Download as pdf or txt
You might also like
- Foodstamp LetterDocument6 pagesFoodstamp LetterTemisha BrownNo ratings yet
- Volcano BrochureDocument2 pagesVolcano BrochureSamantha Reonal92% (12)
- CA DMV Receipt: 1 MessageDocument1 pageCA DMV Receipt: 1 MessageJuan MoraNo ratings yet
- A Single Father's Tax Situation ResponseDocument2 pagesA Single Father's Tax Situation ResponseJenn4459No ratings yet
- Covid Test-PositiveDocument2 pagesCovid Test-PositiveSuresh VarmaNo ratings yet
- All in A Health 05976Document2 pagesAll in A Health 05976mike jonesNo ratings yet
- Your Receipt: Motor Vehicle Administration 6601 Ritchie Highway, N.E. Glen Burnie, Maryland 21062Document2 pagesYour Receipt: Motor Vehicle Administration 6601 Ritchie Highway, N.E. Glen Burnie, Maryland 21062Dan Beard100% (1)
- VW Audi Credit AppDocument1 pageVW Audi Credit AppSaaNo ratings yet
- Juul Labs v. Eonsmoke - ComplaintDocument188 pagesJuul Labs v. Eonsmoke - ComplaintSarah BursteinNo ratings yet
- CTN Cash and Carry V Gallaher Case DigestDocument6 pagesCTN Cash and Carry V Gallaher Case DigestNicole YauNo ratings yet
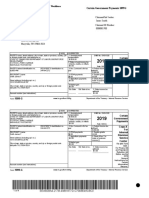
- CertainGovernmentPayments1099G JamesSmith-654202001310815Document4 pagesCertainGovernmentPayments1099G JamesSmith-654202001310815ireaditallNo ratings yet
- Rishabh Gupta PDFDocument3 pagesRishabh Gupta PDFrishabhNo ratings yet
- Drug-Test 8.26Document1 pageDrug-Test 8.26Jc MeNo ratings yet
- MONETARYDETERMINATIONPANDEMICUNEMPLOYMENTASSISTANCE jASONKROLL-3824202010074018 PDFDocument3 pagesMONETARYDETERMINATIONPANDEMICUNEMPLOYMENTASSISTANCE jASONKROLL-3824202010074018 PDFjuanchy12No ratings yet
- Regional Acceptance Ach Draft Form-OneDocument2 pagesRegional Acceptance Ach Draft Form-Onejohnlove720% (1)
- Disaster Business Loan ApplicationDocument4 pagesDisaster Business Loan ApplicationalexNo ratings yet
- 12.23.22 Pardon CertificatesDocument10 pages12.23.22 Pardon CertificatesLakeCoNewsNo ratings yet
- Complaint For Divorce: Virginia: in The - Court For TheDocument3 pagesComplaint For Divorce: Virginia: in The - Court For TheLucie AuerNo ratings yet
- Formsoppsapplication Illinois Birth Record 2018Document2 pagesFormsoppsapplication Illinois Birth Record 2018CynthiaNo ratings yet
- Car Hire Policy DocumentDocument19 pagesCar Hire Policy DocumentGabor SzucsNo ratings yet
- Shaw 3 Law Firm Is Now Taking On Clients For CPS Defense CasesDocument3 pagesShaw 3 Law Firm Is Now Taking On Clients For CPS Defense CasesPR.comNo ratings yet
- Georgia Power Utility AssistanceDocument2 pagesGeorgia Power Utility AssistanceABC15 NewsNo ratings yet
- Your 2020 Social Security Cost of Living Increase 2019Document4 pagesYour 2020 Social Security Cost of Living Increase 2019henryNo ratings yet
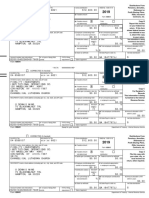
- CORRECTED (If Checked)Document2 pagesCORRECTED (If Checked)Dennis100% (1)
- Earnings Statement: Non NegotiableDocument1 pageEarnings Statement: Non NegotiableKang KimNo ratings yet
- PenFed Signature PageDocument3 pagesPenFed Signature PageL KNo ratings yet
- Mercedes Reg Renew 2020 PDFDocument1 pageMercedes Reg Renew 2020 PDFMood SwingNo ratings yet
- Better Covid ThingDocument4 pagesBetter Covid ThingAuguste RiedlNo ratings yet
- Rent Payment 20febDocument2 pagesRent Payment 20febjadeisangryNo ratings yet
- Including The Long Form Fee Disclosure ("List of All Fees.")Document9 pagesIncluding The Long Form Fee Disclosure ("List of All Fees.")Shamara LoganNo ratings yet
- NY Drivers License HistoryDocument8 pagesNY Drivers License HistoryMarco De Moor BeyNo ratings yet
- Please DocuSign These Documents UPS On-BoardDocument21 pagesPlease DocuSign These Documents UPS On-BoardJayeven EnglishNo ratings yet
- Application For Texas Cerificate of TitleDocument2 pagesApplication For Texas Cerificate of TitleRobert CookNo ratings yet
- Apartment Lease Contract: Moving in - General InformationDocument23 pagesApartment Lease Contract: Moving in - General InformationNoel RivasNo ratings yet
- Business Loan Application - NEWDocument8 pagesBusiness Loan Application - NEWSarah AndersonNo ratings yet
- F 941Document4 pagesF 941gopaljiiNo ratings yet
- Notice of Monetary RedeterminationDocument4 pagesNotice of Monetary RedeterminationDennisNo ratings yet
- Request For Taxpayer Identification Number and CertificationDocument4 pagesRequest For Taxpayer Identification Number and CertificationLogan BairdNo ratings yet
- Alabama Lawsuit Against Former Cape Coral CoupleDocument22 pagesAlabama Lawsuit Against Former Cape Coral CoupleMichael BraunNo ratings yet
- Valid Documents List PDFDocument3 pagesValid Documents List PDFVikkiNo ratings yet
- 2019 1099-Consol Morgan Stanley 5948 KentDocument10 pages2019 1099-Consol Morgan Stanley 5948 Kentesteysi775No ratings yet
- Application For Social Security Card - Ss-5Document1 pageApplication For Social Security Card - Ss-5Casey Orvis100% (1)
- How To Get What The US Government Owes You!Document4 pagesHow To Get What The US Government Owes You!creativemarcoNo ratings yet
- DocuSign PDFDocument7 pagesDocuSign PDFLourdesNo ratings yet
- Teaching CertificateDocument1 pageTeaching Certificateapi-359162285No ratings yet
- February BOA StatementDocument4 pagesFebruary BOA StatementhayyandaiNo ratings yet
- Feb BOADocument8 pagesFeb BOAadairlaciNo ratings yet
- Us 1099 2022Document4 pagesUs 1099 2022mks12No ratings yet
- Self Certification of Social Security NumberDocument1 pageSelf Certification of Social Security NumberSheldon OrrNo ratings yet
- View PDF FormDocument1 pageView PDF FormKathryn NightwineNo ratings yet
- Loa Kong YuenDocument5 pagesLoa Kong YuenLuberto Dwi100% (1)
- Chepter .1. Evaluate Marketing Plan: Marketing Strategy of Idbi BankDocument68 pagesChepter .1. Evaluate Marketing Plan: Marketing Strategy of Idbi BankNaseem ChoudharyNo ratings yet
- Business LoansDocument25 pagesBusiness LoansMai TiếnNo ratings yet
- Georgia GatewayDocument4 pagesGeorgia GatewayEmmanuel MartinsNo ratings yet
- Usa Id Card Front and Back - Google SearchDocument1 pageUsa Id Card Front and Back - Google Searchabdulkabirolamilekan56No ratings yet
- American Founders Bank's Letter To CustomersDocument4 pagesAmerican Founders Bank's Letter To CustomersCourier JournalNo ratings yet
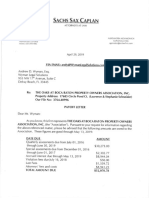
- Payoff Letter From Gonzalez, Counsel Sachs Sax Caplan For Oaks at Boca Raton Property Owners AssociationDocument4 pagesPayoff Letter From Gonzalez, Counsel Sachs Sax Caplan For Oaks at Boca Raton Property Owners Associationlarry-612445100% (1)
- Best Western Plus HotelDocument1 pageBest Western Plus Hoteler_atunugoraiNo ratings yet
- Low Cost or Free Dental Services 1Document1 pageLow Cost or Free Dental Services 1probativeinfoNo ratings yet
- Application Tenant Rent&UtilityAssistance 658250Document30 pagesApplication Tenant Rent&UtilityAssistance 658250morepal2No ratings yet
- Constitution of the State of Minnesota — Republican VersionFrom EverandConstitution of the State of Minnesota — Republican VersionNo ratings yet
- What Are The Major Impacts of China's Cultural Revolution?Document14 pagesWhat Are The Major Impacts of China's Cultural Revolution?vkisho5845No ratings yet
- What Is The Substation Automation System (SAS) and What You MUST Know About ItDocument24 pagesWhat Is The Substation Automation System (SAS) and What You MUST Know About Itዛላው መናNo ratings yet
- Pvh56 Pvh63 Parts and ServiceDocument8 pagesPvh56 Pvh63 Parts and ServiceRiki AkbarNo ratings yet
- Condition Assessment of SeawallsDocument7 pagesCondition Assessment of SeawallsJIBEESH01No ratings yet
- Prevalence and Determinants of Substance Use Among Students at Kampala International University Western Campus, Ishaka Municipality Bushenyi District UgandaDocument18 pagesPrevalence and Determinants of Substance Use Among Students at Kampala International University Western Campus, Ishaka Municipality Bushenyi District UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- 13 - HOLCIM Occupational Safety and Health Uwe BarkmannDocument22 pages13 - HOLCIM Occupational Safety and Health Uwe Barkmannhuylan2204No ratings yet
- SHRB-SN: 1" (25 MM) Deflection SHRB Spring Hanger With Neoprene and Bottom CupDocument1 pageSHRB-SN: 1" (25 MM) Deflection SHRB Spring Hanger With Neoprene and Bottom Cupsas999333No ratings yet
- Business ProposalDocument35 pagesBusiness ProposalMJ MacapagalNo ratings yet
- Comm 10Document2 pagesComm 10boopNo ratings yet
- IIAS 1.0.21 - Columnar Incremental Schema Backup and Restore Feature - 1Document12 pagesIIAS 1.0.21 - Columnar Incremental Schema Backup and Restore Feature - 1HS UFNo ratings yet
- Key A2 Basic Level English Exam PDFDocument4 pagesKey A2 Basic Level English Exam PDFakhilesh sahooNo ratings yet
- PrepositionDocument5 pagesPrepositionsourov07353No ratings yet
- Naive BayesDocument36 pagesNaive BayesgibthaNo ratings yet
- Feedback XI G PRA MID-TERM EP 2Document8 pagesFeedback XI G PRA MID-TERM EP 2Syifa KamilaNo ratings yet
- Basic Civil Engineering: V.K SinghDocument32 pagesBasic Civil Engineering: V.K SinghVikash SinghNo ratings yet
- Emma Sconyers, "I Carry You in My Heart: Facing An Incurable Prenatal Diagnosis"Document40 pagesEmma Sconyers, "I Carry You in My Heart: Facing An Incurable Prenatal Diagnosis"MIT Comparative Media Studies/WritingNo ratings yet
- NEW Garrett TV83 Turbo Repair Kit 468267-0000Document10 pagesNEW Garrett TV83 Turbo Repair Kit 468267-0000thomaskarakNo ratings yet
- Zeus - AntipasDocument2 pagesZeus - AntipasPaw LabadiaNo ratings yet
- End of Quiz: G-LITT001 CEE22 1st Sem (2023-2024) Review Quiz 6Document3 pagesEnd of Quiz: G-LITT001 CEE22 1st Sem (2023-2024) Review Quiz 6Dela Cruz ArabellaNo ratings yet
- The Untouchables and The Pax Britannica Dr. B.R.ambedkarDocument61 pagesThe Untouchables and The Pax Britannica Dr. B.R.ambedkarVeeramani ManiNo ratings yet
- References and AddendumsDocument12 pagesReferences and Addendumsapi-268922965No ratings yet
- Fariha (MGT 212)Document11 pagesFariha (MGT 212)Rabib AhmedNo ratings yet
- Twelve Principles SMC2017 2Document65 pagesTwelve Principles SMC2017 2Fadel PratamaNo ratings yet
- Formatted SBI Clerk Mains Previous Year Paper 2021Document78 pagesFormatted SBI Clerk Mains Previous Year Paper 2021shyamveer147No ratings yet
- Adam&Eve 5Document4 pagesAdam&Eve 5Victor B. MamaniNo ratings yet
- Science DLPDocument12 pagesScience DLPGaila Mae SanorjoNo ratings yet
- Hoogendoorn Anniversary Magazine - 50 Years - LRDocument20 pagesHoogendoorn Anniversary Magazine - 50 Years - LRtachetNo ratings yet
- Econchella PDFDocument2 pagesEconchella PDFSanjana JobiNo ratings yet