Download as pdf or txt
You might also like
- Critical Appraisal of JournalDocument4 pagesCritical Appraisal of JournalRetno Sumara100% (1)
- Encyclopedia Engineering GeologyDocument979 pagesEncyclopedia Engineering GeologyGalhaadis100% (1)
- Mayur Reliance Trends ProjectDocument52 pagesMayur Reliance Trends ProjectSanjay RanvaNo ratings yet
- PESTEL Analysis of Mother EarthDocument9 pagesPESTEL Analysis of Mother EarthSreyasNo ratings yet
- Impact of Information System On Organization (Literature Review)Document11 pagesImpact of Information System On Organization (Literature Review)Md. Nazmus Sakib100% (1)
- EmphatyDocument4 pagesEmphatyPutri SandiekaNo ratings yet
- Hojat 2004Document8 pagesHojat 2004Jair Benavente AsinNo ratings yet
- Validación - Escala de EmpatiaDocument7 pagesValidación - Escala de EmpatiaNidia MontoyaNo ratings yet
- Erosion of Empathy in Medical SchoolDocument1 pageErosion of Empathy in Medical SchoolChristian ObandoNo ratings yet
- Chen2007 Article ACross-sectionalMeasurementOfMDocument5 pagesChen2007 Article ACross-sectionalMeasurementOfMSPE CommitteeNo ratings yet
- An Assessment of Dental Students' Empathy Levels in MalaysiaDocument7 pagesAn Assessment of Dental Students' Empathy Levels in MalaysiaAngelia PratiwiNo ratings yet
- Emergency Department Patient Experience - A Systematic Review of The LiteratureDocument6 pagesEmergency Department Patient Experience - A Systematic Review of The LiteratureMauricio Garcia RomeroNo ratings yet
- En CuestaDocument6 pagesEn CuestaToño VargasNo ratings yet
- Journal Pone 0094207Document7 pagesJournal Pone 0094207JuanaNo ratings yet
- Infeksi Nifas PublisherDocument4 pagesInfeksi Nifas PublisherYayha AgathaaNo ratings yet
- EMP2 2 E12546Document10 pagesEMP2 2 E12546Nelson Da VegaNo ratings yet
- Preguntas Clínicas, Obstáculos y SolucionesDocument8 pagesPreguntas Clínicas, Obstáculos y SolucionesLOVELYMAKEUP COLNo ratings yet
- Content ServerDocument10 pagesContent ServersyarifaNo ratings yet
- Adherence and Medication Adherence Rating Scale (MARS)Document4 pagesAdherence and Medication Adherence Rating Scale (MARS)International Journal of Innovative Science and Research TechnologyNo ratings yet
- File For Plagiarism Checking (Fizza)Document16 pagesFile For Plagiarism Checking (Fizza)Iqra AsimNo ratings yet
- A Brief Instrument To Measure Patients Overall SaDocument7 pagesA Brief Instrument To Measure Patients Overall Sa2225106050995No ratings yet
- Integrative ReviewDocument20 pagesIntegrative Reviewapi-485309887No ratings yet
- Measuring Clinical Reasoning and Interprofessional AttitudesDocument6 pagesMeasuring Clinical Reasoning and Interprofessional AttitudesVizaNo ratings yet
- Research ForumDocument34 pagesResearch ForumJustine May GervacioNo ratings yet
- Assessing Family Satisfaction With Care of Critically Ill Patients: A Pilot StudyDocument9 pagesAssessing Family Satisfaction With Care of Critically Ill Patients: A Pilot StudyCejoy AnnNo ratings yet
- Epstein 2007 Assessmentin Medical EducationDocument11 pagesEpstein 2007 Assessmentin Medical Educationwedad jumaNo ratings yet
- 5 The Impact of Depression On The Academic Productivity of University Students PDFDocument7 pages5 The Impact of Depression On The Academic Productivity of University Students PDFLim Shwe Wen100% (1)
- Assessment of Medical Students ' Shared Decision-Making in Standardized Patient EncountersDocument6 pagesAssessment of Medical Students ' Shared Decision-Making in Standardized Patient EncountersAlex Mauricio Ochoa LuzuriagaNo ratings yet
- Diabetes Spectr 2007 Derr 177 85Document9 pagesDiabetes Spectr 2007 Derr 177 85Juankarloz MedinaNo ratings yet
- Shashi Kumar 2014Document7 pagesShashi Kumar 2014SPE CommitteeNo ratings yet
- Swoope1977 PDFDocument8 pagesSwoope1977 PDFKrupali JainNo ratings yet
- PublishedEBParticle JournalofAlliedHealth CardinDocument11 pagesPublishedEBParticle JournalofAlliedHealth Cardinag wahyudiNo ratings yet
- JHPN 24 E151Document8 pagesJHPN 24 E151MentiEndah dwi SeptianiNo ratings yet
- Interprofessional Collaboration in Primary Health CareDocument12 pagesInterprofessional Collaboration in Primary Health Caremira maryanilaifaNo ratings yet
- How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyDocument17 pagesHow Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyAlexNo ratings yet
- Comprehensive Assessment of Professional CompetenceDocument11 pagesComprehensive Assessment of Professional CompetenceRizka PutrantiNo ratings yet
- 0rder 343 NRS-493-ASSIGNMENT 3 Literature ReviewDocument6 pages0rder 343 NRS-493-ASSIGNMENT 3 Literature Reviewjoshua chegeNo ratings yet
- Quantitative QritiqueDocument8 pagesQuantitative QritiqueShaheen NazakatNo ratings yet
- Article File16071Document14 pagesArticle File16071AnuragNo ratings yet
- Measuring Empathy Among Dental Students and InternDocument7 pagesMeasuring Empathy Among Dental Students and InternMuthia alyshaNo ratings yet
- Fountain 2016Document23 pagesFountain 2016Alfred RodNo ratings yet
- View ContentDocument5 pagesView Contentpiah89No ratings yet
- Patient and Family Member Factors Influencing Outcomes of Poststroke Inpatient RehabilitationDocument9 pagesPatient and Family Member Factors Influencing Outcomes of Poststroke Inpatient RehabilitationAdelya YuzyNo ratings yet
- Users' Views of Dietary SupplementsDocument3 pagesUsers' Views of Dietary SupplementsJave GajellomaNo ratings yet
- Self-Reported Professional Competencies of RN-to-BSN StudentsDocument55 pagesSelf-Reported Professional Competencies of RN-to-BSN StudentsNabeeha FazeelNo ratings yet
- A Review of The Evidence and Recommendations On Communication Skills and The PatientDocument26 pagesA Review of The Evidence and Recommendations On Communication Skills and The PatientThayna MirandaNo ratings yet
- 8 145 - Text With Cover Page v2Document8 pages8 145 - Text With Cover Page v2kkkjaegiNo ratings yet
- NIH Public AccessDocument15 pagesNIH Public AccessSofía SciglianoNo ratings yet
- A Level Psycology Unit 3 Exam Studies.173697407Document47 pagesA Level Psycology Unit 3 Exam Studies.173697407VF MariaNo ratings yet
- Essay 3 4Document6 pagesEssay 3 4api-743531083No ratings yet
- Am I Doing The Right Thing Provider Perspectives On Improving Palliative Care in The Emergency Department 2009 Annals of Emergency MedicineDocument9 pagesAm I Doing The Right Thing Provider Perspectives On Improving Palliative Care in The Emergency Department 2009 Annals of Emergency MedicineTUTIK SISWATINo ratings yet
- Research Papers On Clinical PharmacyDocument6 pagesResearch Papers On Clinical Pharmacyaflbrtdar100% (1)
- Chigerwe Et Al. (2021)Document13 pagesChigerwe Et Al. (2021)Martín TPNo ratings yet
- Chapter 004Document8 pagesChapter 004Dr-Sanjay SinghaniaNo ratings yet
- Interventions To Enhance Communication Among Patients, Providers, and FamiliesDocument8 pagesInterventions To Enhance Communication Among Patients, Providers, and FamiliesvabcunhaNo ratings yet
- Sample Article CritiqueDocument7 pagesSample Article CritiquerebeccaNo ratings yet
- Prescribing Habits and CaregivDocument10 pagesPrescribing Habits and CaregivHerawati YustikasariNo ratings yet
- Disability Attitudes in Health Care: A New Scale InstrumentDocument12 pagesDisability Attitudes in Health Care: A New Scale InstrumentLeila FortesNo ratings yet
- Essay 3 2 1Document6 pagesEssay 3 2 1api-743531083No ratings yet
- Perceptions of Healthcare Professionals Towards Palliative Care in Internal Medicine Wards: A Cross-Sectional SurveyDocument8 pagesPerceptions of Healthcare Professionals Towards Palliative Care in Internal Medicine Wards: A Cross-Sectional SurveyRahmanu ReztaputraNo ratings yet
- Nursing JournalDocument28 pagesNursing JournalDimas SanjayaNo ratings yet
- Nurs702 Critique Final2Document9 pagesNurs702 Critique Final2natalie nodayNo ratings yet
- Jurnal InternasionallDocument17 pagesJurnal Internasionallmercy tobingNo ratings yet
- CPCSEA Status of Resistered EstablishmentsDocument220 pagesCPCSEA Status of Resistered EstablishmentsNaresh Kadyan100% (1)
- Instructional Module For Practical Research 1: Qualitative ResearchDocument4 pagesInstructional Module For Practical Research 1: Qualitative ResearchRayle ParconNo ratings yet
- Case Study of Housing Development With Optimization of Housing Land Utilization by Using Linear ProgramsDocument7 pagesCase Study of Housing Development With Optimization of Housing Land Utilization by Using Linear ProgramsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Program PlanningDocument56 pagesProgram PlanningVinceEjorangoCabigao0% (1)
- Chapter IIIDocument5 pagesChapter IIIapi-3747282100% (1)
- Survey QuestionsDocument3 pagesSurvey QuestionsShreya ChauhanNo ratings yet
- CS408 Quiz-1 File by Vu Topper RM-1-1Document70 pagesCS408 Quiz-1 File by Vu Topper RM-1-1Abdullahaftab RajpootNo ratings yet
- Jurnal PPPDocument12 pagesJurnal PPPFuad AhmadNo ratings yet
- BCF 403 Fundamentals of Production and Operations MGT - Module 2 PDFDocument22 pagesBCF 403 Fundamentals of Production and Operations MGT - Module 2 PDFNaresh KumarNo ratings yet
- Community AssessmentDocument3 pagesCommunity AssessmentDarcy Hamada100% (1)
- Analyzing The Need of Women Empowerment in Reference To Sarvpriye FoundationDocument26 pagesAnalyzing The Need of Women Empowerment in Reference To Sarvpriye FoundationMohit SinghNo ratings yet
- CAE Use of English (Test 2)Document3 pagesCAE Use of English (Test 2)Hu ChiNo ratings yet
- Research QuestionnaireDocument2 pagesResearch QuestionnaireSTEM1 LOPEZNo ratings yet
- Total Quality Management MCQ'sDocument51 pagesTotal Quality Management MCQ'sAli Murtaza0% (1)
- Dissertation - Wan Aizam Syahira BT Wan Sohaimi - 14295 - Sept2014Document64 pagesDissertation - Wan Aizam Syahira BT Wan Sohaimi - 14295 - Sept2014shayanNo ratings yet
- SPR-00 Sekilas Tentang NQAF Indonesia (Final Rev) - English VersionDocument48 pagesSPR-00 Sekilas Tentang NQAF Indonesia (Final Rev) - English VersionwahyudinNo ratings yet
- Academic Resilience As Mediator of Multidimensional Perfectionism and Academic Performance Among Gen-Z Undergraduate StudentsDocument10 pagesAcademic Resilience As Mediator of Multidimensional Perfectionism and Academic Performance Among Gen-Z Undergraduate StudentsStefan HlNo ratings yet
- Medallia Customer Benchmark 2016Document1 pageMedallia Customer Benchmark 2016Jay MellmanNo ratings yet
- Evaluation of Flitch Plate Losses in Power TransformersDocument1 pageEvaluation of Flitch Plate Losses in Power TransformersVictor Julián Fernández CarrazanaNo ratings yet
- Sustainability Reporting in The PhilippinesDocument45 pagesSustainability Reporting in The PhilippinessarahbeeNo ratings yet
- Major Schools of Literary CriticismDocument1 pageMajor Schools of Literary CriticismJeeva MJNo ratings yet
- CM - Selection of Head ContractorDocument28 pagesCM - Selection of Head ContractorAmir YacoubNo ratings yet
- Brochures MSC & MBA - enDocument34 pagesBrochures MSC & MBA - ennoviantysyahriNo ratings yet
- 5E Lesson Plan Template: TeacherDocument3 pages5E Lesson Plan Template: Teacherapi-554354302No ratings yet
- The Comparative e Cacy of Two Approaches To Teaching Sixth Graders Opinion Essay WritingDocument28 pagesThe Comparative e Cacy of Two Approaches To Teaching Sixth Graders Opinion Essay WritingFlorencia FerreroNo ratings yet
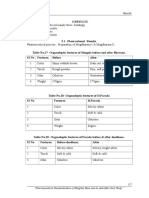
- Results: "Pharmaceutical Standardization of Mugdha Rasa and Its Anti-Microbial StudyDocument8 pagesResults: "Pharmaceutical Standardization of Mugdha Rasa and Its Anti-Microbial StudyPreet ChahalNo ratings yet