Download as pdf or txt
You might also like
- Glute Guide 2.0 PDFDocument25 pagesGlute Guide 2.0 PDFAmandaLever100% (13)
- Spring Reset Mel RobbinsDocument26 pagesSpring Reset Mel RobbinsCyberPuro Nica100% (1)
- Urology Complete Qbank PDFDocument58 pagesUrology Complete Qbank PDFPanda Panda100% (1)
- Management of Impacted TeethDocument153 pagesManagement of Impacted TeethToma Irina100% (1)
- Dent Update 2013. Guidelines For The Assessment of The Impacted Maxillary Canine PDFDocument6 pagesDent Update 2013. Guidelines For The Assessment of The Impacted Maxillary Canine PDFDilla Novia AmrilaniNo ratings yet
- Dent Update 2013. Guidelines For The Assessment of The Impacted Maxillary CanineDocument6 pagesDent Update 2013. Guidelines For The Assessment of The Impacted Maxillary CanineWayan Sutresna Yasa100% (1)
- Brighter Futures - Impacted and Ectopic CaninesDocument4 pagesBrighter Futures - Impacted and Ectopic Caninesdr.rhythm sharmaNo ratings yet
- IjodrDocument7 pagesIjodrMuhammad GhifariNo ratings yet
- Canine Impaction A Review of The Prevalence, Etiology, Diagnosis and TreatmentDocument7 pagesCanine Impaction A Review of The Prevalence, Etiology, Diagnosis and TreatmentFadiShihabNo ratings yet
- Management of Impacted Maxillary Canines Using The Kilroy Spring: A Case SeriesDocument7 pagesManagement of Impacted Maxillary Canines Using The Kilroy Spring: A Case SeriesThang Nguyen TienNo ratings yet
- Maxillary Impacted Canines: A Clinical Review: DR Rajiv Yadav, DR Basanta K. ShresthaDocument6 pagesMaxillary Impacted Canines: A Clinical Review: DR Rajiv Yadav, DR Basanta K. Shresthadrzana78No ratings yet
- Exposición Quirúrgica 2020Document10 pagesExposición Quirúrgica 2020Monica JohanaNo ratings yet
- 3 Bishara1992Document13 pages3 Bishara1992Marcos CastroNo ratings yet
- Surgicalexposureof Impactedteeth: Pamela L. AlbertoDocument10 pagesSurgicalexposureof Impactedteeth: Pamela L. AlbertoDANTE DELEGUERYNo ratings yet
- Management of Impacted CanineDocument97 pagesManagement of Impacted CanineOluseye SoyeboNo ratings yet
- Alberto 2020Document10 pagesAlberto 2020ARMADNo ratings yet
- Impacted Maxillary CanineDocument9 pagesImpacted Maxillary CanineVladimir CurcicNo ratings yet
- Diagnosis of Canine ImpactionDocument27 pagesDiagnosis of Canine ImpactionDr.Thrivikhraman KothandaramanNo ratings yet
- Impacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFDocument13 pagesImpacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFPia ContrerasNo ratings yet
- ContempClinDent31123-1436275 035922Document6 pagesContempClinDent31123-1436275 035922Cyriac JohnNo ratings yet
- Bilateral Congenitally Missing Maxillary Canines. A Case ReportDocument4 pagesBilateral Congenitally Missing Maxillary Canines. A Case ReportAmit SagarNo ratings yet
- DT Ce ArticleDocument6 pagesDT Ce ArticleAndrei BusmachiuNo ratings yet
- Orthodontic Management of Buccally Erupted EctopicDocument6 pagesOrthodontic Management of Buccally Erupted EctopicNguyễn Thị Thanh PhươngNo ratings yet
- 7-Maxillary Canine ImpactionDocument8 pages7-Maxillary Canine ImpactionAhmed aljumailiNo ratings yet
- Canine ImpactionDocument10 pagesCanine ImpactionPZ100% (1)
- Canine Impaction-A Review of The Prevalence, Etiology, Diagnosis and TreatmentDocument26 pagesCanine Impaction-A Review of The Prevalence, Etiology, Diagnosis and TreatmentAnil MarnaNo ratings yet
- Examination of Ectopically Ewhpti Canines: Jbnk@Ing, SwedenDocument10 pagesExamination of Ectopically Ewhpti Canines: Jbnk@Ing, SwedenAhmed ElsharkawyNo ratings yet
- Erickson Kurol (CT Study)Document9 pagesErickson Kurol (CT Study)Srishti SyalNo ratings yet
- The Management of Palatally DisplacedDocument13 pagesThe Management of Palatally DisplacedFourthMolar.comNo ratings yet
- Caninos RetenidosDocument14 pagesCaninos RetenidosEduardo SaabNo ratings yet
- CANINE ManagementDocument17 pagesCANINE ManagementSyed Mohammad Osama AhsanNo ratings yet
- Orthodontic Management of Impacted CanineDocument7 pagesOrthodontic Management of Impacted CanineplsssssNo ratings yet
- Sajnani, 2015Document7 pagesSajnani, 2015Julio AbarzuaNo ratings yet
- Caninos TeoriaDocument7 pagesCaninos TeoriaricardoNo ratings yet
- Localization of Impacted Canines: KeywordsDocument4 pagesLocalization of Impacted Canines: KeywordsFelicia HandaliNo ratings yet
- 2003 124 5 509 514 BeckerDocument6 pages2003 124 5 509 514 BeckerFourthMolar.comNo ratings yet
- Etiology of Maxillary Canine Impaction A Review 2Document4 pagesEtiology of Maxillary Canine Impaction A Review 2Rowan HatemNo ratings yet
- 02 - 09 - Studiu Original - Caninul Maxilar InclusDocument8 pages02 - 09 - Studiu Original - Caninul Maxilar InclusSimu MedaNo ratings yet
- 2000 Ericson Resorption of Incisors AfterDocument9 pages2000 Ericson Resorption of Incisors Afterplayer osamaNo ratings yet
- Maxillary Canine-First Premolar TranspositionDocument9 pagesMaxillary Canine-First Premolar TranspositionFabian BarretoNo ratings yet
- Odonto ExoticosDocument14 pagesOdonto ExoticosPedro FontaniveNo ratings yet
- Artigos Anomalias Dentarias PDFDocument154 pagesArtigos Anomalias Dentarias PDFcaalbuquerque07No ratings yet
- Long-Term Results of Orthodontic Treatment of Impacted Maxillary CaninesDocument8 pagesLong-Term Results of Orthodontic Treatment of Impacted Maxillary CaninesAya Dini Oase CaesarNo ratings yet
- Palatally Impacted Canines - Diagnosis and Treatment OptionsDocument7 pagesPalatally Impacted Canines - Diagnosis and Treatment OptionsKarim El MestekawyNo ratings yet
- Impacted Max CaninesDocument6 pagesImpacted Max CaninesAnkur AggarwalNo ratings yet
- Incisor Root Resorption Associated With Palatally Displaced Maxillary Canines: Analysis and Prediction Using Discriminant Function AnalysisDocument11 pagesIncisor Root Resorption Associated With Palatally Displaced Maxillary Canines: Analysis and Prediction Using Discriminant Function AnalysisnomanNo ratings yet
- Etiology of Maxillary Canine Impaction A ReviewDocument11 pagesEtiology of Maxillary Canine Impaction A ReviewMiltonfcc100% (1)
- Canino Ectopico A Nivel de Incisivo LateralDocument12 pagesCanino Ectopico A Nivel de Incisivo Lateralangianny_cdNo ratings yet
- Ectopic Tooth in The Anterior Wall of The Maxillary SinusDocument3 pagesEctopic Tooth in The Anterior Wall of The Maxillary Sinuspunct_org3256No ratings yet
- Impacted Maxillary CaninesDocument7 pagesImpacted Maxillary CaninesAly OsmanNo ratings yet
- Orthodontic Lect 27Document7 pagesOrthodontic Lect 27Said SaidNo ratings yet
- 30121-Article Text-56500-1-10-20200810Document7 pages30121-Article Text-56500-1-10-20200810IfadahNo ratings yet
- Oral Surgery 1 - Management of Impacted TeethDocument18 pagesOral Surgery 1 - Management of Impacted TeethMahasnehEhabNo ratings yet
- Art 2Document6 pagesArt 2Cristian OneaNo ratings yet
- Impacted CanineDocument162 pagesImpacted CanineNorhan Hossam Ahmed MohamedNo ratings yet
- Unusual Orthodontic Correction of Bilateral Maxillary Canine-First Premolar TranspositionDocument11 pagesUnusual Orthodontic Correction of Bilateral Maxillary Canine-First Premolar TranspositionAstrid DindaNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument39 pagesWorld's Largest Science, Technology & Medicine Open Access Book Publishernurjannah sriayuNo ratings yet
- Canine ImpactionDocument31 pagesCanine Impactionavanthika krishnarajNo ratings yet
- Sindrome Desostose Cleidocraniana-Trat OrtodDocument8 pagesSindrome Desostose Cleidocraniana-Trat Ortodbeh.chaves16No ratings yet
- PIIS0889540611003763Document11 pagesPIIS0889540611003763César Raúl Mauricio VilchezNo ratings yet
- Management of Impacted Canine: Anmol Goel Post Graduate Student Department of Orthodontics V.S Dental CollegeDocument193 pagesManagement of Impacted Canine: Anmol Goel Post Graduate Student Department of Orthodontics V.S Dental CollegeNeelima ChandranNo ratings yet
- Mcintyre Orthodontic Update Canine Part 1Document10 pagesMcintyre Orthodontic Update Canine Part 1Carlos MikaelNo ratings yet
- Reproduction - Boardwork 2Document32 pagesReproduction - Boardwork 2Zidańn100% (1)
- Making Your Career Plan: Integration of Life Goals, Values, Personality, Skills and AptitudeDocument18 pagesMaking Your Career Plan: Integration of Life Goals, Values, Personality, Skills and AptitudeRoella Mae MalinaoNo ratings yet
- 100 LB1 Grease - EnglishDocument7 pages100 LB1 Grease - EnglishbuddhansamratNo ratings yet
- Disaster Readiness and Risk Reduction: Quarter 1 - Module 3: Disasters and Its EffectsDocument16 pagesDisaster Readiness and Risk Reduction: Quarter 1 - Module 3: Disasters and Its EffectsKrystin DiamosNo ratings yet
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- Fazaia Medical CollageDocument33 pagesFazaia Medical Collagemeandershakier.0xNo ratings yet
- MELC-Based: West Fairview High School 2 Quarter - Week 6 in P.E 10Document23 pagesMELC-Based: West Fairview High School 2 Quarter - Week 6 in P.E 10Mau OlivaresNo ratings yet
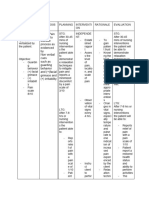
- Acute Pain Related To Disease Process As Evidenced by Non Verbal Cues Such As Guarding Behavior and (+) Facial Grimace and (+) IrritabilityDocument3 pagesAcute Pain Related To Disease Process As Evidenced by Non Verbal Cues Such As Guarding Behavior and (+) Facial Grimace and (+) IrritabilityKrystele CangaNo ratings yet
- Conex CompressionDocument32 pagesConex Compressionh2odavid100% (1)
- Ed 304 Module 3 Section BDocument22 pagesEd 304 Module 3 Section BAljun Bernadez Emperado78% (9)
- SMC Training Manual A4Document32 pagesSMC Training Manual A4vishal rohillaNo ratings yet
- Fire Safety - SOP 01 - Hot Works Permit ProcedureDocument3 pagesFire Safety - SOP 01 - Hot Works Permit ProcedurepikasNo ratings yet
- How Bad Nutrition Affects A Persons AppearnceDocument17 pagesHow Bad Nutrition Affects A Persons AppearnceZeina SadderNo ratings yet
- Pediatrics Examination - and Board Review.Document846 pagesPediatrics Examination - and Board Review.Diana SachelaruNo ratings yet
- Communicating With Clients With Dementia: ListenDocument4 pagesCommunicating With Clients With Dementia: ListeneNo ratings yet
- Waldenfels EthnopsiquiatríaDocument11 pagesWaldenfels Ethnopsiquiatríajulio-vargasNo ratings yet
- SUPPORTIVE STUDY Nisha PDFDocument129 pagesSUPPORTIVE STUDY Nisha PDFrizwanNo ratings yet
- INTRO Level of Awarenesss of Filipino Mothers SAMPLESDocument6 pagesINTRO Level of Awarenesss of Filipino Mothers SAMPLESKathleen Joy Costales MagtanongNo ratings yet
- Ieee PaperDocument5 pagesIeee PaperArya AnandanNo ratings yet
- Work Immersion-1st Summative TDocument4 pagesWork Immersion-1st Summative TJared Panes Sia50% (2)
- Compro Sangresik Facility Service 3 Nov EditDocument12 pagesCompro Sangresik Facility Service 3 Nov EditArif NurrahmanNo ratings yet
- Teen Vaping: What You Need To KnowDocument2 pagesTeen Vaping: What You Need To KnowSyafiq RasidiNo ratings yet
- Historical Development of Community Health and Community Health Nursing in India and WorldDocument37 pagesHistorical Development of Community Health and Community Health Nursing in India and WorldAni mathewNo ratings yet
- PhysicalEducation SrSec 2022-23Document4 pagesPhysicalEducation SrSec 2022-23Rashid AliNo ratings yet
- Construction Site Safety: Accident Reporting and InvestigationDocument11 pagesConstruction Site Safety: Accident Reporting and InvestigationProfessional TrustNo ratings yet
- Nursing Informatics Reviewer (Lab)Document190 pagesNursing Informatics Reviewer (Lab)Raquel MonsalveNo ratings yet
- First Box Content As Per Content Factory ActDocument4 pagesFirst Box Content As Per Content Factory ActjaglansunilNo ratings yet