Professional Documents
Culture Documents
Consequences of Early Extraction of Compromised Fi
Consequences of Early Extraction of Compromised Fi
Uploaded by
Maria MagdalenaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Consequences of Early Extraction of Compromised Fi
Consequences of Early Extraction of Compromised Fi
Uploaded by
Maria MagdalenaCopyright:
Available Formats
Saber et al.
BMC Oral Health (2018) 18:59
https://doi.org/10.1186/s12903-018-0516-4
RESEARCH ARTICLE Open Access
Consequences of early extraction of
compromised first permanent molar:
a systematic review
Afnan M. Saber1†, Doua H. Altoukhi1†, Mariam F. Horaib1†, Azza A. El-Housseiny1,2, Najlaa M. Alamoudi1*
and Heba J. Sabbagh1
Abstract
Background: The aim of this study was to systematically review the literature to determine the sequelae of early
extraction of compromised first permanent molars (FPMs) with regard to the skeletal and dental development of
5- to 15-year-old children. Meta-analysis was conducted when applicable.
Methods: Our research protocol included a search strategy, inclusion/exclusion criteria, and a data extraction plan.
The search engines used were PubMed, Scopus, and Science Direct. Study selection was performed independently
by three reviewers. Articles published from 1960 to 2017 were reviewed based on inclusion and exclusion criteria.
Meta-analysis was performed to compare space closure between upper and lower arches.
Results: Eleven studies fulfilled the inclusion criteria. The consequences were decrease in post extraction space,
accelerated development and eruption of second permanents molars (SPMs) and third molars, a decrease in caries
and/or fillings on the proximal surfaces of adjacent teeth, lingual tipping and retrusion of incisors, and counter
clockwise rotation of the occlusal plane.
Conclusion: There were several consequences of early extraction of FPMs, which were related to skeletal and dental
development. Our systematic review suggests that comprehensive evaluation of the compromised FPMs should be
performed before planning an extraction. The ideal time for FPM extraction is when the SPM is at the early bifurcation
stage in order to achieve complete closure of the extraction space by the SPM. Benefits should be weighed over the
risks to decrease the risk of unfavorable outcomes as much as possible. However, due to the limited evidence on the
outcomes and variables that influence them, high-quality prospective studies are needed.
Keywords: First permanent molar, Early extraction, Early loss, Result or effect of extraction, Children
Background Many factors should be considered before determining
Dental caries is the most common infectious disease the appropriate treatment method for a badly decayed
worldwide [1]. Globally, 60%–90% of school children FPM, such as the level of crown destruction, the degree
have dental caries [2]. The first permanent molar of pulp maturation, the status of the developing denti-
(FPM) emerges early, so is more prone to dental car- tion, the severity of dental pain, the attitude of the
ies and possible premature extraction before 15 years child’s parent(s), and the patient’s ability to withstand
of age. The importance of this tooth lies in its major long treatment under local anesthesia. Accordingly,
role in maintaining normal masticatory function and some clinicians favor early extraction of these teeth be-
dentofacial harmony [3]. cause they are more likely to have a poor prognosis and
require extraction later on [4]. On the other hand, others
prefer to restore an extensively decayed FPM. Extraction
* Correspondence: nalamoudi@kau.edu.sa
†
Equal contributors
of FPMs may be highly considered or not depending on
1
Pediatric Dentistry Department, Faculty of Dentistry, King Abdulaziz treatment consequences and outcomes [5].
University, P.O. Box 80209, Jeddah 21589, Saudi Arabia
Full list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0
International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and
reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to
the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver
(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 2 of 15
In view of the controversy regarding the consequences Data extraction
of early extraction of compromised FPMs, this system- Data were extracted from eligible papers by the three in-
atic review of the literature was undertaken to determine vestigators working independently and included the fol-
the effects and sequelae of early extraction of these teeth lowing: site and country, study design, setting, duration,
with regard to the skeletal and dental development of sample size, age of the patient population at the time of
children aged 5–15 years. Meta-analysis was carried out extraction, duration of follow-up, and methods used to
when applicable. evaluate the consequences of early extraction of the
FPM. Only information specifically related to our
research was extracted from the eligible articles.
Methods
Literature search Meta-analysis
We registered our research topic at the Center for A meta-analysis was carried out to compare the fre-
Reviews and Dissemination (registration number quency of spontaneous space closure following FPM
CRD42015020275). We developed a research protocol extraction in the maxilla with that of the mandible
that included a search strategy, inclusion/exclusion using Review Manager Software (Rev Man 5.1, Cochrane
criteria, and a data extraction plan. The search started Collaboration). The Mantel-Haenszel method was used to
in May 2015 and ended in 2017. The search strategy combine the studies for calculation of summary odds ra-
comprised key words used separately or in various tios and 95% confidence intervals [8]. To decide whether
combinations (“first permanent molar tooth”, “early the results of the separate studies could be combined
extraction”, “early loss”, “results” and “effects”), and meaningfully, a statistical test of homogeneity was carried
was performed in three search engines (PubMed, Sco- out. Based on the chi-square test, an inconsistency coeffi-
pus, and Science Direct) from 1960 to 2017. No lan- cient (I2 statistic) was computed where a value of more
guage restriction was imposed. than 50% indicated moderate heterogeneity and a value of
more than 75% indicated high heterogeneity [9]. The odds
Study selection ratios were pooled with a random effects model for
Article titles were assessed for eligibility by three in- heterogeneous studies. Odds ratios with their 95%
vestigators (AMS, DHA, MFH) independently. Ab- confidence limits for the individual studies and a
stracts of studies with favorable titles were reviewed. summary estimate of effect were graphically displayed
Studies that appeared from the abstract to be unre- in a forest plot.
lated to the topic were excluded at this point. The When possible, we calculated odds ratios and confi-
reference lists of the full-text papers were screened dence intervals for extraction and non-extraction groups
for further relevant studies. The full-text papers were in studies missing this information. The chi-square stat-
then screened by the above-mentioned three investi- istic and p-value were calculated to compare the upper
gators separately and together according to predefined and lower arch space closure values in studies where a
inclusion and exclusion criteria. Authors identified to relationship between them was shown.
have undertaken research related to the consequences
of FPM extraction were contacted with a request for Strengths and limitations of the included studies
access to their unpublished data. The three investigators evaluated the strengths and limi-
tations of the considered articles separately and then dis-
cussed them together. Any disagreement was resolved
Eligibility criteria by consensus. The strengths and limitations of the stud-
The following inclusion criteria were applied: a clinical ies were evaluated according to the STROBE (Strength-
trial, case-control, cross-sectional or cohort study de- ening the Reporting of Observational Studies in
sign; patient age 5 years (time when FPM eruption Epidemiology) checklist. This checklist consists of 22
starts) to 15 years (time of complete eruption of second items that should be reported in the title, abstract, intro-
permanent molar [SPM]) [6] at the time of extraction; duction, methods, results and discussion sections of
and extraction of FPM due to caries or hypomineraliza- published studies, and used to assess the main observa-
tion. The exclusion criteria were: other study design, tional studies, i.e., cohort, case-control and cross-
such as a case report; patient aged older than 15 years sectional studies [10]. All reported items, especially in
or younger than 5 years [6] at the time of extraction; ex- the methods and results sections of the included articles,
traction of a tooth other than the FPM; and extraction were considered a strength of the study, while all miss-
of FPM as an orthodontic treatment. One study in the ing items were considered a weak point. The strength of
Turkish language [7] was translated to English by a na- each article was scored according to the STROBE check-
tive speaker of the Turkish language. list: 1–7 (poor strength), 8–15 (moderate strength), and
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 3 of 15
16–22 (high strength). We also used the system devised Study characteristics
by Shekelle et al. to grade the evidence and classify the Eight of the included studies were cross-sectional [12–19],
strength of the recommendations in the included articles two were case-control [7, 20], and one was prospective
[11] (Additional file 1). and observational [21]. One study [12] was excluded be-
cause the data for malocclusion as an outcome of FPM ex-
traction were invalid; in addition, the criteria used to
Results classify normal and abnormal malocclusion were not uni-
Study selection form or acceptable. Table 1 shows the characteristics and
Our search strategy yielded 1602 hits, comprising 148 in outcomes of the included studies.
PubMed, 194 in Scopus, and 1260 in Science Direct. Du-
plicates were removed, leaving 1554 titles. Of these titles, Outcomes
68 studies were approved for evaluation; their abstracts The consequences of early FPM extraction reported
were screened and those that were beyond the scope of in the selected papers were as follows: effects on
our research were excluded, leaving 29 studies. Refer- post extraction space; effects on development and
ences of full-text articles were checked for related arti- eruption of the SPM and third molar; caries and/or
cles. Five articles were added from the references. The fillings in adjacent teeth; effects on incisors; and
full texts of these studies were acquired and screened ac- effects on skeletal development.
cording to their inclusion and exclusion criteria. The
remaining articles were excluded due to either ortho- Effects on post extraction space
dontic treatment or older age at the time of extraction. Six articles reported changes in the post extraction
No additional information was obtained by contacting space. One was a case-control, split-mouth study [7] that
authors for their unpublished data. The final result was analyzed linear and angular changes in the SPM and second
eleven articles (Fig. 1). premolar adjacent to the extraction site in cephalometric
Fig. 1 Flow diagram of study selection process
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Table 1 Characteristics and outcomes of included studies
Reference Site/Country Duration Study design Sample size Age at Age at Method of Findings P-value or
time of time of assessment OR and CI
Extraction Non- Extraction group Non-extraction
extraction evaluation
group extraction group
group
Effects on post extraction space
Telli and Turkey 1988– Case-control 40 (T) 28 (T) 9.5 years 10.5 Years Comparison of Mean change in Mean change in P < 0.05*
Aytan, 1989 Split-mouth panoramic X-rays at maxillary SPM maxillary SPM for change
1989 [7] extraction and a year angle and distance, angle and distance, in
later 15.65° and − 2.40o and extraction
Comparison of 0.18 mm, 0.10 mm, group; P >
cephalometric respectivelyMean respectivelyMean 0.05 for
radiograph angles change in maxillary change in maxillary change in
Saber et al. BMC Oral Health (2018) 18:59
and distances at second premolar second premolar non-
extraction and a year angle and distance, angle and distance, extraction
later − 5.68° and − 2.33° and 0.53 mm, group
(Angles: between 2.58 mm, respectively P < 0.05*
long access of the respectively Mean change in for change
SPM or second Mean change in mandibular SPM in
premolar and mandibular SPM angle and distance, extraction
Frankfort horizontal angle and distance, 0.96° and 1.15 mm, group, P >
plane in the maxilla 4.62° and 3.83 mm, respectively 0.05 for
and the occlusal respectively Mean change in change in
plane in the Mean change in mandibular second non-
mandible) (distances: mandibular second premolar angle extraction
between the distal premolar angle and and distance, 5.08° group
surface of the upper distance, − 4.63° and 0.54 mm, P < 0.05*
SPM or second and − 1.82 mm, respectively for change
premolar and respectively in
pterygomaxillary extraction
fissure in the maxilla group, P >
and the distance 0.05 for
between the lower change in
SPM or second non-
premolar and the extraction
ramus of the group
mandible) P < 0.05*
for change
in
extraction
group, P >
0.05 for
change in
non-
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
extraction
group
Jälevik Specialist Clinic of NA Cross-sectional 27 subjects NA Median Median Eruption of 23/27 (85.2%) NA Difference
and Pedodontics, (16 girls and age 8.2 age 13.9 permanent dentition, subjects had between
Möller, Sahlgrenska 11 boys) 66 (range (range and space closure spontaneous mandible
2007 University Hospital, (T) 5.6–12.7) 12.1–19) were documented closure 52/66 and
[14] Mölndal, Department years years by: (78.8%) (T)
Page 4 of 15
Table 1 Characteristics and outcomes of included studies (Continued)
Reference Site/Country Duration Study design Sample size Age at Age at Method of Findings P-value or
time of time of assessment OR and CI
Extraction Non- Extraction group Non-extraction
extraction evaluation
group extraction group
group
of Pedontontics, Panoramic X-ray 31/38 (81.6%) maxilla P =
Faculty of Dental casts Spontaneous space 0.518
Odontology, Bitewings closure, maxilla χ2 = 0.42
Göteborg University, 21/28 (75%) OR: 1.48
Sweden Spontaneous space CI: (0.45,
closure, mandible 4.83)
Rãducanu et al., Paediatric 2001–2007 Cross- sectional,hospital- 17 subjects NA 9–15 years
2009 [16] Dentistry based 22 (T)
Saber et al. BMC Oral Health (2018) 18:59
Department, Six maxillary and 16
Dental Medicine mandibular
Faculty of the
UMF Carol Davila,
Bucharest,
Romania
NA Intraoral examination 10/22 spontaneous NA Difference
using dental mirror (45.5%) space closure between
and graduated probe with 2/6 (33.3%) with mandible
to evaluate post- maxillary and maxilla
extraction space spontaneous P = 0.024*
space closure χ2 = 5.1
8/16 (50%) with OR = 0.50 CI
mandibular (0.07, 3.55)
spontaneous
space closure
Teo et Paediatric 2008– Cross-sectional 63 subjects NA 7–13 Mean age Panoramic X-ray to 101/127 (79.5%) NA Difference
al., 2013 DentistryDepartment 2013 Hospital based 236 (T) (mean 8.9) 13.7 years assess Demirjian’s de- spontaneous space between
[18] in a London-based 127 SPM at years velopmental stages closure mandible
dental hospital, UK Demirjian of SPM and to assess 59/63 (94%) had and
stage E *** space closure be- spontaneous space maxilla
(63 tween the contact closure in maxilla P = 0.0001*
maxillary, 64 point of the second 42/64 (66%) had χ2 = 15.32
mandibular) premolar and the spontaneous space OR = 7.73
SPM using a ruler closure in mandible CI (2.48,
When SPM at stage 24.07)
E***)
Rahhal, Arab-American NA Prospective 52 (T) NA 10.5 years NA Panoramic X-ray to 44/52 (84.6%) NA NA
2014 University Clinic, observational (maxillary assess spontaneous maxillary
[21] Jenin, Palestine study FPM) space closure spontaneous space
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
closure
Teo et Dental Hospital, 2010 Cross-sectional, 66 subjects NA Mean age 11–17 At extraction time: 54/94 (57.4%) NA NA
al., 2015 London, UK hospital-based 94 (T) 9.2 years (mean Panoramic X-ray to mandibular
[17] (mandibular 13.8) years assess Demirjian’s de- spontaneous space
FPM) (71 velopmental stages closure$
SPM at of SPM Stage E**: 41/71
stage E** (58%) mandibular
Page 5 of 15
Table 1 Characteristics and outcomes of included studies (Continued)
Reference Site/Country Duration Study design Sample size Age at Age at Method of Findings P-value or
time of time of assessment OR and CI
Extraction Non- Extraction group Non-extraction
extraction evaluation
group extraction group
group
and 23 at At recall: clinical spontaneous space
stage F**) examination with closure$
periodontal probe Stage F**: 13/23
placed occlusally (56.5%) mandibular
between each tooth spontaneous space
distal to the canine closure$
to assess space
closure
Saber et al. BMC Oral Health (2018) 18:59
Effect on third molar development and eruption
Ay et al., Department of Oral 1997– Cross-sectional, 107 subjects 107 subjects < 16 years 18–40 (Comparison of 77/107 (72%) third 20/107 (18.7%) Difference
2006 and Maxillofacial 2004 hospital-based (unilateral 107 (T) (mean extraction and non- molars in Class I third molars in between
[13] Surgery, Cumhuriyet extraction of 25.69) extraction sides in ramus relationship# Class I ramus extraction
University, Sivas, mandibular years the same patient) 82/107 (76.6%) relationship# and non-
Turkey FPM) 107 (T) Panoramic X-ray to Class A impaction 50/107 (46.7%) extraction
assess state of im- depths^78/107 Class A impaction group
paction and impac- (81.3%) in vertical depths^37/107 P < .001*
tion depth of third positions (34.6%) in vertical P < .001*
molars using Pell and positions P < .001*
Gregory classification
and to assess third
molar angulation
Yavuz et Department of NA Cross-sectional 165 (T) 165 165 (T)165 < 12 years 13–18 Panoramic X-ray to 28/165 (17%) third 11/165 (6.6%) third P<
al., 2006 Orthodontics, Dental (comparison of subjects subjects (mean assess development molar erupted molar erupted 0.05*OR:
[19] Faculty, Atatürk extraction and 15.35) and eruption of third 2.86*,***CI:
University, Erzurum, non-extraction years molars by measuring 1.37, 5.96
Turkey sides in the same the vertical distances
patient), hospital- between the mesio-
based buccal cusp tips of
the third molar and
occlusal plane
Dental casts to
assess eruption of
third molar when
part of the crown is
piercing the gingival
tissues
Caries and/or filling of adjacent teeth
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Oliver et Schools of South 1981– Cross-sectional, Occlusal384 Occlusal4910 11– 15– Intraoral examination Occlusal Occlusal P < 0.001*
al., 1988 Glamorgan, UK 1984 disproportionate (S) (S) 12 years 16 years to record caries 131/384 (34.1%) 1153/4910 (23.5%) OR:
[15] stratified Proximal Proximal (in 1980) (in 1984) using a two numeric carious Proximal carious 1.64*,***
sampling, 415 (S) 5038 (S) code system: a tooth 33/415 (7.9%) Proximal CI: 1.35,
schools-based description code, carious 771/5038 (15.3%) 2.1*,***
and a surface carious OR: 0.48
description code
Page 6 of 15
Table 1 Characteristics and outcomes of included studies (Continued)
Reference Site/Country Duration Study design Sample size Age at Age at Method of Findings P-value or
time of time of assessment OR and CI
Extraction Non- Extraction group Non-extraction
extraction evaluation
group extraction group
group
Bitewings to CI: 0.33,
supplement the 0.69
clinical diagnosis of
proximal caries
Effects on incisors
Private clinics NA Case-control 34 (P) 34 (P) ≥11 years* Non- Analysis of lateral 1.NB (mean 23.2o) 1.NB (mean 28.4o) P = 0.004*
Normando (matched for (bilateral extraction: cephalometric X-rays lingual tipping lingual tipping
and gender and age) extraction of 16– from routine
Saber et al. BMC Oral Health (2018) 18:59
Cavacami, mandibular 26.2 years orthodontic
2010 [20] FPM) Extraction records
16–
36 years
Effects on skeletal development
Private sector NA Case-control 34 subjects 34 subjects ≥11 years* Non Analysis of lateral Mean GnSN 65.2o Mean GnSN 67.2o P = 0.05*
Normando (matched for (bilateral extraction: cephalometric X-rays Counter-clockwise Counter-clockwise P = 0.0001*
and gender and age) extraction of 16– from routine rotation of occlusal rotation of the P = 0.048*
Cavacami, mandibular 26.2 years orthodontic plane (mean 5.6o) occlusal plane
2010 [20] FPM) Extraction records Lower anterior face (mean 12.6o)
16– height (mean Lower anterior face
36 years 68.6 mm) height (mean
70.8 mm)
Notes: (−), decrease in value; *statistically significant (P ≤ 0.05); **according to Demirjian: stage E of dental development indicates early bifurcation development, stage F indicates late bifurcation development; ***this
value was calculated by the authors according to the numbers mentioned in the study; #according to Pell and Gregory classification of state of impaction in relation to the ramus, class I described as the crown is near
the anterior border of the ramus; ^according to the Pell and Gregory classification of depth of impaction, class A described as the occlusal surface of the impacted tooth being level or nearly level with the second
molar; $described by the author as having contact-point displacements less than 1 mm
Abbreviations: S surfaces of teeth, T teeth, FPM first permanent molar, SPM second permanent molar, OR odds ratio, CI confidence interval, 1.NB. lower incisor to nasion-B-point angle, GnSN gnathion to sella-nasion
angle, NA value not applicable
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Page 7 of 15
Saber et al. BMC Oral Health (2018) 18:59 Page 8 of 15
radiographs. The FPM was extracted at a mean patient age Rahhal [12, 21] studied the timing of extraction of
of 10.5 years. The investigators measured the angles severely decayed upper FPMs. In his sample of children
between the long access of the SPM or second premolar (mean age 10.5 years) who underwent extraction of an
and Frankfort horizontal plane in the maxilla and the upper FPM, Rahhal found that 84.6% of upper SPMs
occlusal plane in the mandible. They also measured the dis- had complete space closure without any orthodontic
tances between the distal surface of the upper SPM or sec- intervention and only 15.4% of upper SPMs erupted
ond premolar and the pterygomaxillary fissure in the 1 mm distal to the second premolar.
maxilla and the distance between the lower SPM or second In a more recent study, Teo et al. [17] reported on space
premolar and the ramus of the mandible. They reported closure in a group of children of mean age 9.2 years at the
that the FPM extraction space was closed mostly by the time of extraction. They studied three confounding radio-
SPM rather than by the second premolar. SPM angles and graphic factors related to early lower FPM extraction and
distances increased by 15.65° and 0.18 mm, respectively, in its relationship to space closure (Table 1). The three fac-
the maxilla and by 4.62° and 3.83 mm in the mandible, tors were: “1, the second premolar is engaged in the bifur-
while second premolar angles and distances decreased by 5. cation of the second primary molar; 2, the SPM is mesially
68° and 2.58 mm in the maxilla and 4.63° and 1.82 mm in angulated in relation to the FPM; and 3, presence of the
the mandible when compared with the angles and distances third molar”. The presence of all three factors was associ-
before extraction. The results also showed a significant ated with significantly better space closure (P < 0.001), and
change in the means of all angles and distances on the ex- a combination of the second and third factors resulted in
traction side after one year compared with readings at the the most favorable outcomes (P < 0.001).
time of extraction (P < 0.05). This comparison was per- A meta-analysis was performed for the three studies
formed by superimposition of lateral cephalometric [14, 16, 18] that reported space closure in both arches
radiographs. However, no statistically significant dif- separately to compare the frequency of spontaneous
ference in any of the readings was found on the non- space closure of the SPM in the maxilla with that in the
extraction side (P > 0.05) [7]. mandible. Space closure was more likely to occur in the
Jälevik and Möller [14] investigated the effect of extrac- maxilla than in the mandible, but the difference was not
tion of hypomineralized FPMs in a group of children aged statistically significant (odds ratio 2.06, 95% confidence
5.6–12.7 years. They found that the overall rate of space interval 0.46–9.28; P = 0.35). The heterogeneity between
closure was 85.2%. This higher rate was more frequent in the three studies was moderate (I2 = 72%) and
the maxilla (81.6%) than in the mandible (75%), but the statistically significant (P = 0.03). One study found that
difference was not statistically significant (P = 0.518). space closure was significantly greater in the maxilla
Rãducanu et al. [16] reported that post-extraction mi- than in the mandible (94% and 66%, respectively; P = 0.
gration occurred in the following ways: over-eruption of 0001) [18]. The second study also found that space
opposing teeth, horizontal migration of neighboring closure was greater in the maxilla than in the mandible
teeth, space reduced by tipping, dual drift (horizontal (81.6% and 75%, respectively) but the difference was not
and vertical), or complete space closure. The age at statistically significant (P = 0.518) [14]. In contrast, the
which FPM extraction was performed had a significant third study found that space closure was significantly
influence on the post-extraction space in both the maxil- greater in the mandible than in the maxilla (50% and 33.
lary (P = 0.02) and mandibular (P < 0.001) arches. The 3%, respectively; P = 0.024) [16]. All these results were
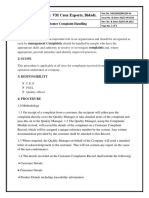
results of this research confirmed that spontaneous illustrated in a forest plot (Fig. 2).
space closure does not occur in children who undergo
FPM extraction after the age of 11 years. The authors re- Effect on development and eruption of the second
ported that the rate of space closure in the mandible permanent molar
(50%) was significantly greater than that in the maxilla A paper by Telli and Aytan [7] discussed the effect of
(33.3%; P = 0.024). FPM extraction on the development and eruption of the
Teo et al. [18] evaluated spontaneous space closure after SPM. They observed that root closure and eruption of
FPM extraction in children aged 7–13 years. They classified the SPM were accelerated on the extraction side when
space closure into five categories. The first category was compared with the non-extraction side according to
complete space closure between the contact points of the panoramic X-ray (Table 1).
SPM and the second premolar. However, the other four
categories had remaining space ranging from 1 mm to Effect on development and eruption of the third molar
5 mm or/and angulation or rotation of the SPM or second Ay et al. [13] studied the changes in angle and position
premolar. Complete space closure in the upper arch was of the mandibular third molar after unilateral mandibu-
significantly (P < 0.001) more likely to be achieved than in lar FPM extraction in a group of children aged younger
the lower arch (in 94% versus 66% of cases, respectively). than 16 years. They used the Pell and Gregory classification
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 9 of 15
Fig. 2 Forest plot for meta-analysis of the comparison between post extraction space closure in the upper and lower arches
for the third molar in relation to the mandibular ramus was present (15.3%; P < 0.001). However, there was a
and its depth of impaction as measured on panoramic X- significantly greater percentage of decayed and/or
ray [22]. This classification was described as follows: “Class filled occlusal surfaces in the adjacent SPM and pre-
I, the crown is near the anterior border of the mandibular molars in the arches with an extracted FPM (34.1%)
ramus; Class II, the crown is one-half covered by the when compared with arches in which the FPM was
ramus; Class III, the crown is completely within the man- present (23.5%; P < 0.001; Table 1).
dibular ramus” (Additional file 2) and as “Class A, the oc-
clusal surface of the impacted tooth is level or nearly level
with the SPM; Class B, the occlusal surface is between the Effects on incisors
occlusal plane and the cervical line of the SPM; Class C, Normando and Cavacami [20] discussed the effects of
the occlusal surface is below the cervical line of the second FPM extraction on the incisors in subjects aged approxi-
molar” (Additional file 3). Angulation of the third molar mately 11 years. Bilateral loss of the lower FPM resulted
was measured between the occlusal plane of the first and in pronounced lingual tipping (P = 0.004) and retrusion
second premolars and the occlusal surface of the third (P = 0.03) of the mandibular incisors. However, there
molar. The angles were classified as follows: vertical, < 11°; was no pronounced effect on inclination of the maxillary
mesioangular or distoangular, 11°–70°; and horizontal, > incisors or their anteroposterior position (Table 1).
70°. Ay et al. found that 72% of third molars on the extrac-
tion side had their crowns near the anterior border of the
mandibular ramus versus 18.7% on the non-extraction Effects on skeletal development
side. In addition, 76.6% of third molars on the extraction Normando and Cavacami [20] also discussed the ef-
side had their occlusal surfaces at or near the level of the fects of FPM extraction on the skeleton. A decrease
SPM compared with 46.7% on the non-extraction side. in the gnathion to sella-nasion angle, (i.e., the point
They also found that 81.3% of third molars were in a verti- indicating anteroinferior growth of the mandible) (P =
cal position on the extraction side versus 34.6% on the 0.05), counter clockwise rotation of the occlusal plane
non-extraction side. These results indicate that third mo- (P = 0.0003), and a mild decrease in lower anterior
lars on the extraction side underwent accelerated eruption face height (P = 0.048) occurred as a result of bilateral
when compared with the non-extraction side. The differ- loss of the lower FPM. There was no significant effect
ence between the extraction and non-extraction sides was on the maxillomandibular relationship in the antero-
consistently statistically significant (P < 0.001) [13]. posterior direction (Table 1).
Yavuz et al. [19] studied the effects of early FPM ex-
traction (before the age of 12 years) on development and
eruption of the third molar in adolescents with mean Ideal time for FPM extraction
age of 15.35 years. They reported that 17% of third mo- Two of the included articles [17, 18] suggested that the
lars had erupted on the extraction side compared with ideal time for FPM extraction is when development is at
only 6.6% of third molars on the contralateral side; the Demerjian stage E [23]. The stages of SPM development
difference was statistically significant (P < 0.05; Table 1). according to Demirjian are: “Stage D crown developed,
Stage E early bifurcation, Stage F late bifurcation, and
Caries and/or filling of adjacent teeth Stage G root development almost complete” [18]. In
Oliver et al. [15] studied the relationship between FPM addition, one of the articles examined spontaneous space
extraction and the prevalence of caries and/or filling of closure for SPMs that were developed to stage E or F.
adjacent teeth. The extractions occurred at the age of The spontaneous space closure rate was found to be
11–12 years. The authors found significantly fewer 58% when the SPM was at stage E and 56.5% when it
decayed and/or filled proximal surfaces in arches with was at stage F. However, the difference was not statisti-
a missing FPM (7.9%) than in arches where the FPM cally significant (P = 1.00) [17].
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 10 of 15
Strengths and limitations of the included articles In one report, the principal indication for extraction of
None of the included studies reported sample size or FPM was extensive caries (70%) followed by hypominer-
power calculations. Only one study clearly described the alization of the molar incisors (11%) [24]. Accordingly,
study design [16]. The setting in which the study was car- in our systematic review, we included studies that ad-
ried out was not reported in two of the articles [7, 12, 20]. dressed the consequences of early extraction of “com-
Six of the studies clearly mentioned patient age at the time promised FPMs”, i.e., FPMs with severe caries or
of extraction and their age when the consequences of ex- hypomineralization.
traction were evaluated. However, two articles did not The studies included in our systematic review showed
mention patient age at the time of extraction [12, 16, 20]. that spontaneous space closure was in the range of 45.
The sequelae were closely related to age at the time of ex- 5%–85.2%. To investigate the reason behind this wide
traction. Two articles [16, 21] did not mention age at the range, we assessed the strengths and limitations of each
time of evaluation of the consequences of extraction. In study. In addition, we subgrouped the samples according
addition, three of the studies did not clearly state their to the site of extraction (maxilla or mandible) and car-
duration of follow-up [19–21]. Two studies did not ried out a meta-analysis to compare them.
undertake case ascertainment in their study participants The highest number of spontaneous space closures was
[16, 20]; however, the other nine studies addressed case reported by Jälevik and Möller [14], who used powerful
ascertainment by intraexaminer or interexaminer repro- methods to assess the eruption of the permanent denti-
ducibility or by using precise methods for assessment of tion, and space closure, including panoramic X-rays, bite-
the outcomes. Seven studies were retrospective in design wing X-rays, casts, and photographs. In contrast, the
and extracted information from patient records, which is smallest number was mentioned by Rãducanu et al. [16].
considered a limitation [13, 16–18]. Interexaminer or Their study had the limitations of a small sample size and
intraexaminer reliability tests were performed in all except a wide subject age range, which may have contributed to
three articles [7, 15, 21]. Confounding factors such as age, the low overall space closure rate.
gender, and geographic location were discussed by only Overall, the spontaneous space closure rate ranged
one study [20] that matched patients for age, while four from 33.3% to 94% in the maxilla and from 50% to 75%
studies [14, 16–18] reported the age of their patients but in the mandible. The smallest space closure (33.3%) in
did not match them in this regard. On the other hand, the maxilla was reported by Rãducanu et al. [16]. As
two studies [7, 15, 21] included age in their inclusion cri- mentioned above, that study had the limitations of a
teria. Finally, only one study reported and analyzed radio- small sample size and subjects who varied widely in age,
graphic factors, which comprised: the second premolar which may explain their low space closure rate for the
being engaged in the bifurcation of the second primary maxilla. On the other hand, the largest space closure
molar; the SPM being mesially angulated in relation to the (94%) for the maxilla was reported by Teo et al. [18].
FPM; and the third molar being present [17] (Table 2). These investigators included a larger sample size and pa-
Scoring of the included articles was done according to tients with SPMs at the early root bifurcation stage,
the STROBE checklist. All of the articles had moderate which could explain their high space closure rate for the
strength except for two [12, 21] that were found to have maxilla. Notably, we did not compare rates of post ex-
weak strength. All the included studies were Category traction space closure at other stages of root formation
III, i.e., yielded evidence obtained from nonexperimental because the data needed to do this were missing.
descriptive studies, such as comparative studies, correl- In the recent study by Teo et al. [17], performed in
ation studies, cohort studies, and case-control studies, 2015, the three aforementioned confounding radiographic
according to the system devised by Shekelle et al. to factors that could affect post extraction space closure were
grade evidence [11]. In addition, all articles were scored analyzed from panoramic radiographs. The presence of
as Class C, based on category III evidence according to these factors was associated with significantly better space
the method used by Shekelle et al. to classify the closure. The combination of a mesially angulated SPM in
strength of the recommendations (Table 3). relation to the FPM and the presence of the third molar
resulted in the most favorable outcomes. Eichenberger et
Discussion al. [25] also agreed that the presence of third molars might
Our systematic review included eleven articles that have a positive effect on spontaneous space closure in the
fulfilled our inclusion criteria. These papers discussed mandible. However, these studies were performed only for
several dental and skeletal consequences related to the mandibular arch, so the maxilla and mandible could
early extraction of compromised FPM. A meta- not be compared.
analysis was carried out to compare the differences in Regarding patient age at the time of extraction, Rãdu-
spontaneous space closure between the upper and canu et al. [16] reported that FPM extractions were per-
lower arches post extraction. formed after the age of 11 years in most children and
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 11 of 15
Table 2 Strengths and limitations of included studies according to the STROBE checklist
Reference Strengths Limitations Scores
Ast et al., 1961 [12] • Clear objectives • Cross-sectional study with convenience sample 5*
• Ascertainment of outcome and reliability of examiners • The study design was not mentioned
were described • The sample size and power of the sample was not
• Extraction and non-extraction groups were matched for calculated
age • The study setting was not clear
• Retrospective study
• Age at time of extraction was not mentioned
• Potential confounders and participant characteristics
were not described
• Weak methodology (method of assessment of molar
relationship was not uniform or acceptable)
Oliver et al., 1988 • The objectives were clear • The study design was not mentioned 9**
[15] • The sample was stratified; however, the eligibility criteria • There was no sample size power calculation
for participant selection was not clear • Potential confounders were not addressed
• Age of participants at time of extraction and evaluation of
consequences were clear
• Examination was carried out by one examiner
• Intraexaminer reproducibility was established
• Numbers of participants used for each examination was
mentioned with reasons for withdrawal
Telli and Aytan, • The objectives were clear • The study design was not mentioned 10**
1989 [7] • Age of participants at time of extraction and evaluation of • There was no sample size power calculation
consequences were clear • The location from which the sample was recruited was
• Split-mouth (extraction and non-extraction sides in the not clear
same patient) • Reason for “non-participants” was not mentioned
• Method used to assess variables was powerful
(superimposition of cephalometric radiographs)
Ay et al., 2006 [13] • The objectives were clear • The study design was not mentioned 9**
• The age was clear both at the time of extraction and • Retrospective
evaluation of consequences • The number of extracted teeth was not clear
• The setting was clear (Department of Oral and Maxillofacial • No sample size power calculation was performed
Surgery of Cumhuriyet University, Sivas, Turkey)
• Participant characteristics were mentioned
• The same investigator undertook all measurements, and
the reproducibility of the method was tested
Yavuz et al., 2006 • The objectives were clear • The study design, method for selecting the sample, 11**
[19] • The location of participant recruitment was clear and period of recruitment were not mentioned
• The age was clear both at the time of extraction and • No sample size power calculation
evaluation of consequences • A retrospective study design
• Reliability testing was done • Potential confounders were not addressed
• Extraction and non-extraction sides were in the same • Follow-up duration was not clear
patient
• All assessments were performed by one examiner
• Intraexaminer reproducibility was established
Jälevik and Möller, • The objectives were clear • The study design was not mentioned 11**
2007 [14] • The setting and location of patient recruitment were clear • Period of recruitment was not mentioned
• The age of participants at time of extraction and time of • A cross-sectional study design
evaluation of consequences were clear • No sample size power calculation was performed
• Methods used to assess variables were powerful
(panoramic X-rays, bitewings, casts and photographs)
Rãducanu et al., • The objectives were clear • No sample size power calculation was performed 13**
2009 [16] • The study design was clear • The age at extraction and at evaluation of
• The location and duration of participant recruitment were consequences was not clear
clear • Numbers of each category were not mentioned, only
• Intraexaminer and interexaminer reliability tests were percentages.
performed • Convenience sample
• Retrospective study
• Potential confounders were not addressed
• Small sample size
Normando and • The objectives were clear • The study design was not mentioned 13**
Cavacami, 2010 [20] • Cases and controls were matched for age, gender, and • The sample size power was not calculated
location • The setting in which the study was performed was not
mentioned
• Age at extraction time was not mentioned
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 12 of 15
Table 2 Strengths and limitations of included studies according to the STROBE checklist (Continued)
Reference Strengths Limitations Scores
• Retrospective study from records
• Follow-up time was not clear
Teo et al., 2013 [18] • The objectives were clear • The study design was not mentioned 11**
• The location and duration of participant recruitment were • No sample size power calculation was performed
clear • Retrospective study from records
• All assessments were undertaken by one examiner
• Intraexaminer repeatability was done
Rahhal, 2014 [21] • The objectives were clear • Study design was not mentioned 6*
• The setting was clear (Arab-American University Clinic, • The sample size power was not calculated
Jenin, Palestine) • Age at evaluation of consequences was not
• Confirmed eligible sample mentioned
• Study only performed at the upper arch
• No controls
• Follow-up duration was not clear
Teo et al., 2015 [17] • The objectives were clear • The study design was not mentioned 14**
• The setting was clear (Dental Hospital, London, UK) • No sample size power calculation was performed
• The age was clear both at the time of extraction and • Retrospective study design
evaluation of consequences
• Intraexaminer reliability was done
Notes: *Scores from 1 to 7 (weak strength); **scores from 8 to 15 (moderate strength)
Abbreviation: STROBE Strengthening the Reporting of Observational Studies in Epidemiology
spontaneous post extraction space closure was rarely space closure. In addition, they did not report on how
achieved [16]. Albadri et al. [24] reported similar find- many patients achieved complete closure or the standard
ings, in which children who underwent FPM extractions deviation of the mean distance and angulation, so we
were older than the age allowing optimal spontaneous were not able to carry out any further analysis.
space closure. Three studies reported differences in the amount of space
Telli and Aytan [7] investigated linear and angular closure between the maxilla and the mandible [14, 16, 18]
measurements using lateral cephalometric radiographs and were subjected to meta-analysis. Jälevik and Möller
and reported that the FPM extraction space was closed [14] and Teo et al. [18] reached the same conclusion i.e.,
mostly by the SPM rather than by the second premolar. that space closure after extraction of a compromised FPM
These authors also found a statistically significant was better in the maxilla than in the mandible. However,
change in the means of all angles and distances on the only Teo et al. [18] showed a significant difference between
extraction side after one year when compared with read- the maxilla and the mandible [18]. In contrast, another
ings at the time of extraction. However, they did not study reported that complete space closure was more likely
compare this outcome with the distance needed for to be achieved in the mandible than in the maxilla [16].
Table 3 Category of evidence and strength of recommendation
Topic Recommendation Category of Strength of
evidence recommendation
Effects on post extraction space Early extraction of compromised FPM leads to decrease in post extraction III*** C^
space
Effect on development and Early extraction of compromised FPM results in accelerated development and III*** C^
eruption of SPM eruption of SPM
Effect on development and Early extraction of compromised FPM results in accelerated development and III*** C^
eruption of third molar eruption of third molar
Caries and/or filling of adjacent Early extraction of compromised FPM causes a decrease in caries and/or III*** C^
teeth fillings of proximal surfaces on adjacent teeth
Effects on incisors Early extraction of compromised FPM results in lingual tipping and retrusion III*** C^
of lower incisors
Effects on skeletal development Early extraction of compromised FPM results in counterclockwise rotation of III*** C^
the occlusal plane
Notes: ***According to the system devised by Shekelle et al. [13] to grade evidence, Category III is evidence from nonexperimental descriptive studies, such as
comparative studies, correlation studies, cohort studies, and case-control studies. ^According to the system used for classifying the strength of the recommenda-
tions devised by Shekelle et al. [13], Class C is directly based on category III evidence or a recommendation extrapolated from category I or II evidence
Abbreviations: FPM first permanent molar, SPM second permanent molar
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 13 of 15
The difference in the eruption pathway between the molar eruption and movement into a better position [13].
maxilla and mandible could be the reason that the max- The same investigator made all the measurements, and
illa showed better space closure. The apex of the maxil- the reproducibility of the method was tested, which is
lary SPM is usually mesially placed in relation to the considered a strength of this study. However, the exact
crown, and during spontaneous space closure, the crown number of teeth extracted was not stated.
tends to tip mesially into a more satisfactory position In addition, it was reported that the development and
[26]. However, complete space closure was achieved in eruption of the third molars on the FPM extraction sides
only 66% of cases where the mandibular FPM was ex- were significantly accelerated compared with the contra-
tracted when the SPMs were at the early bifurcation lateral sides, as evaluated by panoramic X-rays and den-
stage. As explained by Gill et al. [5], extraction of the tal casts. The third molars on the extraction sides in 96
mandibular FPM before or after this stage will not result of 131 cases (73.3%) were closer to the occlusal plane
in complete space closure. Extraction before early bifur- than the third molars on the contralateral sides [19]. Gill
cation may result in distal drifting, tilting and rotation of et al. [5] reported similar results, i.e., a 90% chance of
the unerupted second premolar because it lies in an un- successful third molar eruption after FPM extraction
restrained position apical to the roots of the second de- compared with a 55% chance following premolar extrac-
ciduous molar. If the FPM is extracted during or after tion. Most third molars had a tendency to erupt early
eruption of the SPM, complete space closure is usually and establish a good contact relationship with the SPM.
not achieved. This could be due to the occlusal forces According to panoramic X-rays and clinical examin-
that encourage lingual tilting of the SPM, given that the ation, significantly fewer decayed and/or filled prox-
lingual plate is thinner than the buccal plate of alveo- imal surfaces were found in arches with missing
lar bone, which in turn affects the likelihood of FPMs (8% when FPMs were missing and 15% when
complete space closure. they were present). This was due to ease of cleaning,
One study reported that 84.6% of maxillary SPMs had accessibility for application of fluoride, and less accu-
complete space closure without any orthodontic inter- mulation of plaque. In contrast, significantly more
vention; however, this study had some limitations, in- decayed and/or filled occlusal surfaces were found in
cluding no mention of the age at evaluation of arches with FPM extraction in the adjacent SPMs and
consequences, lack of controls, and an unclear follow-up premolar teeth than arches in which the FPM was
duration [21]. Therefore, we cannot rely on these results; present (34% and 24%, respectively). SPMs had more
in addition, the study was performed only on the max- carious or restored occlusal surfaces than second pre-
illa, so a comparison between the maxilla and the man- molars [15]. Extraction of FPM is not the main etio-
dible cannot be made. logical factor for the development of occlusal caries.
One article discussed the effect of extraction of the However, children requiring FPM extraction were at
FPM on the development and eruption of the SPM. On higher risk for developing occlusal decay in all teeth.
analysis of panoramic X-rays, the authors found that Using cephalometric measurements, Normando and
root closure and eruption of SPM were accelerated on Cavacami [20] found that pronounced lingual tipping
the extraction side when compared with the non- and retrusion of the mandibular incisors had resulted
extraction side [7]. However, these results were not sub- from bilateral loss of the lower FPM. While there was
jected to statistical analysis, which is considered a weak- no pronounced effect on the inclination of the maxillary
ness of this study. Further studies are needed to confirm incisors nor their anteroposterior position due to bilat-
these findings. eral extraction of the lower FPM [20]. Extraction of the
The prevalence of third molar impaction worldwide lower FPM results in increased overbite and overjet due
has been reported to be 24.40% [27]. Further, in 2016, to lingual inclination of the lower incisors [30].
Hatem et al. [28] reported that 70% of third molars were After comparing lateral cephalometric measurements
classified as impacted. Al-Anqudi et al. [29] found that between a control group and a group with bilateral loss
54.3% of patients had at least one impacted third molar. of the FPM, Normando and Cavacami [20] reported sev-
Therefore, extracting posterior teeth can increase the eral findings. A decrease in the gnathion to sella-nasion
eruption space for third molars by mesial movement of angle, counter clockwise rotation of the occlusal plane,
the molars [13]. Third molars observed on the extraction and a mild decrease in lower anterior face height oc-
side were closer to the anterior border of the mandibular curred as a result of bilateral loss of the lower FPM.
ramus, the occlusal surface was level or nearly level with These findings were due to the common clinical observa-
the SPM, and more vertically positioned when compared tion of loss of the vertical dimension resulting from bilateral
with the non-extraction side, which indicates acceleration loss of the FPM. No significant effect was found with regard
of third molar eruption. This is due to the fact that man- to the maxillomandibular relationship in the anteroposter-
dibular FPM extraction increased the space for third ior direction analyzed using different linear and angular
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 14 of 15
measurements. Notably, the mandible was more affected caries in children would avoid these consequences. Where
than the maxilla, with regard to both effects on the incisors extraction of the FPM is unavoidable, the ideal time to ex-
and effects on skeletal development [20]. Nevertheless, this tract should be taken into consideration using the Demir-
report did not mention the ages at which FPMs were ex- jian classification for development of the SPM rather than
tracted, the duration of follow-up, nor the study setting, so by chronological age. The ideal time for FPM extraction;
its findings need further clarification. with fewer undesirable consequences, is when the SPM is
Malocclusion is a well-known problem that could at Demirjian stage E (early bifurcation). The decision to ex-
affect the developing dentition following premature loss tract a FPM in the mandible is more difficult than for one
of primary or permanent teeth [31]. Malocclusion pre- in the maxilla, because the sequelae relate more to the
sents a health issue, as it might negatively influence the mandible than to the maxilla. It appears that the studies in-
quality of life of young patients [32]. Ast et al. [12] cluded in this review have too many weaknesses to draw
claimed that malocclusion was more common in the sufficient evidence. Therefore, further longitudinal studies
FPM extraction group (97%) than in the non-extraction are needed to investigate the influence of age and sex on
group (70%), suggesting that malocclusion could result time of extraction and to compare the consequences of ex-
from early tooth extraction. They also found that ingestion traction with those of other treatment modalities in order
of fluoridated water from birth onwards in children re- to arrive at a decision on how to proceed in these patients.
sulted in significant protection against dental caries, and Finally, confirmation of previous outcomes should be con-
significantly lower rates of loss of permanent teeth, specif- sidered, and other variables that could influence the out-
ically FPMs, and consequently less malocclusion when come should be tested in longitudinal studies.
compared with children who did not ingest fluoridated
water at the optimum concentration [12]. Notably, this Additional files
retrospective study did not mention the design, setting, or
the ages at which FPMs were extracted. In addition, the Additional file 1 Scheme devised by Shekelle et al. for classifying the
method used to address malocclusion was not described evidence for and strength of study recommendations. (DOCX 192 kb)
and the method used to assess the molar relationship was Additional file 2 Pell and Gregory classification of third molar in relation
neither uniform nor acceptable. Therefore, the results of to the mandibular ramus. Class I: the crown is near the anterior border of
the mandibular ramus. Class II: the crown is one-half covered by the
this study cannot be considered reliable. ramus. Class III: the crown is completely within the mandibular ramus.
The ideal time for FPM extraction is when the SPM is (DOCX 104 kb)
at the early bifurcation stage. According to our systematic Additional file 3 Pell and Gregory classification according to impaction
review, extraction of compromised FPM has three seque- depth of third molar. Class A: the occlusal surface of the impacted tooth
is level or nearly level with the second molar. Class B: the occlusal surface
lae, i.e., space changes, effects on the incisors, and effects is between the occlusal plane and the cervical line of the second molar.
on skeletal development. These sequelae are more related Class C: the occlusal surface is below the cervical line of the second
to the mandible than to the maxilla [14, 18, 20]. Spontan- molar. (DOCX 97 kb)
eous space closure was more difficult to achieve in the
mandible than in the maxilla [14, 18]. Lingual tipping and Abbreviations
retrusion of the lower incisors and a mild decrease in ADA: American Dental Association; CI: Confidence interval; FPM: First
permanent molar; GnSN: Gnathion to sella-nasion angle; NA: Value not
lower anterior face height were also reported [20]. As a re- applicable; NB: Lower incisor to nasion-B-point angle; OR: Odds ratio;
sult, the decision to extract the FPM is more critical in the S: Surfaces of teeth; SPM: Second permanent molar; STROBE: Strengthening
mandible than in the maxilla. Nevertheless, we do not the Reporting of Observational Studies in Epidemiology; T: Teeth;
WHO: World Health Organisation
hesitate to extract in the maxilla.
Our systematic review has some limitations. The in- Acknowledgements
cluded studies were observational (cross-sectional and The authors of this review declare no conflicts of interest. Ethical approval
case-control) and seven were retrospective. There is a also was not required for our review. Authors would like to acknowledge
King Abdulaziz University Deanships of Postgraduate Study and Scientific
need for prospective studies to confirm the consequences Research since the work is a part of fulfillment of Master Degree of the first
of FPM extraction. Other variables that affect the conse- three authors. The authors also would like to thank Dr. Doaa El Derwi for her
quences of FPM extraction should also be tested. help in obtaining some of the statistical information. In addition, we would
like to thank Editage (www.editage.com) for English language editing.
This research did not receive any specific grant from funding agencies in the
Conclusions and recommendations public, commercial, or not-for-profit sectors.
The outcomes of early extraction of FPM include a de-
crease in post extraction space, accelerated development Funding
This research did not receive any specific grant from funding agencies in the
and eruption of the SPM and third molar, a decrease in public, commercial, or not-for-profit sectors.
caries and/or fillings on proximal surfaces of adjacent
teeth, lingual tipping and retrusion of incisors, and coun- Availability of data and materials
ter clockwise rotation of the occlusal plane. Prevention of Not applicable.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Saber et al. BMC Oral Health (2018) 18:59 Page 15 of 15
Authors’ contributions 16. Rãducanu AFV, Herteliu C, Rãducanu M. Prevalence of loss of permanent
Literature search, study selection, eligibility criteria, data extraction and first molars in a group of Romanian children and adolescents. Oral Health
manuscript writing were conducted by the three authors (AMS, DHA, MFH) Dent Manag. 2009;8(3):3–10.
equally. AAE: provided the research idea, participated in the design, and 17. Teo TK, Ashley PF, Derrick D. Lower first permanent molars: developing better
critically reviewed the manuscript. NMA critically reviewed the manuscript. predictors of spontaneous space closure. Eur J Orthod. 2015;38(1):90–5.
HS reviewed data extraction and manuscript writing. All authors have read 18. Teo TK, Ashley PF, Parekh S, Noar J. The evaluation of spontaneous space
and approved the final manuscript. closure after the extraction of first permanent molars. Eur Arch Paediatr
Dent. 2013;14(4):207–12.
Ethics approval and consent to participate 19. Yavuz I, Baydas B, Ikbal A, Dagsuyu IM, Ceylan I. Effects of early loss of
Not applicable. permanent first molars on the development of third molars. Am J Orthod
Dentofac Orthop. 2006;130(5):634–8.
Consent for publication 20. Normando D, Cavacami C. The influence of bilateral lower first permanent
Not applicable. molar loss on dentofacial morfology – a cephalometric study. Dental Press J
Orthod. 2010;15(6):100–6.
Competing interests 21. Rahhal A. Extraction timing of heavily destructed upper first permanent
The authors declare that they have no competing interests. molars. Czas Stomatol. 2014;4(3):161–8.
22. Pell GJ, Gregory GT. Impacted mandibular third molars: classification and
modified technique for removal. Dent Digest. 1933;39(9):330–88.
Publisher’s Note 23. Demirjian A, Goldstein H, Tanner JM. A new system of dental age
Springer Nature remains neutral with regard to jurisdictional claims in assessment. Hum Biol. 1973;45(2):211–27.
published maps and institutional affiliations. 24. Albadri S, Zaitoun H, McDonnell ST, Davidson LE. Extraction of first
permanent molar teeth: results from three dental hospitals. Br Dent J. 2007;
Author details 203(7):E14. discussion 408-9
1
Pediatric Dentistry Department, Faculty of Dentistry, King Abdulaziz 25. Eichenberger M, Erb J, Zwahlen M, Schatzle M. The timing of extraction of
University, P.O. Box 80209, Jeddah 21589, Saudi Arabia. 2Pediatric Dentistry non-restorable first permanent molars: a systematic review. Eur J Paediatr
Department, Faculty of Dentistry, Alexandria University, Alexandria, Egypt. Dent. 2015;16(4):272–8.
26. Crabb JJ, Rock WP. Treatment planning in relation to the first permanent
Received: 27 November 2016 Accepted: 19 March 2018 molar. Br Dent J. 1971;131(9):396–401.
27. Carter K, Worthington S. Predictors of third molar impaction: a systematic
review and meta-analysis. J Dent Res. 2016;95(3):267–76.
References 28. Hatem M, Bugaighis I, Taher EM. Pattern of third molar impaction in Libyan
1. Ozdemir D. Dental Caries : The most common disease worldwide and population: a retrospective radiographic study. Saudi J Dent Res. 2016;7(1):7–12.
preventive strategies. Int J Biol. 2013;5(4):55–61. 29. Al-Anqudi SM, Al-Sudairy S, Al-Hosni A, Al-Maniri A. Prevalence and pattern
2. World Health Organization (WHO). Oral Health. World Health Organization. of third molar impaction: a retrospective study of radiographs in Oman.
2012 [Available from: http://www.who.int/mediacentre/factsheets/fs318/en/ Sultan Qaboos Univ Med J. 2014;14(3):e388–92.
[Accessed 15-2-2016 2016]. 30. Abu Aihaija ES, McSheny PF, Richardson AA. Cephalometric study of the
3. American Dental Association (ADA). Tooth eruption. J Am Dent Assoc. 2006 effect of extraction of lower first permanent molars. J Clin Pediatr Dent.
[Available from: http://www.ada.org/~/media/ADA/Publications/Files/ 2000;24(3):195–8.
patient_58.ashx [Accessed 15–2-2016 2016]. 31. Tinanoff N. Malocclusion. In: Kliegman RM, Behrman RE, Jenson HB, Stanton
4. ElSheikh M, Ali A. Planned extraction of first permanent molars during BF, editors. Nelson textbook of pediatrics. 19th ed. Philadelphia: Saunders
late childhood: a clinical note and mini-review. Dent Oral Craniofac Res. Elsevier; 2011. p. 1252.
2015;1(3):77–80. 32. Dimberg L. Malocclusions and Quality of life. Cross-sectional and
5. Gill DS, Lee RT, Tredwin CJ. Treatment planning for the loss of first longitudinal studies in children. Swed Dent J Suppl. 2015;10(237):1–88.
permanent molars. Dent Update. 2001;28(6):304–8.
6. Ekstrand KR, Christiansen J, Christiansen ME. Time and duration of eruption
of first and second permanent molars: a longitudinal investigation.
Community Dent Oral Epidemiol. 2003;31(5):344–50.
7. Telli AE, Aytan S. Changes in the dental arch due to obligatory early extraction
of first permanent molars. Turk Ortodonti Dergisi. 1989;2(1):138–43.
8. Mantel N, Haenszel W. Statistical aspects of the analysis of data from
retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–48.
9. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in
meta-analyses. BMJ. 2003;327(7414):557–60.
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke
JP. The strengthening the reporting of observational studies in
epidemiology (STROBE) statement: guidelines for reporting observational
studies. J Clin Epidemiol. 2008;61(4):344–9.
11. Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Clinical guidelines: developing
guidelines. BMJ. 1999;318(7183):593–6. Submit your next manuscript to BioMed Central
12. Ast DB, Allaway N, Draker HL. The prevalence of malocclusion, related to and we will help you at every step:
dental caries and lost first permanent molars, in a fluoridated city and a
fluoride-deficient city. Am J Orthod. 1962;48(2):106–13. • We accept pre-submission inquiries
13. Ay S, Agar U, Bicakci AA, Kosger HH. Changes in mandibular third molar • Our selector tool helps you to find the most relevant journal
angle and position after unilateral mandibular first molar extraction. Am J
• We provide round the clock customer support
Orthod Dentofac Orthop. 2006;129(1):36–41.
14. Jalevik B, Moller M. Evaluation of spontaneous space closure and • Convenient online submission
development of permanent dentition after extraction of hypomineralized • Thorough peer review
permanent first molars. Int J Paediatr Dent. 2007;17(5):328–35.
• Inclusion in PubMed and all major indexing services
15. Oliver SJ, Dummer PM, Oliver RG, Hicks R, Addy M, Kingdon A, Shaw WC.
The relationship between loss of first permanent molar teeth and the • Maximum visibility for your research
prevalence of caries and restorations in adjacent teeth: a study of 15-16-
year-old children. J Dent. 1988;16(4):155–9. Submit your manuscript at
www.biomedcentral.com/submit
Content courtesy of Springer Nature, terms of use apply. Rights reserved.
Terms and Conditions
Springer Nature journal content, brought to you courtesy of Springer Nature Customer Service Center GmbH (“Springer Nature”).
Springer Nature supports a reasonable amount of sharing of research papers by authors, subscribers and authorised users (“Users”), for small-
scale personal, non-commercial use provided that all copyright, trade and service marks and other proprietary notices are maintained. By
accessing, sharing, receiving or otherwise using the Springer Nature journal content you agree to these terms of use (“Terms”). For these
purposes, Springer Nature considers academic use (by researchers and students) to be non-commercial.
These Terms are supplementary and will apply in addition to any applicable website terms and conditions, a relevant site licence or a personal
subscription. These Terms will prevail over any conflict or ambiguity with regards to the relevant terms, a site licence or a personal subscription
(to the extent of the conflict or ambiguity only). For Creative Commons-licensed articles, the terms of the Creative Commons license used will
apply.
We collect and use personal data to provide access to the Springer Nature journal content. We may also use these personal data internally within
ResearchGate and Springer Nature and as agreed share it, in an anonymised way, for purposes of tracking, analysis and reporting. We will not
otherwise disclose your personal data outside the ResearchGate or the Springer Nature group of companies unless we have your permission as
detailed in the Privacy Policy.
While Users may use the Springer Nature journal content for small scale, personal non-commercial use, it is important to note that Users may
not:
1. use such content for the purpose of providing other users with access on a regular or large scale basis or as a means to circumvent access
control;
2. use such content where to do so would be considered a criminal or statutory offence in any jurisdiction, or gives rise to civil liability, or is
otherwise unlawful;
3. falsely or misleadingly imply or suggest endorsement, approval , sponsorship, or association unless explicitly agreed to by Springer Nature in
writing;
4. use bots or other automated methods to access the content or redirect messages
5. override any security feature or exclusionary protocol; or
6. share the content in order to create substitute for Springer Nature products or services or a systematic database of Springer Nature journal
content.
In line with the restriction against commercial use, Springer Nature does not permit the creation of a product or service that creates revenue,
royalties, rent or income from our content or its inclusion as part of a paid for service or for other commercial gain. Springer Nature journal
content cannot be used for inter-library loans and librarians may not upload Springer Nature journal content on a large scale into their, or any
other, institutional repository.
These terms of use are reviewed regularly and may be amended at any time. Springer Nature is not obligated to publish any information or
content on this website and may remove it or features or functionality at our sole discretion, at any time with or without notice. Springer Nature
may revoke this licence to you at any time and remove access to any copies of the Springer Nature journal content which have been saved.
To the fullest extent permitted by law, Springer Nature makes no warranties, representations or guarantees to Users, either express or implied
with respect to the Springer nature journal content and all parties disclaim and waive any implied warranties or warranties imposed by law,
including merchantability or fitness for any particular purpose.
Please note that these rights do not automatically extend to content, data or other material published by Springer Nature that may be licensed
from third parties.
If you would like to use or distribute our Springer Nature journal content to a wider audience or on a regular basis or in any other manner not
expressly permitted by these Terms, please contact Springer Nature at
onlineservice@springernature.com
You might also like
- Upper Intermediate: KeynoteDocument3 pagesUpper Intermediate: KeynoteLexieNo ratings yet
- Chapter Sixteen Securities Firms and Investment BanksDocument14 pagesChapter Sixteen Securities Firms and Investment BanksBiloni KadakiaNo ratings yet
- 1 s2.0 S0002817717306918 MainDocument10 pages1 s2.0 S0002817717306918 MainSorour 2No ratings yet
- 2016 Article 320Document8 pages2016 Article 320Milena RamirezNo ratings yet
- s12887 017 0870 4Document8 pagess12887 017 0870 4Gulsana HashmiNo ratings yet
- Laser Pulpotomy - An Effective Alternative To Conventional Techniques - A Systematic Review of Literature and Meta-AnalysisDocument9 pagesLaser Pulpotomy - An Effective Alternative To Conventional Techniques - A Systematic Review of Literature and Meta-AnalysisPatrícia BittencourtNo ratings yet
- Lenzi 2016Document9 pagesLenzi 2016Jhovanny OrozcoNo ratings yet
- Global Distribution of Malocclusion Traits: A Systematic ReviewDocument10 pagesGlobal Distribution of Malocclusion Traits: A Systematic ReviewRoxana OneaNo ratings yet
- Bookshelf NBK401552Document24 pagesBookshelf NBK401552Hanina mamiNo ratings yet
- Novel Methodologies and Technologies To Assess Mid-Palatal Suture Maturation: A Systematic ReviewDocument15 pagesNovel Methodologies and Technologies To Assess Mid-Palatal Suture Maturation: A Systematic ReviewnicoNo ratings yet
- Laser DopplerDocument10 pagesLaser Dopplerodontoedu66No ratings yet
- Guy Huynh-Ba 2018Document15 pagesGuy Huynh-Ba 2018IsmaelNo ratings yet
- Barreras Facilitadores Implementacion LabioDocument9 pagesBarreras Facilitadores Implementacion LabioOpeNo ratings yet
- How To Intervene in The Caries Process: Proximal Caries in Adolescents and Adults - A Systematic Review and Meta-AnalysisDocument14 pagesHow To Intervene in The Caries Process: Proximal Caries in Adolescents and Adults - A Systematic Review and Meta-AnalysisLaura ImreNo ratings yet
- Martini 2021Document17 pagesMartini 2021Matheus JacobinaNo ratings yet
- Al Makhmari, S. A., Kaklamanos, E. G., & Athanasiou, A. E. (2017) - Short-Term and Long-Term Effectiveness of Powered Toothbrushes in Promoting PeriodontalDocument21 pagesAl Makhmari, S. A., Kaklamanos, E. G., & Athanasiou, A. E. (2017) - Short-Term and Long-Term Effectiveness of Powered Toothbrushes in Promoting PeriodontalMarco Antonio García LunaNo ratings yet
- Clinical Practice Guideline Adaptation For Risk-Based Caries Management in 18-55 Year-Old Iranian AdultsDocument14 pagesClinical Practice Guideline Adaptation For Risk-Based Caries Management in 18-55 Year-Old Iranian Adultsjunasa.jjfNo ratings yet
- Schwend Ick e 2016Document12 pagesSchwend Ick e 2016Gawi ChangNo ratings yet
- ALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020Document3 pagesALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020محمد نبيل الدعيس100% (1)
- Multiloop Edgewise Archwire Technique and Denture Frame Analysis: A Systematic ReviewDocument9 pagesMultiloop Edgewise Archwire Technique and Denture Frame Analysis: A Systematic Reviewcarmen espinozaNo ratings yet
- Long-Term Survival and Reasons For Failure in Direct Anterior Composite Restorations - A Systematic ReviewDocument10 pagesLong-Term Survival and Reasons For Failure in Direct Anterior Composite Restorations - A Systematic ReviewArcelino FariasNo ratings yet
- 2016 Comparison of Mineral Trioxide Aggregate and Calcium Hydroxyde For ApexifecationDocument8 pages2016 Comparison of Mineral Trioxide Aggregate and Calcium Hydroxyde For Apexifecationbenlaifaoui.amira.2511No ratings yet
- Comparison of Mineral Trioxide Aggregate and Calcium Hydroxide For Apexification of Immature Permanent Teeth: A Systematic Review and Meta-AnalysisDocument8 pagesComparison of Mineral Trioxide Aggregate and Calcium Hydroxide For Apexification of Immature Permanent Teeth: A Systematic Review and Meta-Analysisdrvivek reddyNo ratings yet
- Schwendicke (2016)Document11 pagesSchwendicke (2016)Alex S. OlivaldoNo ratings yet
- Patzelt Et Al-2014-Clinical Implant Dentistry and Related ResearchDocument20 pagesPatzelt Et Al-2014-Clinical Implant Dentistry and Related ResearchSilvia SolisNo ratings yet
- Clinical and Patient-Related Outcomes of A Tapered Implant System With Switched Platform Conical Abutments: A Private Practice Field TrialDocument4 pagesClinical and Patient-Related Outcomes of A Tapered Implant System With Switched Platform Conical Abutments: A Private Practice Field TrialBagis Emre GulNo ratings yet
- Lin 2018Document14 pagesLin 2018giselaNo ratings yet
- Conscious Sedation For The Management of Dental Anxiety in Third Molar Extraction Surgery: A Systematic ReviewDocument10 pagesConscious Sedation For The Management of Dental Anxiety in Third Molar Extraction Surgery: A Systematic ReviewSinara De Souza LopesNo ratings yet
- The Impact of ICDAS On Occlusal Caries Treatment Recommendations For High Caries Risk Patients: An in Vitro StudyDocument7 pagesThe Impact of ICDAS On Occlusal Caries Treatment Recommendations For High Caries Risk Patients: An in Vitro StudyJulio C. MuñozNo ratings yet
- An Update of Treatment Modalities in Children and AdolescentsDocument26 pagesAn Update of Treatment Modalities in Children and Adolescentsjing.zhao222No ratings yet
- Effects of Rapid Maxillary Expansion On The Midpalatal Suture A Systematic ReviewDocument5 pagesEffects of Rapid Maxillary Expansion On The Midpalatal Suture A Systematic ReviewMariana SantosNo ratings yet
- What Are Patients Expectations of Orthodontic TreDocument9 pagesWhat Are Patients Expectations of Orthodontic TreAly OsmanNo ratings yet
- Effects of Educational Interventions On Oral Hygiene: A Systematic Review and Meta-AnalysisDocument18 pagesEffects of Educational Interventions On Oral Hygiene: A Systematic Review and Meta-AnalysisDennis MejiaNo ratings yet
- Orthodontic Camouflage Versus Orthodontic Orthognathic Surgical Treatment in Borderline Class III Malocclusion: A Systematic ReviewDocument13 pagesOrthodontic Camouflage Versus Orthodontic Orthognathic Surgical Treatment in Borderline Class III Malocclusion: A Systematic ReviewClaudia GallardoNo ratings yet
- Periodontal Effects of Maxillary Expansion in Adults Using Non-Surgical Expanders With Skeletal Anchorage vs. Surgically Assisted Maxillary Expansion. A Systematic ReviewDocument12 pagesPeriodontal Effects of Maxillary Expansion in Adults Using Non-Surgical Expanders With Skeletal Anchorage vs. Surgically Assisted Maxillary Expansion. A Systematic ReviewGabriela Lou GomezNo ratings yet
- Ijcpd 16 478Document5 pagesIjcpd 16 478Shameena KnNo ratings yet
- PROMPT Intervention For Children With Severe SpeecDocument39 pagesPROMPT Intervention For Children With Severe SpeecAtalita AzevedoNo ratings yet
- TL3 8 Garbim2021Document33 pagesTL3 8 Garbim2021bomonnhacongdongNo ratings yet
- Art 2Document45 pagesArt 2Juan José Chacón BalderramaNo ratings yet
- 1 Verweij 2017Document9 pages1 Verweij 2017Dokter Gigi NicholasNo ratings yet
- Seale 2008Document5 pagesSeale 2008PhanQuangHuyNo ratings yet
- Study Protocol Open Access: Bianchi Et Al. BMC Oral Health (2021) 21:167Document7 pagesStudy Protocol Open Access: Bianchi Et Al. BMC Oral Health (2021) 21:167baridinoNo ratings yet
- Mandibular Third Molar Extraction: Perceived Surgical Difficulty in Relation To Professional TrainingDocument12 pagesMandibular Third Molar Extraction: Perceived Surgical Difficulty in Relation To Professional TrainingKemas IrsanNo ratings yet
- Alam Et Al 2023 Craniofacial Characteristics in Crouzon S Syndrome A Systematic Review and Meta AnalysisDocument25 pagesAlam Et Al 2023 Craniofacial Characteristics in Crouzon S Syndrome A Systematic Review and Meta AnalysisOral DentNo ratings yet
- Outcome of Crown and Root Resection: A Systematic Review and Meta-Analysis of The LiteratureDocument14 pagesOutcome of Crown and Root Resection: A Systematic Review and Meta-Analysis of The LiteratureLorenaCastanoGarzonNo ratings yet
- Orthodontic Camouflage Versus Orthodontic Orthognathic SurgicalDocument14 pagesOrthodontic Camouflage Versus Orthodontic Orthognathic SurgicalMAYRA ALEJANDRA BAHAMON TRUJILLONo ratings yet
- The Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-AnalysisDocument7 pagesThe Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-Analysisitsme543210No ratings yet
- Evidence-Based Dentistry. How To Design A Research? A Literature ReviewDocument7 pagesEvidence-Based Dentistry. How To Design A Research? A Literature ReviewNadya ANo ratings yet
- Rehabilitación de Dientes Severamente Desgastados Una Revisión SistemáticaDocument25 pagesRehabilitación de Dientes Severamente Desgastados Una Revisión SistemáticaSamuel Flores CalderonNo ratings yet
- 2018 Article 225Document18 pages2018 Article 225Ngo Viet ThanhNo ratings yet
- Kvaal CBCTDocument7 pagesKvaal CBCTLansky TrimeilanaNo ratings yet
- Adherence in Orthodontic Settings UKDocument7 pagesAdherence in Orthodontic Settings UKmundoeletronico.pfNo ratings yet
- Dental Age Assessment Among Tunisian Children Using The Demirjian MethodDocument5 pagesDental Age Assessment Among Tunisian Children Using The Demirjian MethodMishellKarelisMorochoSegarraNo ratings yet
- Quality Assessment of Systematic Reviews On Alveolar Socket Preservation.Document9 pagesQuality Assessment of Systematic Reviews On Alveolar Socket Preservation.andreita_loppNo ratings yet
- Pronostico Nunn Periodontol 2000Document9 pagesPronostico Nunn Periodontol 2000Alejo MoralesNo ratings yet
- The Effect of Pacifier Sucking On Orofacial Structures: A Systematic Literature ReviewDocument11 pagesThe Effect of Pacifier Sucking On Orofacial Structures: A Systematic Literature ReviewAnonymous GbqNxHcNo ratings yet
- NasoalveolarespansionDocument9 pagesNasoalveolarespansionKyke Plazas RománNo ratings yet
- Vonarx 2012Document10 pagesVonarx 2012Laura A. Moraes PintoNo ratings yet
- A Comparison of Four Caries Risk Assessment MethodsDocument13 pagesA Comparison of Four Caries Risk Assessment Methodsovy primaNo ratings yet
- Oday5 PDFDocument8 pagesOday5 PDFOday Abu RomelahNo ratings yet
- Activities 1-5 - BoncalesDocument12 pagesActivities 1-5 - BoncalesBraille Boncales100% (1)
- Battle For The Beetle by Karl Ludvigsen - Chapter One: Birth of A MenaceDocument40 pagesBattle For The Beetle by Karl Ludvigsen - Chapter One: Birth of A MenaceBentley PublishersNo ratings yet
- An Agent-Based Dynamic Occupancy Schedule Model For Prediction of HVAC Energy Demand in An Airport Terminal BuildingDocument10 pagesAn Agent-Based Dynamic Occupancy Schedule Model For Prediction of HVAC Energy Demand in An Airport Terminal BuildingKapil SinhaNo ratings yet
- Industrial Hygiene 101Document25 pagesIndustrial Hygiene 101Ultrapure AnalytichemNo ratings yet
- Socorro Sepulveda LawasDocument2 pagesSocorro Sepulveda LawasBuen LibetarioNo ratings yet
- Building Materials PortfolioDocument75 pagesBuilding Materials PortfolioMikaela Marie GilleraNo ratings yet
- Chapter 14 TestDocument4 pagesChapter 14 TestLeela ZeroNo ratings yet
- Measurement Tire Tread Depth Triangularization PDFDocument4 pagesMeasurement Tire Tread Depth Triangularization PDFTrung Hoàng100% (1)
- Safety and Health Protection On The JobDocument1 pageSafety and Health Protection On The JobCPSSTNo ratings yet
- Energy Auditing Proposal Scope of WorkDocument19 pagesEnergy Auditing Proposal Scope of WorkOmar Bilal AkashNo ratings yet
- The Expansion of Economic GlobalizationDocument15 pagesThe Expansion of Economic GlobalizationRachel Demesa BadaguasNo ratings yet
- Women EntrepreneursDocument27 pagesWomen Entrepreneursurvashirthr86No ratings yet
- Architectural Standards Product Data Sheet: Washbasins N13: Sanitaryware N13/335Document2 pagesArchitectural Standards Product Data Sheet: Washbasins N13: Sanitaryware N13/335Nay Win MaungNo ratings yet
- Prowessiq Data Dictionary PDFDocument5,313 pagesProwessiq Data Dictionary PDFUtkarsh SinhaNo ratings yet
- Fuld & Company - JD Business and Strategic ResearchDocument2 pagesFuld & Company - JD Business and Strategic ResearchShivangi Gupta Student, Jaipuria LucknowNo ratings yet
- Braking of Ceramic DiscDocument15 pagesBraking of Ceramic DiscTushar GoranaNo ratings yet
- Sss Requirements and ProcessDocument3 pagesSss Requirements and ProcessRheu ReyesNo ratings yet
- Managing Sustainability Assessment of Civil Infrastructure Projects Using Work, Nature, and FlowDocument13 pagesManaging Sustainability Assessment of Civil Infrastructure Projects Using Work, Nature, and FlowStevanus FebriantoNo ratings yet
- 10 - Electronics and Communication EngineeringDocument569 pages10 - Electronics and Communication EngineeringRamesh KhatriNo ratings yet
- SOP - Customer CHDocument3 pagesSOP - Customer CHkitekNo ratings yet
- Internal Audit Report FormatDocument3 pagesInternal Audit Report FormatSaket TibrewalNo ratings yet
- Operation and Supply Chain ManagementDocument22 pagesOperation and Supply Chain ManagementJannie LinhNo ratings yet
- Study Habit of The Grade 12 StudentsDocument43 pagesStudy Habit of The Grade 12 StudentsLORENA AMATIAGANo ratings yet
- Internship Report - Nguyễn Trần Phương ThảoDocument25 pagesInternship Report - Nguyễn Trần Phương ThảoThảo PhươngNo ratings yet
- Walt DisneyDocument60 pagesWalt DisneyDemeter LászlóNo ratings yet
- BS en Iso 00062-1999 (2000) PDFDocument20 pagesBS en Iso 00062-1999 (2000) PDFmpica100% (2)
- C4 Smeac 6523Document13 pagesC4 Smeac 6523lawtonjake100% (1)
- Test Bank For Introduction To Global Business Understanding The International Environment Global Business Functions 2nd EditionDocument24 pagesTest Bank For Introduction To Global Business Understanding The International Environment Global Business Functions 2nd EditionChristopherMontgomerycqzp100% (47)