Download as pdf or txt
You might also like
- Motivation LetterDocument1 pageMotivation LetterHendy van Java80% (5)
- E2 Visa Business Plan SampleDocument41 pagesE2 Visa Business Plan SamplecasrsurfNo ratings yet
- The Hospital Team - ReadingDocument2 pagesThe Hospital Team - Readingwuashe59050% (2)
- Medical CertificateDocument2 pagesMedical Certificatejennylynne100% (2)
- NCP Pain HypertensionDocument3 pagesNCP Pain HypertensionEzron Kendrick Duran50% (2)
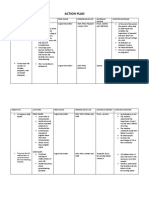
- Action PlanDocument4 pagesAction PlanJosette Mae Atanacio67% (3)
- Sceintific Writing 1Document5 pagesSceintific Writing 1ibrahimNo ratings yet
- Systematic Review and Meta-AnalysisDocument11 pagesSystematic Review and Meta-AnalysisHabtamu WondifrawNo ratings yet
- Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-AnalysisDocument19 pagesGlobal Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-AnalysisAngel ViolaNo ratings yet
- Pone 0100831Document9 pagesPone 0100831ChensoNo ratings yet
- The Natural History Of, and Risk Factors For, Progressive Chronic Kidney Disease (CKD) : The Renal Impairment in Secondary Care (RIISC) Study Rationale and ProtocolDocument16 pagesThe Natural History Of, and Risk Factors For, Progressive Chronic Kidney Disease (CKD) : The Renal Impairment in Secondary Care (RIISC) Study Rationale and Protocolagung neutronNo ratings yet
- Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-AnalysisDocument18 pagesGlobal Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-AnalysisMellya RizkiNo ratings yet
- King ShannonDocument9 pagesKing Shannonarifin hidayatNo ratings yet
- Patient Awareness, Prevalence, and Risk Factors of Chronic Kidney Disease Among Diabetes Mellitus and Hypertensive PatientsDocument9 pagesPatient Awareness, Prevalence, and Risk Factors of Chronic Kidney Disease Among Diabetes Mellitus and Hypertensive Patientsnurul niqmahNo ratings yet
- 2021 Article 2564Document10 pages2021 Article 2564Cinthya Añazco RomeroNo ratings yet
- Shatha Hussain Ali, Et AlDocument9 pagesShatha Hussain Ali, Et AlJeevaNo ratings yet
- Research ArticleDocument10 pagesResearch ArticleAmeldaNo ratings yet
- 2022 Article 1931Document9 pages2022 Article 1931LoganNo ratings yet
- Kaewput 2020Document11 pagesKaewput 2020MarcelliaNo ratings yet
- The Impact of Chronic Kidney Disease On Developed Countries From A Health Economics Perspective: A Systematic Scoping ReviewDocument19 pagesThe Impact of Chronic Kidney Disease On Developed Countries From A Health Economics Perspective: A Systematic Scoping ReviewWalter Espriella CastellarNo ratings yet
- AINES en ERC 2020Document9 pagesAINES en ERC 2020Cesar Augusto Restrepo ValenciaNo ratings yet
- Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis - PMCDocument24 pagesGlobal Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis - PMCtrimardiyanaisyanNo ratings yet
- Prevalence of Comorbidities, Polypharmacy and Drug Related Problems Among Hospitalized Patients With Chronic Kidney DiseaseDocument13 pagesPrevalence of Comorbidities, Polypharmacy and Drug Related Problems Among Hospitalized Patients With Chronic Kidney DiseaseMediterr J Pharm Pharm SciNo ratings yet
- Issm Prisma ChecklistDocument9 pagesIssm Prisma ChecklistInnani Wildania HusnaNo ratings yet
- MousaDocument12 pagesMousaGiriNo ratings yet
- Efficacy of Rituximab Therapy in Children With Nephrotic Syndrome: A 10-Year Experience From An Iranian Pediatric HospitalDocument9 pagesEfficacy of Rituximab Therapy in Children With Nephrotic Syndrome: A 10-Year Experience From An Iranian Pediatric HospitalAris BayuNo ratings yet
- Prevalence of Chronic Kidney Disease in Nigeria Systematic - 052118Document8 pagesPrevalence of Chronic Kidney Disease in Nigeria Systematic - 052118Zainab Abubakar GwanduNo ratings yet
- Application of Creatinine-Based eGFR Equations in Chinese Septuagenarians and OctogenariansDocument12 pagesApplication of Creatinine-Based eGFR Equations in Chinese Septuagenarians and OctogenariansLevi PNo ratings yet
- Long-Term Kidney Function of Childhood Cancer Survivors-Who Needs To Be Monitored?Document4 pagesLong-Term Kidney Function of Childhood Cancer Survivors-Who Needs To Be Monitored?Irawati Eka PutriNo ratings yet
- 2020 Article 1894Document8 pages2020 Article 1894Cleo AlvesNo ratings yet
- Assessment of Diabetes Mellitus Prevalence and Associated Complications Among Patients at Jinja Regional Referral HospitalDocument10 pagesAssessment of Diabetes Mellitus Prevalence and Associated Complications Among Patients at Jinja Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Pharmacoeconomic Evaluation of Hemodialysis Patients: A Study of Cost of IllnessDocument6 pagesPharmacoeconomic Evaluation of Hemodialysis Patients: A Study of Cost of IllnessKhairannisa TrisnaNo ratings yet
- To WordDocument8 pagesTo WordkipobodyNo ratings yet
- Calle, Guillermo Maestro de La, Et Al2017Document7 pagesCalle, Guillermo Maestro de La, Et Al2017priya panaleNo ratings yet
- s12882 021 02319 9Document13 pagess12882 021 02319 9putu juniNo ratings yet
- Clinical Outcome of Donors PDFDocument7 pagesClinical Outcome of Donors PDFEngidaNo ratings yet
- Yilma2020ilma, Daniel, Et Al.2020Document11 pagesYilma2020ilma, Daniel, Et Al.2020priya panaleNo ratings yet
- Impact of Hypertension On Type 2 Diabetes in Mysore Population of South IndiaDocument10 pagesImpact of Hypertension On Type 2 Diabetes in Mysore Population of South Indiagaluh putriNo ratings yet
- Erc Adulto MayorDocument4 pagesErc Adulto MayorMario Ivan De la Cruz LaraNo ratings yet
- Jamainternal Hsu 2020 Oi 200074 1606936160.50628Document8 pagesJamainternal Hsu 2020 Oi 200074 1606936160.50628Kezia AngelinaNo ratings yet
- Upper and Lower Gastrointestinal Bleeding: A Retrospective Study On 10 Years Experiences in Southeastern IranDocument6 pagesUpper and Lower Gastrointestinal Bleeding: A Retrospective Study On 10 Years Experiences in Southeastern IranAlne DanyNo ratings yet
- Self-Management Interventions For Chronic Kidney Disease: A Systematic Review and Meta-AnalysisDocument13 pagesSelf-Management Interventions For Chronic Kidney Disease: A Systematic Review and Meta-AnalysisKikimariaNo ratings yet
- J Egypt Soc Nephrol Transplant203179 1605919 042739Document8 pagesJ Egypt Soc Nephrol Transplant203179 1605919 042739Mina Magdy FahmyNo ratings yet
- Jegh 10 4 344Document7 pagesJegh 10 4 344arifin hidayatNo ratings yet
- Prevalence of Frailty in End Stage Renal DiseaseDocument14 pagesPrevalence of Frailty in End Stage Renal Diseaseor1da2sa3No ratings yet
- ISSN: 2277-4998: Received 20 April 2019 Revised 20 May 2019 Accepted 22 June 2019 Available Online 1 Dec. 2019Document12 pagesISSN: 2277-4998: Received 20 April 2019 Revised 20 May 2019 Accepted 22 June 2019 Available Online 1 Dec. 2019TarigNo ratings yet
- JNursMidwiferySci7294-9611226 024011Document5 pagesJNursMidwiferySci7294-9611226 024011Nurul SaufikaNo ratings yet
- Diabcare 2021 Rwe CKDDocument8 pagesDiabcare 2021 Rwe CKDanderson roberto oliveira de sousaNo ratings yet
- Original Article: Saudi Journal of Kidney Diseases and TransplantationDocument5 pagesOriginal Article: Saudi Journal of Kidney Diseases and TransplantationNiponis ChunchunNo ratings yet
- Prevalence and Risk Factors For ChronicDocument10 pagesPrevalence and Risk Factors For ChronicKhoirul AnamNo ratings yet
- Prevalence of Diabetic Retinopathy in Type II Diabetic Patients in A Health Facility in Karachi, PakistanDocument8 pagesPrevalence of Diabetic Retinopathy in Type II Diabetic Patients in A Health Facility in Karachi, PakistanJaveria RphNo ratings yet
- 10 1111@odi 13236Document10 pages10 1111@odi 13236vero alvarezNo ratings yet
- Impact of Pharmaceutical Care On The Health-RelateDocument14 pagesImpact of Pharmaceutical Care On The Health-RelatealfinadyaNo ratings yet
- 1 s2.0 S1051227616301789 MainDocument7 pages1 s2.0 S1051227616301789 MainResearch OfficeNo ratings yet
- 1 Trinidad y Tobago 2023Document11 pages1 Trinidad y Tobago 2023WENDY PHRITSILA PEÑA TICONANo ratings yet
- Association Between Health LiteraDocument8 pagesAssociation Between Health LiteraberthaNo ratings yet
- Frailty and The Risk of Kidney Function Decline in The Elderly Population: The Rugao Longevity and Ageing StudyDocument8 pagesFrailty and The Risk of Kidney Function Decline in The Elderly Population: The Rugao Longevity and Ageing Studymj.fionaNo ratings yet
- Research Study JournalDocument27 pagesResearch Study JournalHyacinth A RotaNo ratings yet
- Article Info: A B C D e FDocument10 pagesArticle Info: A B C D e FLongwap AbdulNo ratings yet
- Anemia As A Risk Factor in TBDocument15 pagesAnemia As A Risk Factor in TBOlyvia LenseNo ratings yet
- Semaglutide For The Treatment of Non Alcoholic Steatohepatitis Trial Design and Comparison of Non-Invasive BiomarkersDocument9 pagesSemaglutide For The Treatment of Non Alcoholic Steatohepatitis Trial Design and Comparison of Non-Invasive BiomarkersAntonio SalemeNo ratings yet
- CTS MHDDocument8 pagesCTS MHDTheodoreNo ratings yet
- SurvivalDocument7 pagesSurvivalFuad HadiNo ratings yet
- Jcav 13 P 0051Document11 pagesJcav 13 P 0051hasna muhadzibNo ratings yet
- The Clinical Impact of Drug-Induced HepatotoxicityDocument9 pagesThe Clinical Impact of Drug-Induced HepatotoxicityDi LaNo ratings yet
- Precision Medicine Oncology: A PrimerFrom EverandPrecision Medicine Oncology: A PrimerLorna Rodriguez-RodriguezNo ratings yet
- Jcaho 2003 National Patient Safety GoalsDocument13 pagesJcaho 2003 National Patient Safety GoalsJefferson ButalidNo ratings yet
- Circulation Sheet 1K1Document2 pagesCirculation Sheet 1K1Ruth LumibaoNo ratings yet
- Ncp. Oral MucosaDocument1 pageNcp. Oral MucosaZmiaNo ratings yet
- Trends, Legal, EthicalDocument14 pagesTrends, Legal, EthicalGABRIELLE JEANZ AZUMBRADO ACABONo ratings yet
- Best Skincare Clinic in HyderabadDocument5 pagesBest Skincare Clinic in Hyderabadrajitha 0231No ratings yet
- Cefixime For Switch Therapy: Jeremy Hamilton-MillerDocument4 pagesCefixime For Switch Therapy: Jeremy Hamilton-MillerDendy TriatmajaNo ratings yet
- Remedy Responses (LMS)Document1 pageRemedy Responses (LMS)Roger Knight100% (3)
- Nursing Care Plan 601fDocument6 pagesNursing Care Plan 601fEya CamillerNo ratings yet
- Test Bank For Nursing Assistant A Nursing Process Approach 11th EditionDocument7 pagesTest Bank For Nursing Assistant A Nursing Process Approach 11th EditionLarry Cessor100% (32)
- Paramedical Courses in UdaipurDocument6 pagesParamedical Courses in UdaipurAyush Group of EducationNo ratings yet
- Improvement in Quality MetricsDocument10 pagesImprovement in Quality MetricsGodFather xNo ratings yet
- 2e. AAP Tongue Tie FrenotomyDocument2 pages2e. AAP Tongue Tie FrenotomyAprilian Ayu SitaNo ratings yet
- Melanie Daniel Resume 2016Document2 pagesMelanie Daniel Resume 2016api-344304741No ratings yet
- (Draft) Technical Notes SGLG 2023 Health ResponsivenessDocument14 pages(Draft) Technical Notes SGLG 2023 Health ResponsivenessDivina Joy Ventura-Gonzales100% (1)
- DONNING and DOFFINGDocument39 pagesDONNING and DOFFINGCatherine AteradoNo ratings yet
- Nysif PFL Care SeclogoDocument13 pagesNysif PFL Care SeclogoOANo ratings yet
- Request For Proposal (RFP) #4794 Physiotherapy Services: Sponsored by Health PEI - Community Hospitals WestDocument29 pagesRequest For Proposal (RFP) #4794 Physiotherapy Services: Sponsored by Health PEI - Community Hospitals WestDiganta DasNo ratings yet
- Tendernotice 1Document1 pageTendernotice 1sanjay kumarNo ratings yet
- Model Format For Seafarer Employment Agreement PDFDocument6 pagesModel Format For Seafarer Employment Agreement PDFOlehNo ratings yet
- Ommaya Reservoir Drug InfusionDocument19 pagesOmmaya Reservoir Drug InfusionDiah Rahayu SetiawatiNo ratings yet
- Clobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023Document51 pagesClobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023veerraju tvNo ratings yet
- Jagan VaccinationDocument1 pageJagan VaccinationNar JmrNo ratings yet
- 6-Item - KADS - Portuguese - Package Escala de Depressão para AdolescentesDocument4 pages6-Item - KADS - Portuguese - Package Escala de Depressão para Adolescentesmaisalazzarone8652No ratings yet
- CancerpdfDocument3 pagesCancerpdfAbrar KhanNo ratings yet