtiesGresjana RamajNo ratings yet
- Health Sciences in Early IslamDocument75 pagesHealth Sciences in Early IslameliNo ratings yet
- When You Can't Breathe, Nothing Else Matter: Presented by DR Parmeet BhatiaDocument140 pagesWhen You Can't Breathe, Nothing Else Matter: Presented by DR Parmeet Bhatiakamel6No ratings yet
- IIB Sant Pau 2020 WebDocument336 pagesIIB Sant Pau 2020 WebAinhoa GaNo ratings yet
- Focused ReviewDocument6 pagesFocused ReviewGina GiammalvoNo ratings yet
- KLK Loa - Muhammad Halim Bin Abdul WahidDocument3 pagesKLK Loa - Muhammad Halim Bin Abdul WahidHalimwahid HalimNo ratings yet
- Massive Haemorrhage PPT en PDFDocument18 pagesMassive Haemorrhage PPT en PDFviaereaNo ratings yet
- Appendectomy - NCPDocument6 pagesAppendectomy - NCPRhenzes HaraNo ratings yet
- A Handbook of Menstrual Diseases in Chinese MedicineDocument1,225 pagesA Handbook of Menstrual Diseases in Chinese MedicineJeffrey Paardekooper0% (1)
- LOGIQ P5 BrochureDocument8 pagesLOGIQ P5 BrochureHery Afrianto TariganNo ratings yet