Download as pdf or txt
You might also like
- Test - II Test-I: Confirmatory Request FormDocument2 pagesTest - II Test-I: Confirmatory Request FormMSL Laboratory79% (14)
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- National Immunization Program: Manual of Procedures Booklet 11Document42 pagesNational Immunization Program: Manual of Procedures Booklet 11Blue PielagoNo ratings yet
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayNo ratings yet
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- NRC Sam Chart: For Oedematous Child Admission Weight Will Be The Weight Taken On The Day The Child Has No OedemaDocument5 pagesNRC Sam Chart: For Oedematous Child Admission Weight Will Be The Weight Taken On The Day The Child Has No OedemaadiNo ratings yet
- Typhoid-FoodNET CRFDocument3 pagesTyphoid-FoodNET CRFMisty JhaNo ratings yet
- Typhoid Fever Surveillance ReportDocument2 pagesTyphoid Fever Surveillance ReportMarketing HydNo ratings yet
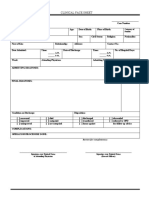
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDocument15 pagesClinical Face Sheet: - A.M. - P.M. - A.M. - P.MNikitaCaitlynLeyaleyNo ratings yet
- CIF MALARIA - Rev4 As July 4 2016 - LatestDocument3 pagesCIF MALARIA - Rev4 As July 4 2016 - LatestNicholai Cabaddu100% (2)
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDocument16 pagesClinical Face Sheet: - A.M. - P.M. - A.M. - P.MCezanne CruzNo ratings yet
- Patients Chart For StudentsDocument18 pagesPatients Chart For StudentsRyrey Abraham PacamanaNo ratings yet
- SampleAnsBookP2 ENDocument8 pagesSampleAnsBookP2 ENmasterNo ratings yet
- Case Report Form Template: Protocol: (Insert Protocol NumberDocument28 pagesCase Report Form Template: Protocol: (Insert Protocol NumberSyvelmarie TinteNo ratings yet
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormBarbie CincoNo ratings yet
- Liver Disease Questionnaire For Proposed Insured/OwnerDocument2 pagesLiver Disease Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYClaire FNo ratings yet
- History FormDocument5 pagesHistory FormYazeed AsrawiNo ratings yet
- Vomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Document4 pagesVomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Peter GirasolNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Group 5 - Obstetrics History SheetDocument4 pagesGroup 5 - Obstetrics History SheetArianne Courtney NacarNo ratings yet
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDocument11 pagesClinical Face Sheet: - A.M. - P.M. - A.M. - P.M3B NOVIDA, ALEYA G.No ratings yet
- Aefi CifDocument6 pagesAefi CifVic KwanNo ratings yet
- Patient Past Medical, Social & Family HistoryDocument5 pagesPatient Past Medical, Social & Family HistoryNashwa Rashed100% (1)
- Measles Case FormDocument3 pagesMeasles Case FormVlad BăhneanuNo ratings yet
- NCM 104 Family Profiling FormDocument6 pagesNCM 104 Family Profiling FormKyle Randolf CuevasNo ratings yet
- Surgical Safety ChecklistDocument1 pageSurgical Safety ChecklistАндрій ДанильцівNo ratings yet
- Community Survey - Profiling-FormDocument6 pagesCommunity Survey - Profiling-FormrodcyruskentNo ratings yet
- New-Patient-Forms-All-2020 GoodDocument8 pagesNew-Patient-Forms-All-2020 GoodCheryl WanNo ratings yet
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYNorjetalexis CabreraNo ratings yet
- Afp CifDocument2 pagesAfp CifMurari Rajendraprasad100% (1)
- Certificate of HealthDocument1 pageCertificate of HealthGabriela Chevez GarciaNo ratings yet
- KipiDocument1 pageKipiHeRha DAniarNo ratings yet
- Clinical Face Sheet: Category of PatientDocument14 pagesClinical Face Sheet: Category of PatientMarjorie UmipigNo ratings yet
- MODULE - 5.4 0-6monthDocument29 pagesMODULE - 5.4 0-6monthabdullahi bashiirNo ratings yet
- Hypertension Questionnaire For Proposed Insured/OwnerDocument1 pageHypertension Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Afp 2013Document2 pagesAfp 2013rhu silagoNo ratings yet
- Case Scenario Mohsen SaadDocument6 pagesCase Scenario Mohsen SaadIbrahim HemdanNo ratings yet
- Epilepsy Questionnaire For Proposed Insured/OwnerDocument1 pageEpilepsy Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Institute of Epidemiology, Disease Control and Research (IEDCR) COVID-19 Suspected Case Record FormDocument1 pageInstitute of Epidemiology, Disease Control and Research (IEDCR) COVID-19 Suspected Case Record Formsifat adnanNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars Cov2) : Section A - Patient DetailsDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars Cov2) : Section A - Patient Detailseldridatech pvt ltdNo ratings yet
- BookDocument6 pagesBookRajesh WadiwaNo ratings yet
- Suidi Oklahoma ProviderDocument28 pagesSuidi Oklahoma ProviderJesse M. MassieNo ratings yet
- Case Investigation Form - Acute Flaccid ParalysisDocument2 pagesCase Investigation Form - Acute Flaccid Paralysisclaverialc10No ratings yet
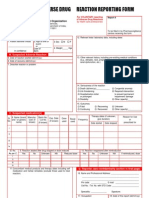
- ADR Form PDFDocument2 pagesADR Form PDFcompudoc111905No ratings yet
- Obstetrical History Previous Pregnancies Complicated With YES NO Family HistoryDocument2 pagesObstetrical History Previous Pregnancies Complicated With YES NO Family HistoryDesiree Cecilio ManlangitNo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- Maap Health ChecklistDocument1 pageMaap Health ChecklistRaymund MagallonesNo ratings yet
- Gegm Medical Report Physician FormDocument2 pagesGegm Medical Report Physician FormJohn SlowNo ratings yet
- Measles Case Reporting Form I.Case Identification/ Demographic DetailsDocument2 pagesMeasles Case Reporting Form I.Case Identification/ Demographic DetailsActivity ManagerNo ratings yet
- DD MM y y y y 8. Signs and Symptoms:: Laboratory Investigation Form FOR-Q05-003-01Document1 pageDD MM y y y y 8. Signs and Symptoms:: Laboratory Investigation Form FOR-Q05-003-01Camille deanNo ratings yet
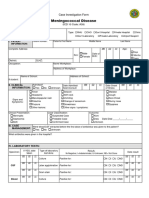
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- HuggDocument1 pageHuggGFVNo ratings yet
- Ad 2023Document1 pageAd 2023GFVNo ratings yet
- Ado5 Feb 2023Document1 pageAdo5 Feb 2023GFVNo ratings yet
- Adobe Scan 05-Feb-2023Document1 pageAdobe Scan 05-Feb-2023GFVNo ratings yet
- Systemic Response To InjuryDocument15 pagesSystemic Response To InjuryJohnVincentPagaddu100% (1)
- Pathophysiology - Chicken Pox Paper PDFDocument6 pagesPathophysiology - Chicken Pox Paper PDFRhiannon MartinNo ratings yet
- International Immunopharmacology: Hyun Jee Han, Chinekwu Nwagwu, Obumneme Anyim, Chinedu Ekweremadu, San KimDocument11 pagesInternational Immunopharmacology: Hyun Jee Han, Chinekwu Nwagwu, Obumneme Anyim, Chinedu Ekweremadu, San KimyoshefarieNo ratings yet
- Bacitracin Disks: Interpretation of ResultsDocument2 pagesBacitracin Disks: Interpretation of ResultsOsama BakheetNo ratings yet
- Vainionpää R, Leinikki P. 2008. Encyclopedia of Virology (Third Edition) - Camridge (US) Academic Press.Document9 pagesVainionpää R, Leinikki P. 2008. Encyclopedia of Virology (Third Edition) - Camridge (US) Academic Press.Annisa YohanesNo ratings yet
- TORCHDocument31 pagesTORCHRupali Arora100% (3)
- Dermatology Finals (Sept. 2014)Document14 pagesDermatology Finals (Sept. 2014)Paz VidaNo ratings yet
- CH 147 MeaslesDocument7 pagesCH 147 Measlesroshen02No ratings yet
- Infectious Diseaes and ModelingDocument46 pagesInfectious Diseaes and ModelingIntan GeaNo ratings yet
- Norovirus LetterDocument2 pagesNorovirus LetterLarryDCurtisNo ratings yet
- Spanish Flu Vs Covid-19Document7 pagesSpanish Flu Vs Covid-19api-599248532No ratings yet
- Acute Cellulitis and Erysipelas in Adults - Treatment - UpToDateDocument28 pagesAcute Cellulitis and Erysipelas in Adults - Treatment - UpToDateYahir PerezNo ratings yet
- CPC Case 1Document9 pagesCPC Case 1Astarte DimasalangNo ratings yet
- Soal UasDocument10 pagesSoal UasDila ZeinNo ratings yet
- Ekakustha and CarmakushtaDocument32 pagesEkakustha and CarmakushtaVenkatesan VidhyaNo ratings yet
- 17Document7 pages17bie2xNo ratings yet
- SR NO NO: Review of Anatomy and Physiology of BloodDocument14 pagesSR NO NO: Review of Anatomy and Physiology of BloodPdianghunNo ratings yet
- 2 - Introduction To VirusesDocument32 pages2 - Introduction To VirusesrostandtchangoueNo ratings yet
- Cleaning+Standards+2021 v1.0+ (Revised+final)Document48 pagesCleaning+Standards+2021 v1.0+ (Revised+final)ابراهيم الحربيNo ratings yet
- Whooping CoughDocument19 pagesWhooping CoughSalaxar Senpai0% (1)
- Parvus Therapeutics and Ardena Enter Agreement For Tech Transfer, Scale-Up and GMP Manufacturing of Navacim NanoparticlesDocument3 pagesParvus Therapeutics and Ardena Enter Agreement For Tech Transfer, Scale-Up and GMP Manufacturing of Navacim NanoparticlesPR.comNo ratings yet
- ImpetigoDocument16 pagesImpetigokikimasyhurNo ratings yet
- Booster DoseDocument1 pageBooster DoseGouravNo ratings yet
- Abstract PDFDocument36 pagesAbstract PDFDhini Kartika SariNo ratings yet
- Pathogenic Organisms and Virulence FactorsDocument45 pagesPathogenic Organisms and Virulence FactorsqwertNo ratings yet
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Sample Collected atDocument2 pagesD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Sample Collected atAnupam Saraf IINo ratings yet
- Pancawati 1322 1335 1Document14 pagesPancawati 1322 1335 1Hendra Abdul RojakNo ratings yet
- COVID-19 and Mandatory Vaccination: Ethical Considerations and CaveatsDocument5 pagesCOVID-19 and Mandatory Vaccination: Ethical Considerations and CaveatsAngelo Christian B. OreñadaNo ratings yet
- Study of Illness Condition: Assessment Organ Involved Normal Function Pathophysiology AnalysisDocument2 pagesStudy of Illness Condition: Assessment Organ Involved Normal Function Pathophysiology Analysisahmad ryanNo ratings yet