
07-12-2020
07-12-2020
You might also like
- HDFC Ergo Policy Renewal 2023 SelfDocument5 pagesHDFC Ergo Policy Renewal 2023 SelfGopivishnu KanchiNo ratings yet
- A - Level Project Work Insights & ReflectionsDocument3 pagesA - Level Project Work Insights & ReflectionsKou Uraki0% (1)
- Masturbation Free EbookDocument5 pagesMasturbation Free EbookVishal Pandey75% (4)
- IEC 60950 Rev1Document3 pagesIEC 60950 Rev1Rip_BarNo ratings yet
- Introduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesDocument8 pagesIntroduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesManoj Kumar ChaurasiaNo ratings yet
- A Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT ScannersDocument11 pagesA Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT Scannershectorkevin2008No ratings yet
- ISMT 12 - Day 385 - Ravanno - Image Guidance in Minimally Invasive Spinal SurgeryDocument17 pagesISMT 12 - Day 385 - Ravanno - Image Guidance in Minimally Invasive Spinal SurgeryVito MasagusNo ratings yet
- Hand Gesture Recognition With Body Sensor NetworksDocument4 pagesHand Gesture Recognition With Body Sensor NetworksSunil Kumar RNo ratings yet
- Automatic Tracking Measurement System On Human Lumbar Vertebral MotionDocument4 pagesAutomatic Tracking Measurement System On Human Lumbar Vertebral MotionebrahimpanNo ratings yet
- C-Arm Positioning Using Virtual FluorosDocument6 pagesC-Arm Positioning Using Virtual FluorosAna LopezNo ratings yet
- MEdical Robotics PDFDocument22 pagesMEdical Robotics PDFAkhil vNo ratings yet
- Start and End Point Detection of Weightlifting Motion Using CHLAC and MRADocument7 pagesStart and End Point Detection of Weightlifting Motion Using CHLAC and MRArasyoung5302No ratings yet
- 21 Computer Assited Orthopedic Surgery 2003Document7 pages21 Computer Assited Orthopedic Surgery 2003SuzanaPetrovicNo ratings yet
- Fast 5DOF Needle Tracking in iOCTDocument10 pagesFast 5DOF Needle Tracking in iOCTxuedunNo ratings yet
- Measurement MotionTrakkingDocument9 pagesMeasurement MotionTrakkingDiaz Ing ToretoNo ratings yet
- An Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningDocument7 pagesAn Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningInternational Organization of Scientific Research (IOSR)No ratings yet
- Chapter 22 - Computed Tomography Simulation ProceduresDocument30 pagesChapter 22 - Computed Tomography Simulation ProceduresCarlo Gangcuangco ValdezNo ratings yet
- Full Body Motion Capture: A Flexible Marker-Based SolutionDocument8 pagesFull Body Motion Capture: A Flexible Marker-Based Solutionfallenangel006No ratings yet
- Development of A Low Cost Upper Limb Motion Tracking System With Real Time Visual OutputDocument5 pagesDevelopment of A Low Cost Upper Limb Motion Tracking System With Real Time Visual OutputPrit ShahNo ratings yet
- Tracking Human Body Parts Using Particle Filters Constrained by Human BiomechanicsDocument10 pagesTracking Human Body Parts Using Particle Filters Constrained by Human BiomechanicsHamid ShayeghNo ratings yet
- Sensors Management in Robotic Neurosurgery: The ROBOCAST ProjectDocument4 pagesSensors Management in Robotic Neurosurgery: The ROBOCAST Projectsekar_102No ratings yet
- Resume C-ArmDocument4 pagesResume C-Armp27838121011No ratings yet
- The Next White Paper: Ultrasound Fusion ImagingDocument6 pagesThe Next White Paper: Ultrasound Fusion ImagingEl DoNo ratings yet
- Initial Clinical Experiences With The Siremobil Iso-C: Innovative Developments and New MethodsDocument4 pagesInitial Clinical Experiences With The Siremobil Iso-C: Innovative Developments and New MethodsFrancisco DiazNo ratings yet
- Automatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsDocument23 pagesAutomatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsNishant UzirNo ratings yet
- Visual Tracking and Control of A Quadcopter Using PDFDocument8 pagesVisual Tracking and Control of A Quadcopter Using PDFYovi Herlin SaputraNo ratings yet
- Dynamic Navigation For Surgical Implant Placement: Overview of Technology, Key Concepts, and A Case ReportDocument9 pagesDynamic Navigation For Surgical Implant Placement: Overview of Technology, Key Concepts, and A Case Reportreem mohamedNo ratings yet
- A Wearable Motion Capture Device Able To Detect Dynamic Motion of Human LimbsDocument12 pagesA Wearable Motion Capture Device Able To Detect Dynamic Motion of Human LimbsAhmed Gawad ElashryNo ratings yet
- Journal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. AminianDocument6 pagesJournal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. Aminianconstantinescuana200No ratings yet
- Diving Deep Into The Concepts of Dynamic Navigation System in Implant Dentistry A ReviewDocument4 pagesDiving Deep Into The Concepts of Dynamic Navigation System in Implant Dentistry A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Poquet 2013 Comanip Mes RQ PDFDocument8 pagesPoquet 2013 Comanip Mes RQ PDFern_43No ratings yet
- Vascular: Improvement of Functions Supporting Neuro-IVRDocument5 pagesVascular: Improvement of Functions Supporting Neuro-IVRmarcelloairesNo ratings yet
- Journal of Biomedical InformaticsDocument8 pagesJournal of Biomedical InformaticssimonsimoonNo ratings yet
- Robotic Arm Based Automatic Ultrasound Scanning For Three-Dimensional ImagingDocument10 pagesRobotic Arm Based Automatic Ultrasound Scanning For Three-Dimensional ImagingAshish Presanna ChandranNo ratings yet
- Seminario 6. Implant Placement Accuracy Using Dynamic NavigationDocument8 pagesSeminario 6. Implant Placement Accuracy Using Dynamic NavigationLenny GrauNo ratings yet
- 20-2007 - Kadoury Et AlDocument12 pages20-2007 - Kadoury Et AlJuan Pablo Romero CamposNo ratings yet
- Appli Pleno IshizakaDocument5 pagesAppli Pleno IshizakaFazaia KckNo ratings yet
- Wang 2009Document11 pagesWang 2009Tuan PhanNo ratings yet
- Jomi 5004Document8 pagesJomi 5004Fernando Ari del CorroNo ratings yet
- Navigation in Minimally Invasive Spine Surgery: Sohrab Virk, Sheeraz QureshiDocument6 pagesNavigation in Minimally Invasive Spine Surgery: Sohrab Virk, Sheeraz QureshiliuyonglogNo ratings yet
- Marker-Free Model Reconstruction and Motion Tracking From 3D Voxel DataDocument10 pagesMarker-Free Model Reconstruction and Motion Tracking From 3D Voxel DataCyrille LamasséNo ratings yet
- Quality Assurance For Image-Guided Radiation Therapy Utilizing CT-basedDocument18 pagesQuality Assurance For Image-Guided Radiation Therapy Utilizing CT-based2016508吳翊晨No ratings yet
- Intelligent X-Ray Based Training System For Pedicle Screw Placement in Lumbar VertebraeDocument7 pagesIntelligent X-Ray Based Training System For Pedicle Screw Placement in Lumbar VertebraeCatalina Sorina ParfeneNo ratings yet
- Sensors 15 02181Document24 pagesSensors 15 02181Alice AmaratyaNo ratings yet
- 2015 - Towards-a-Robotic-Knee-Exoskeleton-Control-Based-on-Human Intention Through EEG and sEMGsignalsDocument8 pages2015 - Towards-a-Robotic-Knee-Exoskeleton-Control-Based-on-Human Intention Through EEG and sEMGsignalsArun KumarNo ratings yet
- Depth Invariant Visual Servoing: Peter A. Karasev, Miguel Moises Serrano, Patricio A. Vela, and Allen TannenbaumDocument7 pagesDepth Invariant Visual Servoing: Peter A. Karasev, Miguel Moises Serrano, Patricio A. Vela, and Allen Tannenbaumzhero7No ratings yet
- A Novel 3D-Vision-Based Collaborative Robot As A Scope Holding System For Port Surgery - A Technical Feasibility StudyDocument8 pagesA Novel 3D-Vision-Based Collaborative Robot As A Scope Holding System For Port Surgery - A Technical Feasibility StudySunny XiongNo ratings yet
- Implant Placement Accuracy Using Dynamic NavigationDocument9 pagesImplant Placement Accuracy Using Dynamic NavigationMrinmayee ThakurNo ratings yet
- Virtual Liver BiopsyDocument10 pagesVirtual Liver Biopsyajaykavitha213No ratings yet
- Dynamic Measurement of Lumbar Curvature Using Fibre-Optic SensorsDocument7 pagesDynamic Measurement of Lumbar Curvature Using Fibre-Optic SensorsebrahimpanNo ratings yet
- Vidal Etal Icra2006Document7 pagesVidal Etal Icra2006madupiz@gmailNo ratings yet
- 3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic ModelingDocument9 pages3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic ModelingCristian HoyNo ratings yet
- Cirugia Asistida Por ComputadoraDocument18 pagesCirugia Asistida Por ComputadoraPaola Alexandra LaguadoNo ratings yet
- Real-Time Human Motion Tracking Using Multiple Depth CamerasDocument7 pagesReal-Time Human Motion Tracking Using Multiple Depth CamerasRishabhRoyNo ratings yet
- CH 3Document21 pagesCH 3Mohamed AhmedNo ratings yet
- 18-2007 - Kadoury Et AlDocument8 pages18-2007 - Kadoury Et AlJuan Pablo Romero CamposNo ratings yet
- Real-Time Tracking of Guidewire Robot Tips Using Deep Convolutional Neural Networks On Successive Localized FramesDocument11 pagesReal-Time Tracking of Guidewire Robot Tips Using Deep Convolutional Neural Networks On Successive Localized FramesNishant UzirNo ratings yet
- CH 4Document12 pagesCH 4Mohamed AhmedNo ratings yet
- Real-Time Full-Body Motion Capture From Video and ImusDocument9 pagesReal-Time Full-Body Motion Capture From Video and ImusPAL ROBOTNo ratings yet
- Three-Dimensional Navigation-Guided Percutaneous Screw Fixation For Nondisplaced and Displaced Pelvi-Acetabular Fractures in A Major Trauma CentreDocument9 pagesThree-Dimensional Navigation-Guided Percutaneous Screw Fixation For Nondisplaced and Displaced Pelvi-Acetabular Fractures in A Major Trauma CentrePierre MartzNo ratings yet
- Sensors 21 02927Document16 pagesSensors 21 02927Ashish Presanna ChandranNo ratings yet
- Markerless Human Motion Capture Through Visual Hull and Articulated ICPDocument5 pagesMarkerless Human Motion Capture Through Visual Hull and Articulated ICPCyrille LamasséNo ratings yet
- Virtual SurgeryDocument22 pagesVirtual SurgeryMounika Surapaneni100% (1)
- Augmented Reality Assisted Surgery: Enhancing Surgical Precision through Computer VisionFrom EverandAugmented Reality Assisted Surgery: Enhancing Surgical Precision through Computer VisionNo ratings yet
- Optical Flow: Exploring Dynamic Visual Patterns in Computer VisionFrom EverandOptical Flow: Exploring Dynamic Visual Patterns in Computer VisionNo ratings yet
- Academy of American Franciscan HistoryDocument36 pagesAcademy of American Franciscan HistoryCESAR HUAROTO DE LA CRUZNo ratings yet
- The Winnipeg Foundation 2014 Annual ReportDocument76 pagesThe Winnipeg Foundation 2014 Annual ReportChrisDcaNo ratings yet
- Parental/Guardian Permission and Liability Waiver Name of Student BirthDocument2 pagesParental/Guardian Permission and Liability Waiver Name of Student BirthlifeteenministryNo ratings yet
- Electrical Commissioning Checklist Non LeedDocument7 pagesElectrical Commissioning Checklist Non Leedcaleb isukuruNo ratings yet
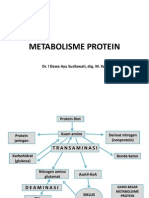
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Chemistry Chapter 1.exercise 1ADocument28 pagesChemistry Chapter 1.exercise 1AAsifNo ratings yet
- URL #Flushyourmeds Scott BarryDocument8 pagesURL #Flushyourmeds Scott Barryurl-flushyourmedsNo ratings yet
- Thermolator Heatrac User GuideDocument98 pagesThermolator Heatrac User GuideValeria SarahiNo ratings yet
- VBIED Attack July 31, 2007Document1 pageVBIED Attack July 31, 2007Rhonda NoldeNo ratings yet
- Module 7: Health Care Delivery SystemDocument9 pagesModule 7: Health Care Delivery SystemDanz KieNo ratings yet
- Ensuring Safety and Cleanliness in The SalonDocument21 pagesEnsuring Safety and Cleanliness in The SalonMa Christina Encinas83% (6)
- Department of Education: Learning Activity SheetDocument7 pagesDepartment of Education: Learning Activity SheetKaren May UrlandaNo ratings yet
- Lecture 6Document32 pagesLecture 6Nilesh PanchalNo ratings yet
- A Study On Occupational Hazards in Die Casting IndustriesDocument8 pagesA Study On Occupational Hazards in Die Casting IndustriesManik LakshmanNo ratings yet
- Starkville Dispatch Eedition 7-29-20Document16 pagesStarkville Dispatch Eedition 7-29-20The DispatchNo ratings yet
- Training - Cga ApplicationDocument34 pagesTraining - Cga ApplicationSubhan Muhammad100% (1)
- Women Mental Health:: Postpartum DepressionDocument62 pagesWomen Mental Health:: Postpartum DepressionTickablingbling Alwaysshine Likeatenglarious100% (1)
- Generator Automatic Voltage Regulator Operation ManualDocument6 pagesGenerator Automatic Voltage Regulator Operation ManualMahdi DehghankarNo ratings yet
- Toothpaste Survey FormDocument1 pageToothpaste Survey FormBimalendu Konar50% (2)
- NG Gan Zee Vs Asian CrusaderDocument3 pagesNG Gan Zee Vs Asian CrusaderWatz RebanalNo ratings yet
- Seed Extraction MethodsDocument3 pagesSeed Extraction MethodsPreetam NayakNo ratings yet
- SRHR - FGD With Young PeopleDocument3 pagesSRHR - FGD With Young PeopleMandira PrakashNo ratings yet
- Anthe Junior Sample Paper Class IXDocument14 pagesAnthe Junior Sample Paper Class IXMota Chashma85% (62)
- Bence Bays Resume July 2015Document2 pagesBence Bays Resume July 2015api-292242662No ratings yet
- Mother's Personality and Its Interaction With Child Temperament As Predictors of Parenting BehaviorDocument12 pagesMother's Personality and Its Interaction With Child Temperament As Predictors of Parenting BehaviorMichelle PajueloNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- HDFC Ergo Policy Renewal 2023 SelfDocument5 pagesHDFC Ergo Policy Renewal 2023 SelfGopivishnu KanchiNo ratings yet
- A - Level Project Work Insights & ReflectionsDocument3 pagesA - Level Project Work Insights & ReflectionsKou Uraki0% (1)
- Masturbation Free EbookDocument5 pagesMasturbation Free EbookVishal Pandey75% (4)
- IEC 60950 Rev1Document3 pagesIEC 60950 Rev1Rip_BarNo ratings yet
- Introduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesDocument8 pagesIntroduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesManoj Kumar ChaurasiaNo ratings yet
- A Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT ScannersDocument11 pagesA Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT Scannershectorkevin2008No ratings yet
- ISMT 12 - Day 385 - Ravanno - Image Guidance in Minimally Invasive Spinal SurgeryDocument17 pagesISMT 12 - Day 385 - Ravanno - Image Guidance in Minimally Invasive Spinal SurgeryVito MasagusNo ratings yet
- Hand Gesture Recognition With Body Sensor NetworksDocument4 pagesHand Gesture Recognition With Body Sensor NetworksSunil Kumar RNo ratings yet
- Automatic Tracking Measurement System On Human Lumbar Vertebral MotionDocument4 pagesAutomatic Tracking Measurement System On Human Lumbar Vertebral MotionebrahimpanNo ratings yet
- C-Arm Positioning Using Virtual FluorosDocument6 pagesC-Arm Positioning Using Virtual FluorosAna LopezNo ratings yet
- MEdical Robotics PDFDocument22 pagesMEdical Robotics PDFAkhil vNo ratings yet
- Start and End Point Detection of Weightlifting Motion Using CHLAC and MRADocument7 pagesStart and End Point Detection of Weightlifting Motion Using CHLAC and MRArasyoung5302No ratings yet
- 21 Computer Assited Orthopedic Surgery 2003Document7 pages21 Computer Assited Orthopedic Surgery 2003SuzanaPetrovicNo ratings yet
- Fast 5DOF Needle Tracking in iOCTDocument10 pagesFast 5DOF Needle Tracking in iOCTxuedunNo ratings yet
- Measurement MotionTrakkingDocument9 pagesMeasurement MotionTrakkingDiaz Ing ToretoNo ratings yet
- An Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningDocument7 pagesAn Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningInternational Organization of Scientific Research (IOSR)No ratings yet
- Chapter 22 - Computed Tomography Simulation ProceduresDocument30 pagesChapter 22 - Computed Tomography Simulation ProceduresCarlo Gangcuangco ValdezNo ratings yet
- Full Body Motion Capture: A Flexible Marker-Based SolutionDocument8 pagesFull Body Motion Capture: A Flexible Marker-Based Solutionfallenangel006No ratings yet
- Development of A Low Cost Upper Limb Motion Tracking System With Real Time Visual OutputDocument5 pagesDevelopment of A Low Cost Upper Limb Motion Tracking System With Real Time Visual OutputPrit ShahNo ratings yet
- Tracking Human Body Parts Using Particle Filters Constrained by Human BiomechanicsDocument10 pagesTracking Human Body Parts Using Particle Filters Constrained by Human BiomechanicsHamid ShayeghNo ratings yet
- Sensors Management in Robotic Neurosurgery: The ROBOCAST ProjectDocument4 pagesSensors Management in Robotic Neurosurgery: The ROBOCAST Projectsekar_102No ratings yet
- Resume C-ArmDocument4 pagesResume C-Armp27838121011No ratings yet
- The Next White Paper: Ultrasound Fusion ImagingDocument6 pagesThe Next White Paper: Ultrasound Fusion ImagingEl DoNo ratings yet
- Initial Clinical Experiences With The Siremobil Iso-C: Innovative Developments and New MethodsDocument4 pagesInitial Clinical Experiences With The Siremobil Iso-C: Innovative Developments and New MethodsFrancisco DiazNo ratings yet
- Automatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsDocument23 pagesAutomatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsNishant UzirNo ratings yet
- Visual Tracking and Control of A Quadcopter Using PDFDocument8 pagesVisual Tracking and Control of A Quadcopter Using PDFYovi Herlin SaputraNo ratings yet
- Dynamic Navigation For Surgical Implant Placement: Overview of Technology, Key Concepts, and A Case ReportDocument9 pagesDynamic Navigation For Surgical Implant Placement: Overview of Technology, Key Concepts, and A Case Reportreem mohamedNo ratings yet
- A Wearable Motion Capture Device Able To Detect Dynamic Motion of Human LimbsDocument12 pagesA Wearable Motion Capture Device Able To Detect Dynamic Motion of Human LimbsAhmed Gawad ElashryNo ratings yet
- Journal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. AminianDocument6 pagesJournal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. Aminianconstantinescuana200No ratings yet
- Diving Deep Into The Concepts of Dynamic Navigation System in Implant Dentistry A ReviewDocument4 pagesDiving Deep Into The Concepts of Dynamic Navigation System in Implant Dentistry A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Poquet 2013 Comanip Mes RQ PDFDocument8 pagesPoquet 2013 Comanip Mes RQ PDFern_43No ratings yet
- Vascular: Improvement of Functions Supporting Neuro-IVRDocument5 pagesVascular: Improvement of Functions Supporting Neuro-IVRmarcelloairesNo ratings yet
- Journal of Biomedical InformaticsDocument8 pagesJournal of Biomedical InformaticssimonsimoonNo ratings yet
- Robotic Arm Based Automatic Ultrasound Scanning For Three-Dimensional ImagingDocument10 pagesRobotic Arm Based Automatic Ultrasound Scanning For Three-Dimensional ImagingAshish Presanna ChandranNo ratings yet
- Seminario 6. Implant Placement Accuracy Using Dynamic NavigationDocument8 pagesSeminario 6. Implant Placement Accuracy Using Dynamic NavigationLenny GrauNo ratings yet
- 20-2007 - Kadoury Et AlDocument12 pages20-2007 - Kadoury Et AlJuan Pablo Romero CamposNo ratings yet
- Appli Pleno IshizakaDocument5 pagesAppli Pleno IshizakaFazaia KckNo ratings yet
- Wang 2009Document11 pagesWang 2009Tuan PhanNo ratings yet
- Jomi 5004Document8 pagesJomi 5004Fernando Ari del CorroNo ratings yet
- Navigation in Minimally Invasive Spine Surgery: Sohrab Virk, Sheeraz QureshiDocument6 pagesNavigation in Minimally Invasive Spine Surgery: Sohrab Virk, Sheeraz QureshiliuyonglogNo ratings yet
- Marker-Free Model Reconstruction and Motion Tracking From 3D Voxel DataDocument10 pagesMarker-Free Model Reconstruction and Motion Tracking From 3D Voxel DataCyrille LamasséNo ratings yet
- Quality Assurance For Image-Guided Radiation Therapy Utilizing CT-basedDocument18 pagesQuality Assurance For Image-Guided Radiation Therapy Utilizing CT-based2016508吳翊晨No ratings yet
- Intelligent X-Ray Based Training System For Pedicle Screw Placement in Lumbar VertebraeDocument7 pagesIntelligent X-Ray Based Training System For Pedicle Screw Placement in Lumbar VertebraeCatalina Sorina ParfeneNo ratings yet
- Sensors 15 02181Document24 pagesSensors 15 02181Alice AmaratyaNo ratings yet
- 2015 - Towards-a-Robotic-Knee-Exoskeleton-Control-Based-on-Human Intention Through EEG and sEMGsignalsDocument8 pages2015 - Towards-a-Robotic-Knee-Exoskeleton-Control-Based-on-Human Intention Through EEG and sEMGsignalsArun KumarNo ratings yet
- Depth Invariant Visual Servoing: Peter A. Karasev, Miguel Moises Serrano, Patricio A. Vela, and Allen TannenbaumDocument7 pagesDepth Invariant Visual Servoing: Peter A. Karasev, Miguel Moises Serrano, Patricio A. Vela, and Allen Tannenbaumzhero7No ratings yet
- A Novel 3D-Vision-Based Collaborative Robot As A Scope Holding System For Port Surgery - A Technical Feasibility StudyDocument8 pagesA Novel 3D-Vision-Based Collaborative Robot As A Scope Holding System For Port Surgery - A Technical Feasibility StudySunny XiongNo ratings yet
- Implant Placement Accuracy Using Dynamic NavigationDocument9 pagesImplant Placement Accuracy Using Dynamic NavigationMrinmayee ThakurNo ratings yet
- Virtual Liver BiopsyDocument10 pagesVirtual Liver Biopsyajaykavitha213No ratings yet
- Dynamic Measurement of Lumbar Curvature Using Fibre-Optic SensorsDocument7 pagesDynamic Measurement of Lumbar Curvature Using Fibre-Optic SensorsebrahimpanNo ratings yet
- Vidal Etal Icra2006Document7 pagesVidal Etal Icra2006madupiz@gmailNo ratings yet
- 3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic ModelingDocument9 pages3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic ModelingCristian HoyNo ratings yet
- Cirugia Asistida Por ComputadoraDocument18 pagesCirugia Asistida Por ComputadoraPaola Alexandra LaguadoNo ratings yet
- Real-Time Human Motion Tracking Using Multiple Depth CamerasDocument7 pagesReal-Time Human Motion Tracking Using Multiple Depth CamerasRishabhRoyNo ratings yet
- CH 3Document21 pagesCH 3Mohamed AhmedNo ratings yet
- 18-2007 - Kadoury Et AlDocument8 pages18-2007 - Kadoury Et AlJuan Pablo Romero CamposNo ratings yet
- Real-Time Tracking of Guidewire Robot Tips Using Deep Convolutional Neural Networks On Successive Localized FramesDocument11 pagesReal-Time Tracking of Guidewire Robot Tips Using Deep Convolutional Neural Networks On Successive Localized FramesNishant UzirNo ratings yet
- CH 4Document12 pagesCH 4Mohamed AhmedNo ratings yet
- Real-Time Full-Body Motion Capture From Video and ImusDocument9 pagesReal-Time Full-Body Motion Capture From Video and ImusPAL ROBOTNo ratings yet
- Three-Dimensional Navigation-Guided Percutaneous Screw Fixation For Nondisplaced and Displaced Pelvi-Acetabular Fractures in A Major Trauma CentreDocument9 pagesThree-Dimensional Navigation-Guided Percutaneous Screw Fixation For Nondisplaced and Displaced Pelvi-Acetabular Fractures in A Major Trauma CentrePierre MartzNo ratings yet
- Sensors 21 02927Document16 pagesSensors 21 02927Ashish Presanna ChandranNo ratings yet
- Markerless Human Motion Capture Through Visual Hull and Articulated ICPDocument5 pagesMarkerless Human Motion Capture Through Visual Hull and Articulated ICPCyrille LamasséNo ratings yet
- Virtual SurgeryDocument22 pagesVirtual SurgeryMounika Surapaneni100% (1)
- Augmented Reality Assisted Surgery: Enhancing Surgical Precision through Computer VisionFrom EverandAugmented Reality Assisted Surgery: Enhancing Surgical Precision through Computer VisionNo ratings yet
- Optical Flow: Exploring Dynamic Visual Patterns in Computer VisionFrom EverandOptical Flow: Exploring Dynamic Visual Patterns in Computer VisionNo ratings yet
- Academy of American Franciscan HistoryDocument36 pagesAcademy of American Franciscan HistoryCESAR HUAROTO DE LA CRUZNo ratings yet
- The Winnipeg Foundation 2014 Annual ReportDocument76 pagesThe Winnipeg Foundation 2014 Annual ReportChrisDcaNo ratings yet
- Parental/Guardian Permission and Liability Waiver Name of Student BirthDocument2 pagesParental/Guardian Permission and Liability Waiver Name of Student BirthlifeteenministryNo ratings yet
- Electrical Commissioning Checklist Non LeedDocument7 pagesElectrical Commissioning Checklist Non Leedcaleb isukuruNo ratings yet
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Chemistry Chapter 1.exercise 1ADocument28 pagesChemistry Chapter 1.exercise 1AAsifNo ratings yet
- URL #Flushyourmeds Scott BarryDocument8 pagesURL #Flushyourmeds Scott Barryurl-flushyourmedsNo ratings yet
- Thermolator Heatrac User GuideDocument98 pagesThermolator Heatrac User GuideValeria SarahiNo ratings yet
- VBIED Attack July 31, 2007Document1 pageVBIED Attack July 31, 2007Rhonda NoldeNo ratings yet
- Module 7: Health Care Delivery SystemDocument9 pagesModule 7: Health Care Delivery SystemDanz KieNo ratings yet
- Ensuring Safety and Cleanliness in The SalonDocument21 pagesEnsuring Safety and Cleanliness in The SalonMa Christina Encinas83% (6)
- Department of Education: Learning Activity SheetDocument7 pagesDepartment of Education: Learning Activity SheetKaren May UrlandaNo ratings yet
- Lecture 6Document32 pagesLecture 6Nilesh PanchalNo ratings yet
- A Study On Occupational Hazards in Die Casting IndustriesDocument8 pagesA Study On Occupational Hazards in Die Casting IndustriesManik LakshmanNo ratings yet
- Starkville Dispatch Eedition 7-29-20Document16 pagesStarkville Dispatch Eedition 7-29-20The DispatchNo ratings yet
- Training - Cga ApplicationDocument34 pagesTraining - Cga ApplicationSubhan Muhammad100% (1)
- Women Mental Health:: Postpartum DepressionDocument62 pagesWomen Mental Health:: Postpartum DepressionTickablingbling Alwaysshine Likeatenglarious100% (1)
- Generator Automatic Voltage Regulator Operation ManualDocument6 pagesGenerator Automatic Voltage Regulator Operation ManualMahdi DehghankarNo ratings yet
- Toothpaste Survey FormDocument1 pageToothpaste Survey FormBimalendu Konar50% (2)
- NG Gan Zee Vs Asian CrusaderDocument3 pagesNG Gan Zee Vs Asian CrusaderWatz RebanalNo ratings yet
- Seed Extraction MethodsDocument3 pagesSeed Extraction MethodsPreetam NayakNo ratings yet
- SRHR - FGD With Young PeopleDocument3 pagesSRHR - FGD With Young PeopleMandira PrakashNo ratings yet
- Anthe Junior Sample Paper Class IXDocument14 pagesAnthe Junior Sample Paper Class IXMota Chashma85% (62)
- Bence Bays Resume July 2015Document2 pagesBence Bays Resume July 2015api-292242662No ratings yet
- Mother's Personality and Its Interaction With Child Temperament As Predictors of Parenting BehaviorDocument12 pagesMother's Personality and Its Interaction With Child Temperament As Predictors of Parenting BehaviorMichelle PajueloNo ratings yet