Download as docx, pdf, or txt
You might also like
- MDT Guide and DocumentationDocument8 pagesMDT Guide and Documentationng58818aNo ratings yet
- AtlsDocument23 pagesAtlsvivi chanNo ratings yet
- Positioning of The Patient For Abdominal ExaminationDocument8 pagesPositioning of The Patient For Abdominal ExaminationDoctor Saleem RehmanNo ratings yet
- INTUSSUSCEPTIONDocument3 pagesINTUSSUSCEPTIONJanine Karla OrcaNo ratings yet
- DIVERTICULOSISDocument21 pagesDIVERTICULOSISTiffany AdriasNo ratings yet
- Acute Abdomen: DR Teamir Negussie Assistant Professor Dept of SurgeryDocument69 pagesAcute Abdomen: DR Teamir Negussie Assistant Professor Dept of SurgeryteamirNo ratings yet
- Adrias - CROHN'S DISEASEDocument19 pagesAdrias - CROHN'S DISEASETiffany AdriasNo ratings yet
- HP Nov02 PainDocument6 pagesHP Nov02 PainSampath GoudNo ratings yet
- APPENDICITISDocument37 pagesAPPENDICITISjohn paul richard mindanaoNo ratings yet
- Acute Appendicitis PaedsDocument5 pagesAcute Appendicitis PaedsemmaazizNo ratings yet
- Acute Raptured Appendicitis - VMCDocument6 pagesAcute Raptured Appendicitis - VMCMicahMananguitNo ratings yet
- Intussusception: Prepared By: Aisha H. AlaghaDocument20 pagesIntussusception: Prepared By: Aisha H. AlaghaaiooshaNo ratings yet
- Examination of The AbdomenDocument19 pagesExamination of The AbdomenAllen AykayNo ratings yet
- Approach To Abdominal PainDocument44 pagesApproach To Abdominal PainEleanorNo ratings yet
- Abdomen ScriptDocument14 pagesAbdomen Scriptadrian nakilaNo ratings yet
- AppendicitisDocument17 pagesAppendicitisAhmed Halaby100% (1)
- Research MethodsDocument6 pagesResearch MethodsDesmond Grasie ZumankyereNo ratings yet
- Nursing Assessment: Patient History, An Infant or A Child May Be Relatively Free From Symptom Until She or He CriesDocument4 pagesNursing Assessment: Patient History, An Infant or A Child May Be Relatively Free From Symptom Until She or He Criescyrilcarinan100% (1)
- Appendicitis Is A Condition Characterized by Inflammation of The Appendix. It Is Classified As A MedicalDocument5 pagesAppendicitis Is A Condition Characterized by Inflammation of The Appendix. It Is Classified As A Medicalbhe_jewelNo ratings yet
- AbdominDocument4 pagesAbdominDl Al-azizNo ratings yet
- What Is IntussusceptionDocument11 pagesWhat Is IntussusceptionNatoya ChristieNo ratings yet
- Health Assessment SAS Session 16Document5 pagesHealth Assessment SAS Session 16Mary Maxiluch TabudlongNo ratings yet
- Nursing Care Plan For Inguinal Hernia HBDocument4 pagesNursing Care Plan For Inguinal Hernia HBdheeneshbabu0% (1)
- Sample Chapter 9780323399562Document23 pagesSample Chapter 9780323399562TaeyomiNo ratings yet
- Dipolog Medical Center College Foundation Inc. College of NursingDocument16 pagesDipolog Medical Center College Foundation Inc. College of NursingTiffany AdriasNo ratings yet
- AbdomenDocument18 pagesAbdomenMuhammad FahmyNo ratings yet
- Approach To Abd PainDocument23 pagesApproach To Abd Painoscar3spurgeonNo ratings yet
- Abdominal PainDocument12 pagesAbdominal PainGeeza Gem VicencioNo ratings yet
- Ectopic PregnancyDocument13 pagesEctopic PregnancyJonielyn LagunaNo ratings yet
- Scrotal HerniaDocument9 pagesScrotal HerniaReymart BolagaoNo ratings yet
- Crohn's DiseaseDocument20 pagesCrohn's DiseaseTiffany AdriasNo ratings yet
- Physical Assessment - Yuli PutriDocument4 pagesPhysical Assessment - Yuli PutriIkadek AgustianaNo ratings yet
- A Case Study of RupturedDocument12 pagesA Case Study of RupturedkisNo ratings yet
- A Case PresentationDocument50 pagesA Case PresentationAnaleah MalayaoNo ratings yet
- Assessment Appendicitis 1Document1 pageAssessment Appendicitis 1Aoshi ShinomoriNo ratings yet
- Dyspepsia BrochureDocument5 pagesDyspepsia BrochureJns RamNo ratings yet
- Trinity University of Asia: St. Luke's College of NursingDocument18 pagesTrinity University of Asia: St. Luke's College of NursingKate Duque100% (1)
- What Is IntussusceptionDocument3 pagesWhat Is IntussusceptionPatrick John CruzNo ratings yet
- Exam of The AbdomenDocument11 pagesExam of The AbdomenjohnNo ratings yet
- Acute Abdominal Pain in ChildrenDocument8 pagesAcute Abdominal Pain in ChildrenSophiNo ratings yet
- Intussuseption and Hirschprung's DiseaseDocument5 pagesIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- Presented by Dr. Ayalew ZDocument35 pagesPresented by Dr. Ayalew Zyared getachewNo ratings yet
- Appendicitis (History & Examination)Document6 pagesAppendicitis (History & Examination)Doctor Saleem Rehman75% (4)
- Pedia PT3Document8 pagesPedia PT3sonava vichNo ratings yet
- Appendicitis DR WellDocument17 pagesAppendicitis DR Wellk.adeputriNo ratings yet
- Nursing InterventionsDocument3 pagesNursing InterventionsJemiah Lyn C. BragadoNo ratings yet
- IntussusceptionDocument4 pagesIntussusceptionlovethestarNo ratings yet
- Nursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument7 pagesNursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationHanz Abbigail Roco100% (1)
- INTUSSUSCEPTION2Document3 pagesINTUSSUSCEPTION2Jade RubyNo ratings yet
- Abdominal Pain PDFDocument23 pagesAbdominal Pain PDFSahil DhamijaNo ratings yet
- Maternal Finals ReportDocument21 pagesMaternal Finals ReportLaude Sebastian DanNo ratings yet
- LI - Physical Examination - AbdomenDocument6 pagesLI - Physical Examination - AbdomenTravis DonohoNo ratings yet
- Nursing Care Plan APDocument3 pagesNursing Care Plan APMargarita PaureneNo ratings yet
- CMS Ob&Gyn 1 AnswersDocument13 pagesCMS Ob&Gyn 1 AnswersMohamed Abib100% (6)
- AppendicitisDocument3 pagesAppendicitisPrince Jhessie L. AbellaNo ratings yet
- Signs and SymptomsDocument4 pagesSigns and SymptomsRizki KhairNo ratings yet
- APPENDECITISDocument5 pagesAPPENDECITISfxbukenyaNo ratings yet
- Abdominal Examination UMYDocument181 pagesAbdominal Examination UMYMspitha LiaNo ratings yet
- IntussusceptionDocument2 pagesIntussusceptionAireen Mae P. NapigkitNo ratings yet
- Inspection, Auscultation, Palpation, and Percussion of The AbdomenDocument16 pagesInspection, Auscultation, Palpation, and Percussion of The AbdomenKaye ExeveaNo ratings yet
- AppendicitesDocument4 pagesAppendicitesBashar KhalilNo ratings yet
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 1 out of 5 stars1/5 (1)
- Rheumatic Fever (Caypuno, Isaac-Lee P.)Document15 pagesRheumatic Fever (Caypuno, Isaac-Lee P.)Carlojay IniegoNo ratings yet
- Scabies (Calaustro Kyla)Document22 pagesScabies (Calaustro Kyla)Carlojay IniegoNo ratings yet
- Scoliosis (Coleto, Leonard-And Cruz, Princess)Document10 pagesScoliosis (Coleto, Leonard-And Cruz, Princess)Carlojay IniegoNo ratings yet
- Pediculosis (Cantorne, Sharmaine E)Document10 pagesPediculosis (Cantorne, Sharmaine E)Carlojay IniegoNo ratings yet
- Arthritis (Cabansag, Ma. Flor-And-Cabansag, Joyce)Document38 pagesArthritis (Cabansag, Ma. Flor-And-Cabansag, Joyce)Carlojay IniegoNo ratings yet
- Impetigo (Calonge, Edwilyn)Document14 pagesImpetigo (Calonge, Edwilyn)Carlojay IniegoNo ratings yet
- Meningitis (Marcos Mighty Er)Document5 pagesMeningitis (Marcos Mighty Er)Carlojay IniegoNo ratings yet
- Osteosarcoma (Dalit, Kate Trixie-And-baybado, Janice)Document26 pagesOsteosarcoma (Dalit, Kate Trixie-And-baybado, Janice)Carlojay IniegoNo ratings yet
- Leukemia (Sapongay Charice)Document29 pagesLeukemia (Sapongay Charice)Carlojay IniegoNo ratings yet
- Urinary Tract Infection (Maramag Eunice Laman Jenny Pearl)Document16 pagesUrinary Tract Infection (Maramag Eunice Laman Jenny Pearl)Carlojay IniegoNo ratings yet
- Wilms-Tumor (Respicio Trixie)Document18 pagesWilms-Tumor (Respicio Trixie)Carlojay IniegoNo ratings yet
- The Family and Family HealthDocument100 pagesThe Family and Family HealthCarlojay IniegoNo ratings yet
- Hyperbilirubinemia (Gerardo, Maria Maricar P)Document11 pagesHyperbilirubinemia (Gerardo, Maria Maricar P)Carlojay IniegoNo ratings yet
- Cerebral Palsy (Morta Kate)Document41 pagesCerebral Palsy (Morta Kate)Carlojay IniegoNo ratings yet
- Sepsis in Newborns (Flores, Christine Mae & Espiritu, Richelle)Document9 pagesSepsis in Newborns (Flores, Christine Mae & Espiritu, Richelle)Carlojay IniegoNo ratings yet
- Febrile Seizure (Macapia Ivy and Manalo Ricca)Document8 pagesFebrile Seizure (Macapia Ivy and Manalo Ricca)Carlojay IniegoNo ratings yet
- Bronchial Asthma (Parinas Rhoanne)Document10 pagesBronchial Asthma (Parinas Rhoanne)Carlojay IniegoNo ratings yet
- Respiratory Distress Syndrome (Iniego Carlo Jay)Document9 pagesRespiratory Distress Syndrome (Iniego Carlo Jay)Carlojay IniegoNo ratings yet
- Diabetes Mellitus (Maglelong Kristine)Document27 pagesDiabetes Mellitus (Maglelong Kristine)Carlojay IniegoNo ratings yet
- Sudden Infant Death Syndrome (Dela Crus, Christian Jess)Document13 pagesSudden Infant Death Syndrome (Dela Crus, Christian Jess)Carlojay IniegoNo ratings yet
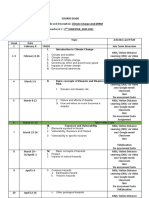
- Course Guide: I. Introduction To Climate ChangeDocument2 pagesCourse Guide: I. Introduction To Climate ChangeCarlojay IniegoNo ratings yet
- Drugs Acting On: Renal SystemDocument75 pagesDrugs Acting On: Renal SystemCarlojay IniegoNo ratings yet
- Meconium Aspiration Syndrome (Daran, Maria Ranela)Document8 pagesMeconium Aspiration Syndrome (Daran, Maria Ranela)Carlojay IniegoNo ratings yet
- Climate Change COURSE GUIDEDocument2 pagesClimate Change COURSE GUIDECarlojay IniegoNo ratings yet
- Colic (Gattering, John Paul & Francisco, Solemnio)Document6 pagesColic (Gattering, John Paul & Francisco, Solemnio)Carlojay IniegoNo ratings yet
- Decreased Cardiac OutputDocument3 pagesDecreased Cardiac OutputCarlojay IniegoNo ratings yet
- Blood Glucose Monitoring: Romulo D. Lopez JR, RN LPTDocument15 pagesBlood Glucose Monitoring: Romulo D. Lopez JR, RN LPTCarlojay IniegoNo ratings yet
- Hand Sanitizer: Using Fresh Citrus Sinensis (Orange) and Barbadensis-Miller (Aloe Vera)Document4 pagesHand Sanitizer: Using Fresh Citrus Sinensis (Orange) and Barbadensis-Miller (Aloe Vera)Carlojay IniegoNo ratings yet
- Antepartum Iniego Carlo Jay P: PurposeDocument8 pagesAntepartum Iniego Carlo Jay P: PurposeCarlojay IniegoNo ratings yet
- Vol 11Document108 pagesVol 11Anavin TonNo ratings yet
- Case Study Nursing Diagnosis of PneumothoraxDocument8 pagesCase Study Nursing Diagnosis of PneumothoraxJansen Arquilita RiveraNo ratings yet
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- TD Vaccine Operational GuidelinesDocument2 pagesTD Vaccine Operational GuidelinesSiddhartha NandiNo ratings yet
- Without Anskey-Ms RF, Ortho, Neuro - DrillsDocument13 pagesWithout Anskey-Ms RF, Ortho, Neuro - Drillsjon elleNo ratings yet
- 991111 EUS教學 (6) 重點式急診心臟超音波之應用Document67 pages991111 EUS教學 (6) 重點式急診心臟超音波之應用juice119100% (5)
- Clinical Pharmacy FinalDocument83 pagesClinical Pharmacy FinalAbin ChandrakumarNo ratings yet
- Sonopuls 492: Enraf-Nonius Enraf-NoniusDocument14 pagesSonopuls 492: Enraf-Nonius Enraf-NoniusRekha SatheesanNo ratings yet
- MT632 Unit 1 Introduction Human Anatomy and Physiology Chapter 1 The BasicsDocument12 pagesMT632 Unit 1 Introduction Human Anatomy and Physiology Chapter 1 The BasicsTia MallariNo ratings yet
- Flow RateDocument2 pagesFlow Rateفيرمان ريشادNo ratings yet
- Final DRDNB Seats For SS Counselling 2021Document152 pagesFinal DRDNB Seats For SS Counselling 2021Pavan KumarNo ratings yet
- QwewqeDocument1 pageQwewqeMuneeb ShahzadNo ratings yet
- Case Protocol SampleDocument1 pageCase Protocol SampleMarco Paulo Reyes NaoeNo ratings yet
- Hemorrhoid BandingDocument47 pagesHemorrhoid BandingAslam AssandakaniNo ratings yet
- Schizophrenia Case StudyDocument14 pagesSchizophrenia Case Studyapi-593859653No ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- Bates Chapter 7 - HEENTDocument87 pagesBates Chapter 7 - HEENTGuia De GuzmanNo ratings yet
- Maste Med SheetDocument78 pagesMaste Med SheetBarbie Wiggers100% (1)
- Wikipedia - Epididymitis (CHECKED)Document6 pagesWikipedia - Epididymitis (CHECKED)pixoguiasNo ratings yet
- Ineffective Tissue PerfussionDocument2 pagesIneffective Tissue Perfussionmonico39No ratings yet
- Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of EstradiolDocument8 pagesComparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of EstradiolSindatricks ZorokaNo ratings yet
- Stop The Bleed Booklet FinalDocument16 pagesStop The Bleed Booklet FinalUrsula MalauNo ratings yet
- Distribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemDocument3 pagesDistribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemirmaarmiyahNo ratings yet
- ITLSAdvancedPre TestDocument8 pagesITLSAdvancedPre TestMuhammad AsifNo ratings yet
- Preterm Labor, Hyperemesis Gravidarum - PathophysiologyDocument2 pagesPreterm Labor, Hyperemesis Gravidarum - PathophysiologyreyneldanNo ratings yet
- BSP-Medical FormDocument1 pageBSP-Medical FormNyleg Aicilag100% (2)
- (ERS Monograph) Fransesco Bonella, Daniel Culver, Dominique Israel - Biet - Sarcoidosis ERS Monograph-European Respiratory Society (2022)Document364 pages(ERS Monograph) Fransesco Bonella, Daniel Culver, Dominique Israel - Biet - Sarcoidosis ERS Monograph-European Respiratory Society (2022)Carmen IlarieNo ratings yet
- Emerging in MalariaDocument8 pagesEmerging in MalariaEmad OsmanNo ratings yet