Download as pdf or txt
You might also like
- Year 7 Drama Marking SheetDocument2 pagesYear 7 Drama Marking Sheetruthdoyle76No ratings yet
- CAMDEX. A Standardised Instrument For The Diagnosis of MentalDocument13 pagesCAMDEX. A Standardised Instrument For The Diagnosis of MentalLeila CamilaNo ratings yet
- Group Counseling Informed Consent For ParentsDocument1 pageGroup Counseling Informed Consent For Parentsapi-239096806No ratings yet
- Self-Regulation Assessment ScaleDocument2 pagesSelf-Regulation Assessment Scaleapi-383607481No ratings yet
- ChildDevelopmentAndTraumaGuide PDFDocument20 pagesChildDevelopmentAndTraumaGuide PDFCern GabrielNo ratings yet
- Early Expression of Autism Spectrum DisordersDocument39 pagesEarly Expression of Autism Spectrum Disordersjyoti mahajanNo ratings yet
- Executive Functions Diamond 2020Document17 pagesExecutive Functions Diamond 2020CamilaNo ratings yet
- Autism 07april 2019Document26 pagesAutism 07april 2019هلا دلبحNo ratings yet
- Unit 3 - Assessment of Individuals With ASDDocument17 pagesUnit 3 - Assessment of Individuals With ASDHeeta PanchasaraNo ratings yet
- Sensory Room Presentation Due 12Document9 pagesSensory Room Presentation Due 12api-582889983No ratings yet
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderDocument2 pagesAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasNo ratings yet
- WISCDocument8 pagesWISCMaham KhawajaNo ratings yet
- Treatmentmanual 29aug 2012Document207 pagesTreatmentmanual 29aug 2012Jovanka SolmosanNo ratings yet
- Childhood Autism Rating Scale, 2Nd Edition (Cars2)Document4 pagesChildhood Autism Rating Scale, 2Nd Edition (Cars2)Khadidja BoutouilNo ratings yet
- Specific Learning DisabilitiesDocument61 pagesSpecific Learning DisabilitiesShallu JoonNo ratings yet
- Sample Disorders Common Among Children and AdolescentsDocument39 pagesSample Disorders Common Among Children and AdolescentsAdilHumdaniNo ratings yet
- Emotional CPR - AustraliaDocument1 pageEmotional CPR - AustraliaSharon A Stocker0% (1)
- Interpretative Considerations IN THE DRAW A Person TEST Interpretative Considerations IN THE DRAW A Person TESTDocument13 pagesInterpretative Considerations IN THE DRAW A Person TEST Interpretative Considerations IN THE DRAW A Person TESTSuresh LukoseNo ratings yet
- Subjective Peripheral Neuropathy Screen QuestionnaireDocument1 pageSubjective Peripheral Neuropathy Screen QuestionnaireresearchNo ratings yet
- IDEAL List of Tools and AssessmentsDocument10 pagesIDEAL List of Tools and AssessmentsAbeliz Durant MunizNo ratings yet
- Development Assessment Scales: Chair Person: DR - Ami Patel Speaker:Dr - YogeshDocument24 pagesDevelopment Assessment Scales: Chair Person: DR - Ami Patel Speaker:Dr - YogeshTharindu WewaldeniyaNo ratings yet
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroNo ratings yet
- The Autism-Spectrum Quotient (AQ) : Evidence From Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and MathematiciansDocument13 pagesThe Autism-Spectrum Quotient (AQ) : Evidence From Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and MathematiciansDamian Maya0% (1)
- Measuring Oral Health and Quality of LifeDocument172 pagesMeasuring Oral Health and Quality of LifeCalin Dragoman100% (1)
- Global Development Delay (GDD) : DefinitionDocument2 pagesGlobal Development Delay (GDD) : DefinitionOmaima Al-shammakhi100% (1)
- Articulation ProblemDocument3 pagesArticulation ProblemErrorry JecksonNo ratings yet
- Dads and AutismDocument50 pagesDads and AutismcirclestretchNo ratings yet
- How I Use The Evidence in Dysphagia Management (1) : Prepared, Proactive and PreventativeDocument4 pagesHow I Use The Evidence in Dysphagia Management (1) : Prepared, Proactive and PreventativeSpeech & Language Therapy in PracticeNo ratings yet
- PBS Families PDFDocument10 pagesPBS Families PDFCandice Burch100% (1)
- 2 - Diagnostic Evaluation of Autism Spectrum DisordersDocument9 pages2 - Diagnostic Evaluation of Autism Spectrum DisordersAlice WernecNo ratings yet
- CARESOSA - Research Questions Set 1Document7 pagesCARESOSA - Research Questions Set 1Lucille CaresosaNo ratings yet
- Evidence Based Review of Interventions For Autism Used in or of Relevance To Occupational TherapyDocument14 pagesEvidence Based Review of Interventions For Autism Used in or of Relevance To Occupational Therapyapi-308033434No ratings yet
- Bi Ling SampleDocument12 pagesBi Ling Sampleirish xNo ratings yet
- Comcogtable 3 Summary All TestsDocument17 pagesComcogtable 3 Summary All TestsanamariapobleteNo ratings yet
- JoDD 17-1 26-37 Schroeder Et AlDocument12 pagesJoDD 17-1 26-37 Schroeder Et AlEspíritu Ciudadano100% (1)
- The Relationship Between Fine and Gross Motor Ability, Self-Perceptions and Self-Worth in Children and AdolescentsDocument11 pagesThe Relationship Between Fine and Gross Motor Ability, Self-Perceptions and Self-Worth in Children and AdolescentsHardeep Singh BaliNo ratings yet
- Self-Report Measures of Executive Functioning AreDocument8 pagesSelf-Report Measures of Executive Functioning AreLeonardo Castro RodríguezNo ratings yet
- Thematic Language-Stimulation TherapyDocument19 pagesThematic Language-Stimulation TherapyPipa Yau100% (1)
- Autism - Developmental-History-FormDocument12 pagesAutism - Developmental-History-Formmemphisosiris0No ratings yet
- Mock Referral ReportDocument7 pagesMock Referral ReportZach Selnes100% (1)
- Cognitive Behaviour Therapy With Children Who StutterDocument10 pagesCognitive Behaviour Therapy With Children Who StutterMaria RomeroNo ratings yet
- Positive Behaviour SupportsDocument1 pagePositive Behaviour SupportsCandice BurchNo ratings yet
- Guidelines Down Syndrome Assessment and Intervention PDFDocument292 pagesGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaNo ratings yet
- Psychology Assessment - I - M1Document42 pagesPsychology Assessment - I - M1Brinda ChughNo ratings yet
- An Update On The Comorbidity of ADHD and ASDDocument16 pagesAn Update On The Comorbidity of ADHD and ASDCristina SolerNo ratings yet
- Final Group Counseling Project - Stress ManagementDocument82 pagesFinal Group Counseling Project - Stress Managementapi-548101945No ratings yet
- Cognitive Development For StudentsDocument94 pagesCognitive Development For StudentsaplesgjskNo ratings yet
- 2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthDocument3 pages2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthCaio MayrinkNo ratings yet
- F.5 Selective Mutism Powerpoint 2016Document32 pagesF.5 Selective Mutism Powerpoint 2016Ptrc Lbr LpNo ratings yet
- Dorothy V.M. Bishop-David McDonald-2009Document16 pagesDorothy V.M. Bishop-David McDonald-2009Inma MéndezNo ratings yet
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocument7 pagesThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALNo ratings yet
- Effectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenDocument6 pagesEffectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenYanuar Adi SanjayaNo ratings yet
- Social Communication Assessment After Traumatic Brain Injury A Narrative Review of Innovations in Pragmatic and Discourse Assessment MethodsDocument15 pagesSocial Communication Assessment After Traumatic Brain Injury A Narrative Review of Innovations in Pragmatic and Discourse Assessment MethodsPapato KongNo ratings yet
- Language and Literacy Disorders Sivaswetha RDocument14 pagesLanguage and Literacy Disorders Sivaswetha RSriram Manikantan100% (1)
- Mental Health & Wellbeing For Children & Young People - Part TwoDocument24 pagesMental Health & Wellbeing For Children & Young People - Part Twomariya khanNo ratings yet
- Diagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Document17 pagesDiagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Betania MendozaNo ratings yet
- M Torres Neuropsychological Report 5Document12 pagesM Torres Neuropsychological Report 5Reyna De AlbaNo ratings yet
- Obsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsDocument6 pagesObsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsJorge VelardeNo ratings yet
- Attention-Deficit/Hyperactivity Disorder (Adhd) : Cecil R. Reynolds, PHD Randy W. Kamphaus, PHDDocument3 pagesAttention-Deficit/Hyperactivity Disorder (Adhd) : Cecil R. Reynolds, PHD Randy W. Kamphaus, PHDashrafasdNo ratings yet
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeFrom EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNo ratings yet
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeFrom EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeNo ratings yet
- A Systematic Review of What Barriers and Facilitators Prevent and Enable Physical Healthcare Services Access For Autistic AdultsDocument14 pagesA Systematic Review of What Barriers and Facilitators Prevent and Enable Physical Healthcare Services Access For Autistic AdultsLoreto Opazo RojasNo ratings yet
- Agenesis of The Corpus Callosum - Genetic, Developmental and Functional Aspects of ConnectivityDocument13 pagesAgenesis of The Corpus Callosum - Genetic, Developmental and Functional Aspects of ConnectivityLoreto Opazo RojasNo ratings yet
- Clinical Assessment, Genetics, and Treatment Approaches in ASDDocument18 pagesClinical Assessment, Genetics, and Treatment Approaches in ASDLoreto Opazo RojasNo ratings yet
- 10.1 Pharmacological Therapy of Autism Spectrum DisorderDocument7 pages10.1 Pharmacological Therapy of Autism Spectrum DisorderLoreto Opazo RojasNo ratings yet
- Autism - Cause Factors, Early Diagnosis and TherapiesDocument10 pagesAutism - Cause Factors, Early Diagnosis and TherapiesLoreto Opazo RojasNo ratings yet
- Penumbra IsquémicaDocument7 pagesPenumbra IsquémicaLoreto Opazo RojasNo ratings yet
- Why Non Speech Oral Motor Exercises Are Not WarrantedDocument13 pagesWhy Non Speech Oral Motor Exercises Are Not WarrantedLoreto Opazo RojasNo ratings yet
- 1.1 Lenguaje, DS y AfasiaDocument6 pages1.1 Lenguaje, DS y AfasiaLoreto Opazo RojasNo ratings yet
- Evaluación de La Deglución Con NasofibroscopíaDocument7 pagesEvaluación de La Deglución Con NasofibroscopíaLoreto Opazo RojasNo ratings yet
- Anullment CATHOLIC TRIBUNALDocument20 pagesAnullment CATHOLIC TRIBUNALMons Jr BaturianoNo ratings yet
- Manual de Partes-HISTER 9 Ton.Document556 pagesManual de Partes-HISTER 9 Ton.Juan PabloNo ratings yet
- Allen Bradley 160 C SeriesDocument28 pagesAllen Bradley 160 C SeriesTihomir Matulić100% (1)
- Statistical Methods For Spatial Data AnalysisDocument3 pagesStatistical Methods For Spatial Data Analysissakali ali0% (1)
- SAP Kernel 720Document24 pagesSAP Kernel 720rajaraobhmNo ratings yet
- 900FH&1000FH TurbinesDocument12 pages900FH&1000FH TurbinesRyanNo ratings yet
- Mathematics: Quarter 1 - Module 8: Division of Whole Numbers by Decimals Up To 2 Decimal PlacesDocument34 pagesMathematics: Quarter 1 - Module 8: Division of Whole Numbers by Decimals Up To 2 Decimal PlacesJohn Thomas Satimbre100% (1)
- Transducer Engineering Lab ManualDocument44 pagesTransducer Engineering Lab Manualspgmaniarunagiri100% (2)
- Curiculum Vitae JurnalisDocument1 pageCuriculum Vitae JurnalisEh Ada UjankNo ratings yet
- Chechk List Fokker 50Document1 pageChechk List Fokker 50Felipe PinillaNo ratings yet
- LISI AEROSPACE - PULL-STEM™ and PULL-IN™ PinsDocument6 pagesLISI AEROSPACE - PULL-STEM™ and PULL-IN™ PinsLeandro González De CeccoNo ratings yet
- Artikel 5Document26 pagesArtikel 5Surya DhNo ratings yet
- Student Performance Contract With Parents AgreementDocument1 pageStudent Performance Contract With Parents AgreementCURT KEANU VILLANUEVANo ratings yet
- Bread Board - Transformer - PCB - Soldering - LectureDocument31 pagesBread Board - Transformer - PCB - Soldering - Lectureananyautkarsh140904No ratings yet
- Model Course 1.07 PDFDocument75 pagesModel Course 1.07 PDFShiena CamineroNo ratings yet
- Volume AdministrationDocument264 pagesVolume AdministrationeviyipyipNo ratings yet
- 14 Sept Quiz Chapter 1 SoalanDocument5 pages14 Sept Quiz Chapter 1 SoalanLukman MansorNo ratings yet
- Dry Concentrator IntroductionDocument6 pagesDry Concentrator Introductionmanuel3021No ratings yet
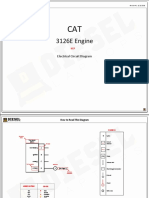
- 3126E Engine: Electrical Circuit DiagramDocument10 pages3126E Engine: Electrical Circuit DiagramPhil B.No ratings yet
- Rollarc 400Document48 pagesRollarc 400m khNo ratings yet
- Error - Failed To Compute Elastoplastic Strain Variables - 1150 - Knowledge Base PDFDocument3 pagesError - Failed To Compute Elastoplastic Strain Variables - 1150 - Knowledge Base PDFmatinNo ratings yet
- Paper 1 Each Questions Is Followed by Options A, B, and C. Circle The Correct AnswerDocument9 pagesPaper 1 Each Questions Is Followed by Options A, B, and C. Circle The Correct AnswerWan SafinaNo ratings yet
- Memory Based Paper Sbi Clerk 11th July 2 266bb4c1Document72 pagesMemory Based Paper Sbi Clerk 11th July 2 266bb4c1SHIVANI chouhanNo ratings yet
- Ag Test Package FormatDocument25 pagesAg Test Package FormatoparoystNo ratings yet
- GE4.2 Bearing Capacity EquationsDocument66 pagesGE4.2 Bearing Capacity EquationsInter Galactic0% (1)
- 42 Annual Conference of Linguistic Society of Nepal (42nd LSN)Document9 pages42 Annual Conference of Linguistic Society of Nepal (42nd LSN)Nani Babu GhimireNo ratings yet
- Astm d7091 13Document10 pagesAstm d7091 13Anonymous zia5og7psNo ratings yet
- Noun (Subject) + Verb + The + Superlative Adjective + Noun (Object)Document6 pagesNoun (Subject) + Verb + The + Superlative Adjective + Noun (Object)anaNo ratings yet
- Moral Stories - Situated Reasoning About Norms, Intents, Actions, and Their Consequences 2012.15738Document21 pagesMoral Stories - Situated Reasoning About Norms, Intents, Actions, and Their Consequences 2012.15738Zhu XUNo ratings yet